Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
Acetylcholine and gastrin
|
Acetylcholine and gastrin promote the release of histamine from the mast cell or enterochromaffin-like cells, which then bind to the histamine H2-receptor on the parietal cell.
|
|
|
Activation of H2 receptors
|
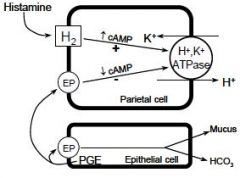
Activation of H2 receptors activates adenylyl cyclase which increases the levels of cAMP which activates intracellular protein phosphokinases.
This activates the hydrogen-potassium adenosine triphosphatase (H+/K+-ATPase) or proton pump to move into position in the secretory canaliculus located in the apical membrane of the parietal cell. The proton pump transports hydrogen ions out of the cytoplasm and into the secretory canaliculus, where they are exchanged for potassium ions that enter the parietal cell via the opposite ion channel. In the secretory canaliculus, the hydrogen ion combines with chloride form hydrochloric acid (HCl), which is then released from the secretory canaliculus into the gastric acid lumen. The proton pump is the final common pathway for gastric acid secretion |
|
|
Mucosal defense
|
The secretion of a mucus layer that protects gastric epithelial cells is key defense mechanism against acid.
|
|
|
Mucus production
|
Mucus production is stimulated by prostaglandins E2 (and prostacyclin), which also directly inhibit gastric acid secretion by parietal cells
|
|
|
Mucosal defense
|
A second important part of the normal mucosal defense is the secretion of bicarbonate ions by superficial gastric epithelial cells. Bicarbonate neutralizes the acid in the region of the mucosal cells, thereby raising pH and preventing acid-mediated damage.
|
|
|
Alcohol aspirin and other drugs--mucus secretion
|
Alcohol, aspirin, and other drugs that inhibit prostaglandin formation decrease mucus secretion and predispose to the development of acid-peptic disease.
|
|
|
Increased attack
|
i. Increased acid secretion may occur in patients with duodenal ulcer, but most patients with gastric ulcer have normal or reduced rates of acid secretion.
ii. Pepsin plays a role in the proteolytic activity involved in ulcer formation. |
|
|
Decrease in Mucosal defense
|
i. Mucosal defense and repair mechanisms protect the gastroduodenal
mucosa from noxious endogenous and exogenous substances. ii. The viscous nature and near-neutral pH of the mucus-bicarbonate barrier protect the stomach from the acidic contents in the gastric lumen. iii. The maintenance of mucosal integrity and repair is mediated by the production of endogenous prostaglandins. iv. H. pylori and NSAIDs cause alterations in mucosal defense by different mechanisms and are important factors in the formation of peptic ulcers. |
|
|
Pathophysiology of gastroesophageal reflux disease (GERD)
|
The pathophysiology of GERD is associated with defects in transient relaxations of the lower esophageal sphincter, esophageal acid clearance and buffering capabilities, anatomy, gastric emptying, mucosal resistance and with exposure of the esophageal mucosa to aggressive factors (gastric acid, pepsin, and bile salts) leading to esophageal damage.
