![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
71 Cards in this Set
- Front
- Back
|
Hearing loss from the external/middle ear that is the result of obstruction, mass loading, stiffness effect, and discontinuity. |
Conductive Hearing Loss |
|
|
Hearing loss due to cochlea deterioration. |
Sensory Hearing Loss |
|
|
Hearing loss due to lesions on or impairment of acoustic nerve (CN VIII), auditory nuclei, ascending tracts, auditory cortex. |
Neural Hearing Loss |
|
This is an example of |
What a cockroach hides behind (kidding...made you smile or shiver though)... Cerumen impaction potentially causing conductive hearing loss |
|
|
A vibrating tuning fork is placed a top a Pt's head. Pt indicates they hear it in the ear that they couldn't hear the whisper in. What is this an example of and what is the test called? |
Lateralization to bad ear indicating conductive hearing loss. Weber Test |
|
|
If the Pt hears the tuning fork atop their head in the ear they could hear the whisper in, what is that an example of? |
Lateralization to the good ear indicating sensorineural hearing loss. |
|
|
The Pt hears the vibrating tuning fork atop their head in both ears. What is the significance? |
Pt has a negative Weber Test and demonstrates no hearing loss. |
|
|
The Pt has a vibrating tuning fork placed behind their ear, then indicates they can no longer hear the sound and it is placed in front of their ear. The Pt indicates they CANNOT hear the vibration in front of their ear. Where, specifically, is the tuning fork being placed at the beginning of the test? What is the significance of the findings? What is the name of the test? |
|
|
|
The Pt has a vibrating tuning fork placed behind their ear, then indicates they can no longer hear the sound and it is placed in front of their ear. The Pt indicates they CAN hear the vibration in front of their ear. What is the significance? |
AC>BC = Negative Rinne Test (no hearing loss) |
|
|
You perform the Whisper, Weber, and Rinne tests on your Pt. The were positive on all three tests. What is your next step and why? |
Pt should be referred to an ENT or an Audiologist for Pure-tone Audiometry to confirm the type(s) of hearing loss they have and to determine at what Hz ranges they have hearing loss. Once those determinations are made, the ENT or Audiologist can make additional Tx/management recommendations for the Pt. |
|
|
Normal hearing loss is what vocal and dB equivalents? |
Soft whisper & 0-20dB |
|
|
Mild hearing loss is what vocal and dB equivalents? |
Soft spoken voice & 20-40 dB |
|
|
40-60 dB is a normal spoken voice. What is the hearing loss classification associated with that? |
Moderate hearing loss |
|
|
60-80 dB is a loud spoken voice. If you are unable to hear that, what is the hearing loss classification? |
Severe hearing loss |
|
|
Profound hearing loss means you are unable to hear someone shouting at you. What is the decibel range associated with that? |
>80 dB |
|

This Pt's CC = Otalgia. The Pt tells you that she just needed to use q-tips to clean her ears and that the amber d/c was wax. What is your Dx and what PE will r/in or r/o? |
Dx: Otitis Externa Physical Exams: Palpate Pinna + Tug Test = Pinna s/b sore/tender; Otoscopic examination = Edema & erythema of ear canal, d/c should look granular (dried purulent exudate vs sticky cerumen), may even see evidence of fresh purulent d/c proximal to TM |
|

Otoscopic examination reveals this. What is the likely causative bacteria? What would you prefer to Tx with? |
Pseudomonas or other Gram Neg Rods Abx drops: fluoroquinolones |
|
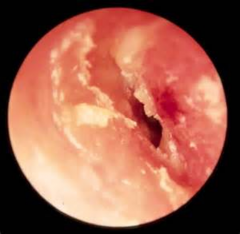
What are the risk factors for contracting this infxn? |
Recent water exposure (esp. in a community pool or lake) Mechanical trauma (scratching with foreign object) |
|

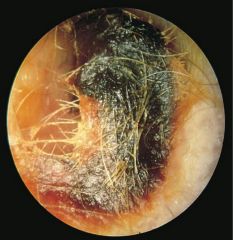
Otoscopic examination reveals this. What is this and how is it different? |
This is an otitis externa caused by aspergillus fungi. Tx requires antifungal drops. |
|
|
What Dz prevention counsel would you provide to a Pt that presented with Otitis Externa? |
Counsel them to:
alcohol/viengar) after participating in water activities |
|
|
Your Pt is immunocompromised and has a persistent Otitis Externa infxn. What is concerning about this? |
It could develop into Osteomyelitis (Malignant external otitis) which is a spread of the infxn into the skull base. |
|
|
In addition to fluoroquinolone drops, what else can be used to Tx Otitis Externa? |
|
|
|
A 35 yo diabetic comes into the urgent care complaining of ear pain that is deep. HPI reveals that the Pt was seen a few weeks ago for Otitis Externa. What is at the top of your Diff Dx list, why, what are you looking for on PE, how will you confirm? |
granulation tissue in ear canal
|
|

