Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
|
To which parts of the gut are the dorsal and ventral messentries attached?
|
The entire primitive gut is attached to the posterior body wall of the embryo by a dorsal messentry. Only the foregut is connected by a ventral messentry to the ant. body wall. Th
|
|
|
What tissue does the endoderm form?
|
Lining for the digestive tract, secretory cells of the glands that open into the GI tract.
|
|
|
What tissue does the mesoderm form?
|
smooth muscle, connective tissue and blood vessels
|
|
|
The vitellin duct is connected to the area that will form ....? What happens if it doesn't close?
|
The terminal part of the illeum.
- meckel's diverticulum - vitelline cyst (closes at proximal and distal ends but stays open in middle) - vitteline fistula (stays completely open and illum communicates with umbilicus |
|
|
Where do other (non-vittelin) cysts and diverticulae arise from?
|
Incomplete separation of the endoderm and the notocord
|
|
|
The foregut gives rise to what 5 things?
|
- respiratory tree (larynx --> alveoli)
- esophagus -stomach - liver, gallbladder & pancrease - duodenum as far as the entrance to the common bile duct |
|
|
What are the 5 critical events in the formation of the foregut?
|
1. Formation of the laryngeaotracheal diverticulum
2. Gastric dilation 3. Elongation of esophagus (moves the stomach into the abdomen) 4. Occlusion of the foregut (proximal and distal to the gastric dilation) by endoderm - acts as pulgs, gastric cavity fills and expands) 5. Recanalization of the foregut (programmed cell death) |
|
|
List 2 critical events in the formation of the stomach.
|
1. Rotation of the stomach to the left (dorsal messentry becomes the greater omentum and the ventral messentry becomes coverings of the liver and it's ligaments)
2. Faster growth along one border creates the greater curvature |
|
|
What 4 things does the midgut develop into?
|
- the res of the duodenum
- the jejunum and illeum - the cecum and appendix - the ascending colon and part of the transverse ( ie those parts supplied by the superior mesenteric artery) |
|
|
What are the 3 main critical events in the formation of the midgut?
|
1. the elongation and physiologic herniation of the midgut into the umbilical cavity
2. Further elongation and rotation of 90deg to the R of the fetus 3. Return of the midgut into the abdominal cavity |
|
|
What are 4 common abnormalities of midgut development?
|
- malrotation: appendix on L
- Omphalocele: failure to return, intestines in umbilical cord - gastroschisis: rupture in the ant. body wall (usually on R of umbillical cord). These intestines aren't covered and float freely in amniotic cavity) - Umbilical hernia: caused by delayed closure of the umbilical ring |
|
|
The hindgut gives rise to what? (5)
|
- distal transverse colon
- descending colon - sigmoid colon - rectum - upper part of anal canal |
|
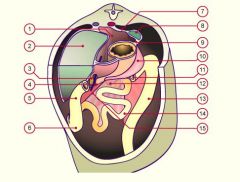
Identify the structures
|
1.Omental bursa
2.Liver 3.Gall bladder 4.Duodenum 5Ascending colon 6Cecum 7Lienorenal ligament 8Spleen 9. Gastrolienal ligament 10. Greater omentum 11.Transverse colon 12.Mesenterium 13. Descending colon 14. Small intestine convolution 15. Root of the mesentery |
|
|
What layer does the pancreas come from?
|
the distal part of the foregut
|
|

|

1 - foregut
3 - lung buds 4 - dorsal pancrease 5- stomach 6 midgut 7 hindgut |
|
|
The urorectal septum partitions the cloacal membrane into:
1. ______ 2. ______ What do they become? |
1. Urogenital sinus (bladder & urethra)
2. Rectoanal canal (the rectum and the upper part of the anal canal) |
|