|
|
|
Proton pump inhibitors (PPIs) -drugs/type
|
Drugs used for treating peptic ulcer disease and GERD
A. Inhibitors of acid secretion omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole |
|
|
Proton pump inhibitors (PPIs) - MECH
|
omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole
i. Irreversibly inhibit K+/H+ ATPase in parietal cells ii. DECR Daily gastric acid secretion iii. Takes 3–5 days for maximal inhibition of acid secretion |
|
|
Proton pump inhibitors (PPIs) - Adverse Effects
|
omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole
i. Most common: headache, nausea, diarrhea, and abdominal pain ii. Acid suppression may increase the risk of gastroenteritis, Clostridium difficile-associated colitis and community-acquired pneumonia. iii. Increase risk of fractures (hip, wrist, spine) in patients > 50 years old when taking high doses for prolonged periods ($ 1 year); supplement with vitamin D and calcium to prevent osteoporosis |
|
|
Proton pump inhibitors (PPIs) -drug interxn
|
omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole
i. These drugs will INCR gastric pH which may alter the rate of absorption &/or bioavailability of other drugs ii. Omeprazole Inhibits P450 --> DECR metabolism and thus INCR toxicity of other therapeutic agents that are metabolized by P450; other PPIs do not inhibit CYP2C19 iii. Inhibition of P450 enzymes inhibits conversion of clopidogrel to the active metabolite which would diminish the platelet effects of the drug |
|
|
Proton pump inhibitors (PPIs) -Clinical uses
|
omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole
The proton pump inhibitors are the most effective drugs in treating GERD and peptic ulcer disease. They are used in combination with antibiotics in eradicating H. pylori. They also can be used in combination with NSAIDS to reduce the risk of ulcers. |
|
|
Histamine H2 receptor antagonists -drugs
|
ranitidine, nizatidine, famotidine, & cimetidine
|
|
|
Histamine H2 receptor antagonists - mech
|
ranitidine, nizatidine, famotidine, & cimetidine
i. Competitive antagonists of histamine at H2 receptors ii. DECR Volume of gastric juice and its [H+] & DECR pepsin secretion |
|
|
Histamine H2 receptor antagonists -EXCRETION
|
ranitidine, nizatidine, famotidine, & cimetidine
Renally excreted, DECR dose in patients with renal impairment |
|
|
Histamine H2 receptor antagonists -Adverse reactions (Most common)
|
ranitidine, nizatidine, famotidine, & cimetidine
Headache, drowsiness, fatigue, diarrhea |
|
|
Histamine H2 receptor antagonists -Drug interactions
|
ranitidine, nizatidine, famotidine, & cimetidine
i. These drugs will INCR gastric pH which may alter the rate of absorption &/or bioavailability of other drugs ii. Cimetidine inhibits P450 --> DECR metabolism and INCR toxicity of other therapeutic agents that are metabolized by P450 |
|
|
Histamine H2 receptor antagonists -Clinical uses
|
ranitidine, nizatidine, famotidine, & cimetidine
These drugs revolutionized the treatment of peptic ulcer disease. They are available over the counter for occasional use for treating dyspepsia. Increasingly, the proton pump inhibitors are replacing the H2-receptor antagonists in clinical use for treatment of moderate to severe GERD and in peptic ulcer disease. |
|
|
Misoprostol (methyl derivative of
prostaglandin E1)--PROTECTION ACTIONS |
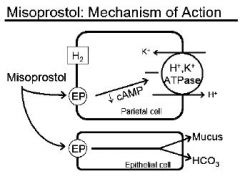
Protective actions include:
i. DECR acid secretion ii. INCR mucus secretion iii. INCR HCO3 secretion |
|
|
Misoprostol (methyl derivative of
prostaglandin E1)--Adverse reactions |
i. Diarrhea and abdominal cramping
ii. Uterine contractions--> CONTRAINDICATED during pregnancy |
|
|
Misoprostol (methyl derivative of
prostaglandin E1)--Clinical use |
Prevention of NSAID-induced gastric injury. In addition co-therapy with a proton pump inhibitor can reduce the risk of NSAID-induced gastric injury.
|
|
|
Sucralfate (complex of sulfated sucrose and poly-Al(OH)3)--Mech
|
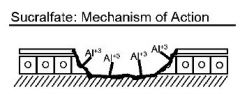
Provides a protective barrier; forms a gel that adheres to the ulcer crater
|
|
|
Sucralfate (complex of sulfated sucrose and poly-Al(OH)3)--ADVERSE EFFECTS
|
Can cause constipation due to Al3+ content
|
|
|
Sucralfate (complex of sulfated sucrose and poly-Al(OH)3)--DRYG INTERAXNS
|
Can inhibit the absorption of other drugs given concurrently. The interaction can be minimized by giving the interacting drug at least 2 hours before sucralfate.