What is this and what is it indicative of? |
This is granulation tissue in the ear canal and is indicative of MEO (osteomyelitis) |
|

What is this and what are possible causes? |
Serous Otitis Media
|
|

What is this and what causes it? |
Typmanic Membrane
|
|
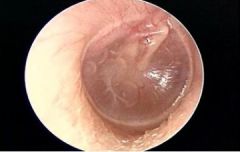
What would your clinical findings be for this Pt? |
Hypomobile TM Retracted TM Dull TM Air bubbles or fluid posterior to TM (non purulent no infxn) Conductive hearing loss |
|
|
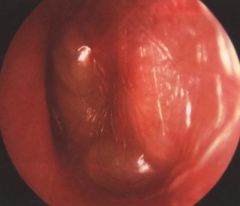
Pt presents w/Otalgia, fever, conductive hearing loss. HPI indicates recent URI. What is the most likely Dx, why, what PE will r/in or r/out? |
Acute Otitis Media
erythematous, bulging TM with purulent exudate posterior |
|

Yesterday your Pt's TM looked like this. You prescribed Abx. They called today to tell you they don't need to take the Abx because the pain is suddenly gone. What happened? |
Pt's TM ruptured resulting in a sudden sense of pain relief and otorrhea. Pt still needs to complete the full course of Abx prescribed |
|
What bacteria are the most likely culprits for this? |
Streptococcus pneumoniae Streptococcus pyogenes Haemophilus influenzae |
|

What would be your first choice to Tx this? |
|
|
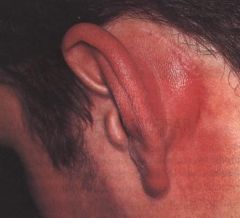
This Pt presents with a fever, Hx of recent AOM, and what is pictured. What is the most likely Dx, why, and what is Tx? |
Mastoiditis because the inflammed mass over the mastoid bone, fever, and recent AOM infxn. Pt needs IV Abx (cephalosporin) URGENTLY to prevent surgical intervention |
|
|
Recurrent OM or TM perforation can result in what? |
Chronic Otitis Media |
|
|
Chronic purulent aural discharge, otalgia, hearing loss are S/Sxs of what dz? |
Chronic Otitis Media |
|

You culture this exudate and determine it is Staphylococcus aureus. What is the most likely Dx and why? |
Chronic Otitis Media Staphylococcus aureus is causative an perforated TMs are more likely to develop COM |
|
|
What is the firstline Tx of Chronic Otitis Media? |
Fluoroquinolones (Otic drops or oral) |
|
|
What medication is contraindicated if Pt has perforated TM? |
Corticosteroids |
|

What is this and why does a Pt need it? |
Tympanostomy tubes to help with chronic OM and eustachian tube dysfxn |
|

Describe the Dz process in the picture |
No active Dz process - just a scar from previous TM perforation(s) |
|

