![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
6 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
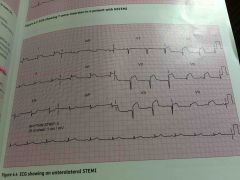
Anterior or anteroseptal infarction Leads V1-V4 Extension to involve leads V5-V6, I and aVL |
Typically caused by a lesion in the left anterior descending (LAD) coronary artery |
|
|
|
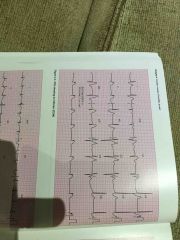
Inferior infarction Leads II, III and aVF |
Caused often by a lesion in right coronary artery or, less commonly, the circumflex artery |
|
|
|
Lateral infarction Leads V5-V6 and / or leads I and aVL (sometimes aVL alone) |
Caused usually by a lesion in the circumflex artery or diagonal branch of the LAD artery |
|
|
|
Posterior myocardial infarction Recognised when there is reciprocal ST-segment depression in the anterior chest leads ST-segment depression in the leads may reflect posterior ST-segment elevation, and development of a dominant R wave in V1 and V2 reflects posterior Q wave development |
Most commonly due to a right coronary artery occlusion but may be caused by a dominant circumflex artery lesions in individuals in whom the artery provides the main blood supply to the posterior part of the left ventricle and septum. |
|
|
|
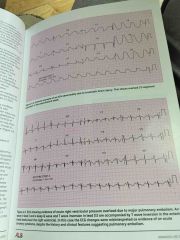
Right ventricular (RV) infarction may be present in up to 1/3 of patients with inferior and posterior STEMI. Extensive RV infarction may be seen in a conventional ECG when ST - segment elevation in lead V1 accompanies an inferior or posterior STEMI |
A diagnosis of extensive RV infarction is suggested by fluid - responsive hypotension and signs of high systemic venous pressure (manifest as jugular venous distension) without pulmonary congestion |
|
|
|
The ST - segment depression and T - wave inversion that may occur in NSTEMI are less clearly related to the site of myocardial damage than the changes in STEMI |
Acute ECG abnormalities may be caused by conditions other than ACS. The ECGs of some people with Subarachnoid haemorrhage or Traumatic brain injury may show acute changes including ST - segment depression or elevation, or T - wave inversion |
|