|
|
|
Sucralfate (complex of sulfated sucrose and poly-Al(OH)3)--CLINICAL USE
|
Sucralfate can be used in treating mild cases of GERD and mild esophagitis but is not effective in the management of severe disease. Similarly better options (inhibitors of acid secretion) are available for treating peptic ulcer disease as well.
|
|
|
Bismuth Salts
a. Protective actions |
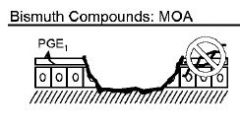
i. Forms a protective coating in the ulcer crater
ii. INCR Prostaglandin production iii. Anti-H. pylori activity |
|
|
Bismuth Salts--ADVERSE EFFECTS
|
Clinically important side effect: darkened stool
|
|
|
Bismuth Salts--CLINICAL USE
|
Bismuth subsalicylate has been used for years in treating mild GI ailments. Bismuth subcitrate potassium is available as a combination product with metronidazole and tetracycline for the treatment of H. pylori.
|
|
|
H. pylori and PUD
|
a. Gram-negative bacillus found on or between gastric epithelial cells
b. 70-90% of patients with PUD are infected c. H. pylori DECR mucosal protection |
|
|
Two examples of FDA approved regimens for H. pylori
|
i. Proton pump inhibitor + bismuth subsalicylate + metronidazole + tetracycline
ii. Proton pump inhibitor + clarithromycin + amoxicillin (or metronidazole) |
|
|
H pylori-- Antibiotic use
|
i. Two antibiotics are used to decrease the development of resistance.
ii. If therapy fails with one combination, then another should be used in subsequent treatment. iii. Amoxicillin should not be used in patients allergic to penicillins iv. Alcohol consumption should be avoided when taking metronidazole due to the drug’s disulfiram-like effects Eradicating H. pylori will DECR rates of recurrence compared to that of other drugs used to treat peptic ulcer disease |
|
|
Systemic antacids (can be absorbed systemically)
|
NaHCO3
|
|
|
Nonsystemic antacids (not absorbed to appreciable extent)
|
CaCO3,
Al(OH)3, Mg(OH)2 |
|
|
Antacids Pharmacologic properties
|
a. Antacids react with HCl to form neutral, less acidic or poorly soluble salts
b. Pepsin activity is decreased when pH > 5.0 |
|
|
Antacids--ADVERSE EFFECTS
|
a. NaHCO3 is absorbed --> transient metabolic alkalosis
b. Effects on bowel motility i. Al(OH)3 can cause constipation iI. Mg(OH)2 can cause loose stools or diarrhea iIi. When combined in the same preparation the net effect on bowel motility depends upon the ratio of Al3+ to Mg2+ c. Other adverse effects i. Al(OH)3 binds phosphate causing hypophosphatemia ii. Patients with impaired renal function --> DECR clearance of Al3+ and Mg2+ --> INCR plasma levels of Al3+ and Mg2+ --> systemic toxicity iii. Na+ content may be important in patients with CHF or HTN |
|
|
Antacids--DRUG INTERAXNS
|
i. These drugs will INCR gastric pH which may alter the rate of absorption &/or bioavailability of other drugs
ii. Al3+ compounds adsorb some drugs forming insoluble complexes which are not absorbed, thus DECR bioavailability iii. Alkalinization of the urine by these drugs may affect renal clearance (INCR elimination of acidic drugs, DECR elimination of basic drugs) |
|
|
Antacids--CLINICAL USE
|
i. Antacids were the main treatment of peptic ulcer disease before the discovery of the H2 receptor antagonists.
ii. OTC antacids can be used in patients with mild, infrequent heartburn. There are not used clinically for moderate to severe GERD or for treating peptic ulcer disease. |