Complication of a chronically retracted TM is |
Cholesteatoma
|
|

This Pt complains of aural fullness, fluctuating hearing, pain w/changes in pressure (flying). What is this called and what is the best method of Tx? |
Eustachian Tube Dysfxn Pt can take oral & intranasal decongestants to help drain some of the fluid back up |
|
|
A Pt took a recent trip to Africa and experienced severe Otaglia and temporary hearing loss when the plane was making it's descent. What caused it and what are some management techniques? |
Pt is experiencing barotrauma as a result of having poor eustachian tube fxn. Pt is unable to equalize the pressure changes in the inner ear leading to the pain and temporary hearing loss. Pt can take an oral decongestant 30 minutes before expected altitude change or can try to equalize the pressure by yawning, chewing, swallowing, or autoinflating. |
|
|
The sensation of sound when there is no exogenous source of sound is called? |
Tinnitus |
|
|
Tinnitus can be Txd by: |
|
|
|
Vertigo is defined as: |
The sensation of spinning or motion when there is no motion or spinning. |
|
|
The cardinal symptom of vestibular Dz |
Vertigo
|
|
|
Pt presents with gradual onset, progressive vertigo without any associated auditory symptoms. Which category of Vertigo does the Pt have and why? |
Central - because it is gradual and no associated hearing symptoms |
|
|
Pt presents with rapid onsent, severe vertigo, with tinnitus and hearing loss. Which category of Vertigo does the Pt have and why? |
Peripheral - because it is rapid, severe, and has associated auditory symptoms |
|
|
Duration of vertigo & auditory Sxs are |
the distinguishing feature of vertigo |
|
|
Pt presents with fluctuating hearing loss, tinnitus, episodic vertigo spells lasting a few hours. What is the Dx and what is the Tx? |
Meniere's Dz Pt should eat a low salt diet, restrict caffeine, take a diruetic, and get a referral to neurology |
|
|
What is Meniere's Dz |
Edema and distention of the endolymphatic compartment |
|
|
Pt presents with acute, continuous, severe vertigo lasting for up to a week, with unilateral hearing loss, and tinnitus. What is the Dx for the Pt and what is the Tx? |
Labyrinthitis
|
|
|
Pt presents with recurrent brief (1-2 min) episodes of vertigo every time she moves her head to the side. What is the Dx and Tx? |
Benign Paroxysmal Positioning Vertigo
|
|
|
Pt presents complaining of a single paroxysmal episode of vertigo that does not involve the ear but lasts a few days. What is the Dx and the Tx? |
Vestibular Neuronitis supportive care for Tx including valium |
|
|
Pt presents with unilateral sensorineural hearing loss, deterioration of speech and discrimination. Pt has continuous dysequilibrium. What is the Dx and Tx? |
Acoustic Neuroma: a benign lesion of CN VIII that is Dxd using MRI. Tx includes obsveration, microsurgical excision, stereotactic radiotherapy, VEGF inhibitors |
|

Pt presents with a foul smelling d/c from the left nostril. Otoscopic examination reveals this. What happened and why? |
Pt has a FB obstrxn made or an organic material that became infxd |
|

In what type of Pt are you most likely to find this? |
|
|

Your Pt has a Hx of recent nasal packing to stop epistaxis. Visual examination of the nose reveals this. What is it and why did they get it? |
Rhinolith: a large foreign body often found in the nose of adults who had nasal packing |
|

What tools should be used or considerations should be made with this Pt? |
|
|
are all types of what? |
Nasal Trauma |
|

This Pt comes in complaining of difficulty breathing on the left side, snoring, nasal d/c, and post nasal drip. What is the Dx and what is the Tx? |
Dx: Nasal Septal Deviation Tx: Maintain airway & surgical correction if severe |
|

This Pt presents with a whistling noise during breathing, occasional epistaxis, malodorous d/c from nose. What is the Dx and Tx? |
Dx: Nasal Septal Perforation Tx: none if mild, if moderate - severe can use a silicone prothesis or have surgically corrected. Also should keep lubricated with bacitracin ointment |
|

What can cause this? |
|
|

What is this and what is it called? |
Nasal Septal Hematoma: collection of blood localized to the septum usually the result of trauma |
|

What is the appropriate Tx for this and what are the possible complications? |
Tx: I&D both sides, culture fluid, pack the nose, prophylatic Abx Complications: Staph infxn, saddle nose defect |
|
|
Pt presents with non-specific findings, nasal congestion, watery rhinorrhea, hyposmia, sneezing, dry cough, malaise, pharyngitis. Pt wants Abx to Tx. What do you tell your Pt and why? |
Pt most likely has viral rhinosinusitis or the common cold. Viral infxns do not respond to Abx and so they are not an appropriate tx. Dz is self-limiting typically 10 days and Pt can take a variety of OTC meds: oral decongestant, nasal decongestant, nasal saline, NSAIDs, Zinc acetate to reduce duration of Sxs. |
|
|
How do you educate your Pt on the prevention/Tx of Viral Rhinosinusitis? |
Px: Good hand, cough hygiene, and minimize contact with others to prevent spread Tx: increase fluids, rest, OTC support |
|
|
Pt presents with inflamed nasal cavity, purulent d/c, nasal congestion, hyposmia, facial pain & pressure, cough, halitosis. What is your Dx? |
Acute Bacterial Rhinosinusitis |
|
|
What are possible complications of ABRS? |
|
|
|
What is the best way to Tx ABRS? |
presentation is complicated |
|
|
What are the firstline Abx for ABRS? |
|