Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
|
Ghrelin
|
Increased eating
Arcuate nuclesus of hypothalamus |
|
|
Leptin
Glucagon like peptide-1 (GLP-1) Peptide Y (PYY) |
Decreased eating
Arcuate Nucleus of hypothalamsu |
|
|
Neuropeptide Y (NPY)
Agouti Related Protein Opioids (mu) Galanin |
Incr eating--
Paraventricular nucleus of hypothalamus |
|
|
Melanocyte stimulating hormone
Corticotropin releasing hormone Cholecystokinin |
Decreased eating
Paraventricular nucleus of hypothalamus |
|
|
Orexin
Melanocyte concentration hormone |
Increased eating
Lateral Hypothlamus (only one) |
|
|
α2
5-HT1A |
Incr eating
Hypothalamus |
|
|
α1 and β2
5-HT1B and 2C Histamine H1 and H3 |
Decr eating
Hypothalamus |
|
|
Dopamine
|
Incr eating
Nucleus Accumbens (only one) |
|
|
Opioids
|
Incr eating
Amygdala (only one) |
|
|
Neuropeptide Y (NPY)
Agouti Related Protein Opioids (mu) |
Incr eating
Brainstem |
|
|
Leptin
Melanocyte stimulating hormone Cholecystokinin |
Decr eating
Brainstem |
|
|
Ghrellin
|
Incr eating
Vagus nerve |
|
|
Leptin
CCK GLP-1 PYY |
decr eating
Vagus Nerve |
|
|
Cannabinoid CB1
|
Incr eating
various/undetermined |
|
|
Dopamine D1 and D2
|
Decr eating
various/undetermined |
|
|
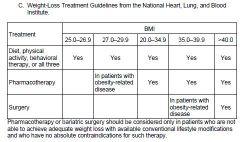
Guidelines for therapy based on BMI
|
|
|
|
Sympathomimetics (Diethylpropion and Phentermine)
a. Mechanism of action |
Appetite suppressants
(1) The norepinephrine transporter (NET) normally removes norepinephrine from the synaptic cleft so terminating its actions. (2) Norepinephrine is sequestered into vesicles via the vesicular monoamine transporter (VMAT). (3) Amphetamine and similar drugs enhance release of norepinephrine (a) Norepinephrine is released into the cytoplasm from vesicular stores (b) The direction of the monoamine transporters (including NET and VMAT) is reversed (4) The released norepinephrine acts on hypothalamic receptors (α1 and β2) to decrease eating (5) Weight regain occurs upon cessation of therapy |
|
|
Sympathomimetics (Diethylpropion and Phentermine)--Adverse Effects
|
(1) Insomnia (if taken in late in the day)
(2) Cardiovascular effects (hypertension, palpitations, arrhythmias, valvular heart disease) (3) Potential for abuse |
|
|
Sympathomimetics (Diethylpropion and Phentermine)--Contraindications
|
(1) Patient with hypertension or cardiovascular disease
(2) Diabetics may experience decreased insulin or oral hypoglycemic dosage requirements soon after starting therapy and prior to any weight loss (3) History of drug abuse |
|
|
Sympathomimetics (Diethylpropion and Phentermine)--Drug interaxns
|
MAO inhibitors
|
|
|
Sympathomimetics (Diethylpropion and Phentermine)--Clinical use
|
(1) Short-term (up to 12 weeks) use in weight management
(2) Mean weight loss of about 3 kg more than with placebo (3) As tolerance develops, they become ineffective, and the risk of dependence and abuse increases. |
|
|
Lorcaserin
a. Mechanism of action |
(1) Lorcaserin is an agonist of the the 5-HT2C receptor designed to promote weight loss.
(2) Activation of the 5-HT2C receptor decreases food intake through the proopiomelanocortin system of neurons. |
|
|
Lorcaserin--Adverse Effects
|
Headache, nausea and dizziness
|
|
|
Lorcaserin--contraindications & precautions
|
Potential for serotonin syndrome when taken with other drugs which modulate serotonin
|
|
|
Lorcaserin--drug interactions
|
(1) Inhibits CYP2D6 which would increase the serum concentrations of drugs metabolized by this P450 isoenzyme
(2) Potential for serotonin syndrome |
|
|
Lorcaserin--Clinical Use
|
(1) Approved for use in obese patients (body mass index [BMI] of >30
kg/m2) and for patients who are overweight (BMI >27 kg/m2) and have one weight-related risk factor such as hypertension, dyslipidemia or type 2 diabetes. (2) Moderate effect on weight loss (3%-4% reduction of individual’s body weight) |
|
|
Phentermine and topiramate combination
a. Mechanism of action |
1) Phentermine - see above
(2) Topiramate is an antiepileptic drug. Some patients experience weight loss with topiramate and it is hypothesized that this may be due tobappetite suppression resulting from both antagonism of AMPA receptors and metabolic acidosis. |
|
|
Phentermine and topiramate combination--Adverse Effects
|
(1) Insomnia and cardiovascular effects related to the phentermine
(2) Cognitive impairment, and metabolic acidosis and kidney stones with topiramate (3) Those associated with the combination include dry mouth, paresthesia, constipation, and dysgeusia |
|
|
Phentermine and topiramate combination-Contraindications & precautions
|
Contraindicated for use in pregnancy - Topiramate is associated with increased risk of oral clefts when taken in the first trimester of pregnancy
|
|
|
Phentermine and topiramate combination--Drug Interactions
|
(1) Phentermine - MAO inhibitors
(2) Inhibitors and inducers of P450 enzymes have corresponding effects on blood levels of topiramate |
|
|
Phentermine and topiramate combination--Clinical Use
|
(1) Approved for use in obese patients (body mass index [BMI] of >30 kg/m2) and for patients who are overweight (BMI >27 kg/m2) and have one weight-related risk factor such as hypertension, dyslipidemia or type 2 diabetes.
(2) 7%-9% reduction of individual’s body weight |
|
|
Impairment of food absorption (orlistat)
1. Mechanism of action |
a. Lipase hydrolyzes dietary fat (triglycerides) into absorbable free fatty acids and monoacylglycerols.
b. Micelle formation allows absorption of approximately 90% of dietary triglyceride as monoacylglycerol and fatty acids; cholesterol and fat-soluble vitamins absorbed with lipids c. Orlistat is a synthetic derivative of the naturally-occuring lipase inhibitor, lipostatin (produced by the mold Streptomyces toxytricini). Orlistat forms a covalent bond with active sites in the lipase. d. By inhibiting GI lipase, approximately 1/3 of dietary triglyceride is excreted unchanged in stool; absorption of cholesterol and fat-soluble vitamins are also decreased |
|
|
Impairment of food absorption (orlistat)--Adverse Effects
|
a. Flatulence with discharge
b. Oily spotting c. Fecal urgency More likely to occur after high-fat dietary indiscretions and are associated with a high incidence of drug discontinuation. |
|
|
Impairment of food absorption (orlistat)--Drug interactions
|
Absorption of fat-soluble vitamins is decreased. Supplements are required. They should be taken 2 hours before or 1 hour after taking orlistat.
|
|
|
Impairment of food absorption (orlistat)--Clinical Use
|
a. Approved for long term use in patients >12 years old.
b. After one year, orlistat produces a weight loss of about 9–10%. |
|
|
Drugs which affect weight (for information only)
|
readable in handout
|