![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
178 Cards in this Set
- Front
- Back
|
Neurofibromatosis 1: Name the Gene Name the Chromosome Name the Inheritance pattern What is the eponym? |
Gene: Neurofibromin (involved in cell signaling) Chromosome: 17 (q11.2) Inheritance Pattern: Autosomal Dominant Eponym: Von Recklinghausen Disease |
|
|
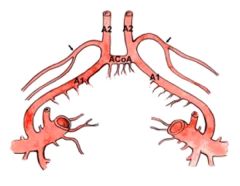
Posterior Circulation: Name the origin: Posterior Inferior Cerebellar Artery Anterior Inferior Cerebellar Artery Superior Cerebellar Artery |
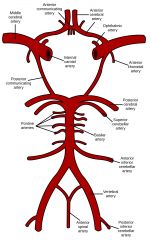
PICA: From the vertebral artery prior to the origin of the anterior spinal arteries AICA: Proximal basilar artery SCA: Distal basilar artery just prior to the origin of the posterior cerebral arteries image09 |
|
|
Trapezius Name the: Nerve Roots Trunk Cord Action Test |
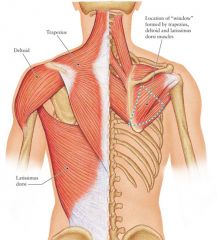
Nerve: Spinal Accessory Roots: C3-C4 Trunk: Pre-trunk Cord: Pre-cord Action: Shoulder elevation Test: Shrug the shoulders image04 |
|
|
Rhomboids Name the: Nerve Roots Trunk Cord Action Test |
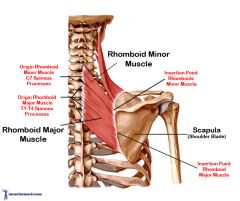
Nerve: Dorsal scapular Roots: C4-C5 Trunk: Pre-trunk Cord: Pre-Cord Action: Scapular retraction and elevation Test: Place the hand on the small of the back and push out, away from the back image00 |
|
|
Supraspinatus Name the: Nerve Roots Trunk Cord Action Test |
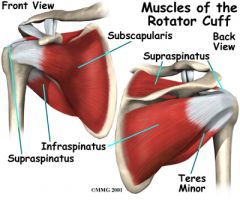
Nerve: Suprascapular nerve Roots: C5-C6 Trunk: Upper Trunk Cord: Pre-Cord Action: Shoulder abduction, first 30 degrees Test: Have the patient abduct the shoulder. For the first 10-15 degrees, the supraspinatus is the principal abductor of the shoulder. Beyond 30 degrees, the deltoid muscle becomes the main propagator of this action. image08 |
|
|
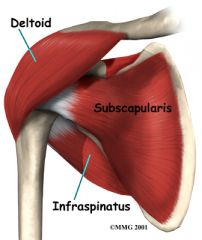
Infraspinatus Name the: Nerve Roots Trunk Cord Action Test |
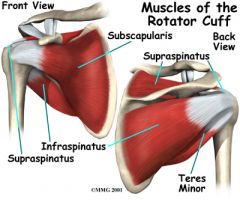
Nerve: Suprascapular Roots: C5-C6 Trunk: Upper Trunk Cord: Pre-Cord Action: Shoulder external rotation and adduction Test: Have the patient externally rotate the shoulder. This can be best appreciated when the patient holds the elbow at the side, flexes it to mid-position, and rotates the forearm outwards against resistance. It can be palpated just below the scapular spine. image08 |
|
|
Teres Major Name the: Nerve Roots Trunk Cord Action Test |
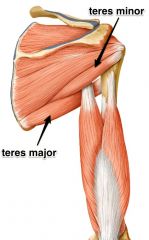
Nerve: Lower subscapular Roots: C5-C6 Trunk: Upper trunk Cord: Posterior cord Action: Shoulder adduction and internal rotation Test: Have the patient adduct the elevated shoulder. This muscle also contributes to internally rotating the humerus.
image 13 |
|
|
Subscapularis Name the: Nerve Roots Trunk Cord Action Test |
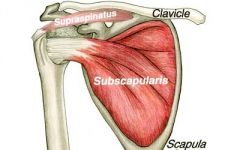
Nerve: Upper subscapular Roots: C5-C6 Trunk: Upper trunk Cord: Posterior cord Action: Shoulder internal rotation Test: Have the patient internally rotate the shoulder. This can be best appreciated when the patient holds the elbow at the side, flexes it to mid-position, and rotates the forearm inwards against resistance. image 12 |
|
|
Teres Minor Name the: Nerve Roots Trunk Cord Action Test |
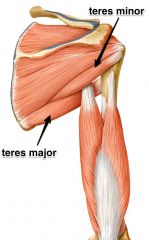
Nerve: Axillary Roots: C5-C6 Trunk: Upper trunk Cord: Posterior cord Action: Shoulder external rotation Test: Have the patient externally rotate the shoulder. This muscle is generally less powerful and less easy to palpate than the infraspinatus, which has the same action. image 13 |
|
|
Deltoid Name the: Nerve Roots Trunk Cord Action Test |
Nerve: Axillary Roots: C5-C6 Trunk: Upper Trunk Cord: Posterior Cord Action: Shoulder abduction Test: Have the patient abduct the shoulder. For the first 10-15 degrees, the supraspinatus is the principal abductor of the shoulder. Beyond 30 degrees, the deltoid muscle becomes the main propagator of this action. image 15 |
|
|
Biceps Brachii Name the: Nerve Roots Trunk Cord Action Test |
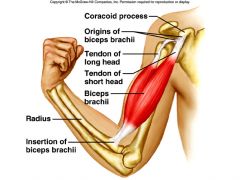
Nerve: Musculocutaneous Roots: C5-C6 Trunk: Upper Trunk Cord: Lateral Cord Action: Elbow flexion and forearm supination Test: Have the patient flex the elbow with forearm in the supinated position. Alternatively, have the patient supinate the forearm. The biceps brachii is a more powerful supinator than the supinator muscle. image 19 |
|
|
Serratus Anterior Name the: Nerve Roots Trunk Cord Action Test |

