![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
What is the diabetic foot triad? |
Vasculopathy - peripheral vascular disease - microangiopathy --> nail changes, gangrene of digits Immunopathy - monomicrobial vs polymicrobial - predominantly gram +ve cocci, followed by gram -ve and anaerobes - present as abscess, OM, septic arthritis, cellulitis Neuropathy - glove and stocking sensory loss (sensation) - clawing of toes (motor) - dryness of skin (autonomic) |
|
|
What are the different presentations of a diabetic foot? |
1. Ulcers (neuropathic, vascular, decubitus) 2. Cellulitis OR necrotizing fasciitis (TRO) 3. Gangrene (wet vs dry) 4. Infection (osteomyelitis, septic arthritis, abscess, necrotizing fasciitis, gas gangrene) 5. Charcot foot |
|
|
What are the common areas for the different types of ulcers? |
1. vascular/ischemic - dorsum of foot - 1st web spae - heel - toes - anterior shin - lateral aspect of leg - bony areas 2. Neuropathic ulcer (tripod stance) - sole of foot - pulp of toe 3. Decubitus - heel - lateral aspect of base of 5th metatarsal 4. Venous - Medial aspect of leg (may be behind malleolus) - Gaiter's area |
|
|
What is the definition of critical limb ischemia? |
1. rest pain that is relieved by dependency 2. gangrene 3. ischemic ulcer *** pallor <20 degree of lifting foot up *** ABPI < 0.5 is critical limb ischemia *** other symptoms of limb ischemia: claudication, 6 Ps (pallor, parasthesia, pain, paralysis, pulselessness, perishingly cold) |
|
|
What are the examination findings of charcot's joint? |
- enlargement of joint - hypermobility of joint - warm and swollen initially, followed by crepitus in later stages - may have collapse of midfoot and rocker bottom deformity as a result - commonly affects mid tarsal joints, followed by metatarsophalangeal joint and finally ankle joint |
|
|
What is the pathophysiology of hammer toes, mallet toes & claw toes? |
1. imbalance between intrinsic and extrinsic muscle strength mallet toes: flexion deformity of DIPJ, with no PIPJ or MTPJ involvment claw toes: flexion deformity at DIPJ and PIPJ hammer toes: flexion deformity of PIPJ |
|
|
How to assess for vasculopathy? |
1) skin changes:
- loss of hair - pale/dusky discoloration - shiny - trophic nail changes - hyperpigmentation 2) Look for ischemic ulcers 3) Assess for temperature of skin (perishingly cold) 4) Assess for capillary refill time 5) Assess for all peripheral pulses 6) Buerger's test (conduct if 1 or more pulses are not palpable) - indicates PVD - also assess for severity of PVD based on the vascular angle |
|
|
How to assess for neuropathy? |
1) Pin prick testing in glove and stocking distribution - look for hyperaesthesia, hypoaesthesia, anaesthesia 2) Propioception and vibration sense 3) Tendon reflex (ankle jerk) 4) protective sensation via 10 points semmes weinstein monofilament testing - should be more than 7 in normal patients |
|
|
What are the signs of autonomic neuropathy on skin? |
- dry skin - scaling - fissuring - callosity (tips of toes/soles) |
|
|
What is the definition of charcot's joint?
x-ray changes of charcot's joint? |
Progressive degeneration of a weight bearing joint, resulting in deformity
pathophysiology is either a) increased osteoclasts to area due to increased blood supply and hence collapse of foot bony structure
b) repetitive microtrauma leading to inflammatory resorption, hence collapse of foot bony structure
** a/w with hypertrophic changes on x-ray usually: - density increase - debris - distended joint - dislocation - disorganisation - destruction of joint |
|

Describe and diagnose |
Charcot foot: - destruction of tarsometatarsal joints - sclerotic margins - general disorganization of tarsal bones - joint surface uneven |
|
|
Indications of amputation? |
- dead limb - dangerous limb - damn nuisance |
|
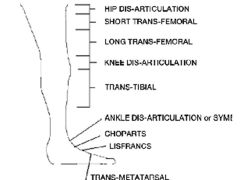
Types of amputation? |
ray (tarso-metatarsal of 1 ray) > Forefoot (trans-metatarsal)> lisfranc (tarso-metatarsal) > chopart's (mid tarsal)> syme's (through ankle) > BKA > AKA |
|
|
King's classification of DM foot |
|
|
|
general management of diabetic foot? |
1) control DM - hypocount charting TDS + 10pm - start insulin sliding scale 2) prevent dehydration - IO charting - IV at least 1.5 L a day 3) cover with topical and oral/IV antibiotics - trace blood culture - trace wound culture - trace inflammatory markers: ESR, CRP, FBC - change from broad spectrum to specific antibiotics after culture results are out 4) Daily wound dressing 5) Elevate the limb if swollen |
|
|
Specific management plan for diabetic foot |
1. Ulcers: - radical debridement if deep and dirty - Vascular consult (KIV angioplasty) - KIV amputation, depending on presence of contamination, OM, cellulitis, abscess, vascularity etc - special footwear, offloading 2. Gangrene - If dry: wait for the segment to auto-amputate, and clean the area regularly - If wet: amputation - Vascular consult 3. Abscess: - I&D in OT |
|
|
MDM team for DM foot |
surgeons: ortho, vascular medical: endocrinologists, ID specialists, KIV renal allied health: podiatrist, dietician, PT, OT, MSW nurses: DM nurse, wound care nurse KIV amputation support group |
|
|
Specific treatment for charcot's foot |
o Conservative Contact casting Charcot restraint orthotic walker (CROW) Refer podiatrist for shoe modifications Bisphosphonate therapy o Surgical Exostectomy Correct the deformities using plates and screws Arthrodesis |
|

What is this |
charcot restraint orthotic walker (CROW) |