Identify the structures
|
1- foregut
3 - lung buds 4 - stomach 5 - dorsal pancreas 6 - mid gut 7- hindgut |
|
|
The proctodeum becomes what?
|
The distal anal canal ("anal valves")
Has a different blood supply and innervation |
|
|
What are the 2 main causes of imperforate anus (what happens?)
|
1. Urorectal septum deviates and grows too close to posterior wall causing anal stenosis.
2. Urorectal septum fuses with posterior wall = anal atresia |
|
|
What causes fistulas between the urinary and fecal tracts?
|
The urorectal septum is divided into 2 parts, and if these two parts fail to fuse you get fistulas.
|
|
|
An outgrowth into the ventral messentry produces what 3 structures?
|
- Liver (the mesoderm of the septum transversum is reduce to contibution to the liver)
- gall bladder - pancreas |
|
|
How does the pancreas form?
|
Starts as dorsal and ventral buds. Rotation of the gut combined with differential growth rates force the two together. (Ventral bud spins round to join dorsal)
|
|
|
Why do some people have an accessory pancreatic duct?
|
B/c the duct of the ventral pancreatic bud can sometimes persist
|
|
|
Where does the diaphragm come from ( 3 sources)? Why can babies get hernias?
|
- dorsal messentry
- septum transversum - pleuroperitoneal folds (outgrowths of body wall) * if folds don't grow fast enough gut will herniate into thorax when it returns from umbillicus |
|
|
What are the 4 signs of a GI obstruction in a newborn? Which sign will help you distinguish an upper obstruction from a lower?
|
- distention proximally (and atrophy distally - use it or loose it!)
- reduced stool output - vomitting: projectile and clear emesis if upper, normal and bile-stained if lower - polyhydraminos |
|
|
What are the 8 causes of an obstruction:
- failure to.. - persistence of - wayward growth of 2 things... - congenital condition - 2 probs with intest |
- failure to recanalize esophagus (no apoptosis)
- Congenital membranous atresia (persistent cloacal membrane) - Imperforate anus (stenosed or atresia from urorectal septum) - Congenital hypertrophic pyloric sphincter - a ring of pancreas around the duodenum (from persistance of multiple pancreatic buds) - congenital volvulus (twisted bowel) - intussusception (telescopes in on itself) |
|
|
What source of obstruction is common in babies with CF?
|
Meconium ileus - impaction with mecunium b/c it is too viscous
|
|
|
What is the tissue source (ie embryonic layer) of the kidneys and the ureters?
|
the intermediate mesoderm.
|
|
|
Discuss the formation of the mesonephric duct:
1. nephrogenic cord (something forms) 2. somethings will ..... forming the ........ duct 3. the duct will .... 4. the top part of the duct will..... and the rest will........ |
1. Vesicles form in nephrogenic cord opposite cervical segments
2. vesicles fuse forming the pronephric duct 3. the duct grows to sacral end of embyo eventually opening into cloaca 4. the cervical part of the cord degenerate and remainder of the duct is now the mesonephric duct |
|
|
The uteric bud will form what?
The metanephric mass of mesoderm will form what else? |
- bud: calices, pelvis, ureters
- mass: parenchyma of kidney |
|
|
Describe messages being sent in reciprocal signalling:
1. mass --> bud 2. bud --> mass 3. mass--> bud 4. bud ---> mass |
1. Grow towards me!
2. survive while the rest of duct dissolves 3. divide into branches 4. make tubercules |
|
|
How do nephrons form from a uteric bud sitting in a cap of metanephric tissue?
|
Vesicles form in metanephric tissue. They elongate, (produce urine) then fuse with bud.
|
|
|
Describe the "ascent of the kidneys" (where do they start from? How do they stay alive as they climb?)
|
They develop near the sacral segments of the spine, with pelvis facing anteriorly. The climb and rotate medially. As they climb kidneys will attach to higher arteries and release lower ones (this is how accessory arteries can develop).
|
|
|
What are the 3 abnormalities that can interrupt kidney ascent?
|
accessory arteries
ectopic kidneys (benin if congenital, if acquire - ie kidney falls from sudden loss of fat - then will kink ureter closed) fused kidneys (b/c nephrogenic cords merged) |
|
|
What can happen from abnormal interactions of ureteric bud (off mesonephric duct) and the metanephric mass?
|
1. bifid ureter - if bud branches before reaching mass (or supernumerary)
2. crossed ectopic - if bud crosses midline and merges with mass on the other side - both kidneys on same side |
|
|
If the uteric buds fail to interact what condition results?
What are the 4 symptoms? What causes them? |
Renal agenesis - no kidneys!
Causes Potter's Facies Oligohydraminos: squishes the baby and causes - flattened profile - flexion contractures - pulmonary hypoplasia (no fluid to breath) - small chest |
|
|
Describe the:
- length of fibers - location of nuclei - connection of cells of Cardiac cells |
- short and branched
- 1 or 2 nucleus in centre of cell - connected via gap junctions in intercalated disks |
|
|
Describe the:
- length of fibers - location of nuclei - connection of cells of Skeletal cells |
- long and straight
- multi-nucleated (nucleus at periph) - isolated - each cell has own neuro-muscular junction |