Nerve: Long thoracic Roots: C5-C6-C7 Trunk: Pre-trunk Cord: Pre-cord Action: Scapular protraction and stabilization Test: Have the patient push the hand forward with the arm straight. Weakness of the serratus anterior will manifest as winging of the scapula when the patient pushes against a wall. image 35 |
|
|
Brachialis Name the: Nerve Roots Trunk Cord Action Test |
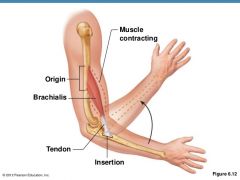
Nerve: Musculocutaneous Roots: C5-C6 Trunk: Upper Cord: Lateral Action: Elbow flexion Test: Have the patient flex the elbow. Unlike the biceps brachii, the brachialis inserts on the ulna rather than the radius and therefore does not participate in pronation or supination. image 22 |
|
|
Pectoralis Major (clavicular head) Name the: Nerve Roots Trunk Cord Action Test |
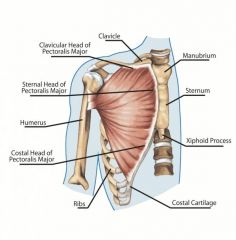
Nerve: Lateral Pectoral Roots: C5-C6 Trunk: Upper trunk Cord: Lateral Cord Action: Shoulder flexion, adduction, internal rotation Test: This muscle has multiple actions. Have the patient flex the shoulder (i.e. throw a side-arm pitch), adduct the shoulder, or internally rotate the shoulder (i.e. arm wrestle) |
|
|
Brachioradialis Name the: Nerve Roots Trunk Cord Action Test |
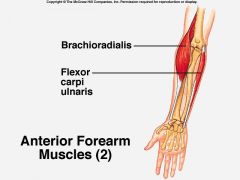
Nerve: Radial Roots: C5-C6 Trunk: Upper Trunk Cord: Posterior Action: Elbow flexion in midpronation Test: Have the patient flex the elbow with the forearm in mid-pronation image 29 |
|
|
Extensor Carpi Radialis Longus Name the: Nerve: Roots: Trunk: Cord: Action: Test: |

Nerve: Radial Roots: C6-C7 Trunk: Upper & Middle Cord: Posterior cord Action: Wrist extension Test: Have the patient extend the wrist radially. image 41 |
|
|
Supinator Name the: Nerve: Roots: Trunk: Cord: Action: Test: |
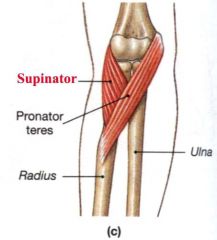
Nerve: Posterior interosseous Roots: C6-C7 Trunk: Upper & Middle Trunk Cord: Posterior Cord Action: Forearm supination Test: Have the patient supinate the forearm. The supinator muscle assists the biceps brachii in this action. image 46 |
|
|
Pronator Teres: Nerve: Roots: Trunk: Cord: Action: Test: |
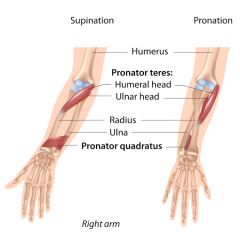
Nerve: Median Roots: C6-C7 Trunk: Upper & Middle Trunk Cord: Lateral Cord Action: Forearm pronation Test: Have the patient pronate the forearm with the elbow fully extended. image 47 |
|
|
Flexor Carpi Radialis: Nerve: Roots: Trunk: Cord: Action: Test: |
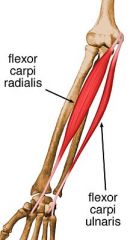
Flexor Carpi Radialis: Nerve: Median Roots: C6-C7 Trunk: Upper & middle trunk Cord: Lateral cord Action: Wrist flexion Test: Have the patient flex the wrist radially. image 55 |
|
|
Triceps Nerve: Roots: Trunk: Cord: Action: Test: |
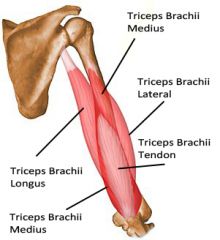
Triceps Nerve: Radial Roots: C6-C7-C8 Trunk: Upper, Middle, and Lower Cord: Posterior Action: Elbow extension Test: Have the patient extend the elbow. In manual muscle testing, it is best to let the patient start with the elbow at 90 degrees. At more acute angles, the triceps is at a mechanical disadvantage. image 64 |
|
|
Extensor Carpi Ulnaris Nerve: Roots: Trunk: Cord: Action: Test: |
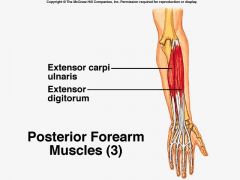
Extensor Carpi Ulnaris Nerve: Posterior interosseous Roots: C7-C8 Trunk: Middle & Lower Cord: Posterior Action: Wrist extension Test: Have the patient extend the wrist with an ulnar deviation image 66 |
|
|
Pectoralis Major - (sternocostal head): Nerve: Roots: Trunk: Cord: Action: Test: |
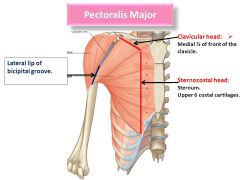
Pectoralis Major sternocostal: Nerve: Medial pectoral Roots: C8-T1 Trunk: Lower trunk Cord: Medial Cord Action: Shoulder flexion, adduction, internal rotation Test: The muscle has multiple actions. Have the patient flex the shoulder (i.e. throw a side-arm pitch), adduct the shoulder, or internally rotate the shoulder (i.e. arm-wrestle). image 56 |
|
|
Latissimus Dorsi: Nerve: Roots: Trunk: Cord: Action: Test: |
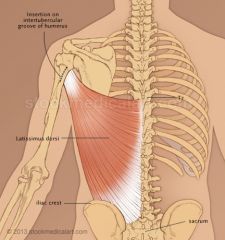
Latissimus Dorsi: Nerve: Thoracodorsal nerve Roots: C6-C7-C8 Trunk: Upper, Middle, and Lower Cord: Posterior Action: Shoulder extension, adduction, internal rotation Test: Have the patient extend the shoulder with the arm fully adducted and internally rotated. image 68 |
|
|
Extensor Digitorum Communis: Nerve: Roots: Trunk: Cord: Action: Test: |

Extensor Digitorum Communis: Nerve: Posterior Interosseous Roots: C7-C8 Trunk: Middle & Lower Trunk Cord: Posterior Action: Finger extension (digits 2-5) Test: Have the patient extend digits 2-5. For the purposes of manual muscle testing, it may be most useful to test the extension of a single digit such as the middle finger. image 70 |
|
|
Extensor Indicis: Nerve: Roots: Trunk: Cord: Action: Test: |

Nerve: Posterior interosseous Roots: C7-C8 Trunk: Middle & Lower Trunk Cord: Posterior Cord Action: Finger extension (index finger) Test: Have the patient extend the index finger
image 71 |
|
|
Extensor Pollicis Longus: Nerve: Roots: Trunk: Cord: Action: Test: |

Extensor Pollicis Longus: Nerve: Posterior interosseous Roots: C7-C8 Trunk: Middle & Lower Trunk Cord: Posterior Action: Thumb extension Test: Have the patient extend the thumb image 72 |
|
|
Abductor Pollicis Longus: Nerve: Roots: Trunk: Cord: Action: Test: |
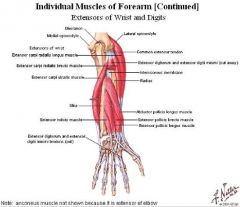
Abductor Pollicis Longus: Nerve: Posterior interosseous Roots: C7-C8 Trunk: Middle & Lower Trunk Cord: Posterior Cord Action: Thumb abduction Test: Have the patient abduct the thumb at right angles to the palm. This muscle is part of the anterior border of the anatomical snuff box. image 77 |
|
|
Flexor pollicis longus Nerve: Roots: Trunk: Cord: Action: Test: |

Flexor pollicis longus Nerve: Anterior interosseous Roots: C7-C8 Trunk: Middle & Lower trunk Cord: Lateral & Medial cord Action: Thumb flexion Test: Have the patient flex the thumb at the interphalangeal joint. image 85 |
|
|
Flexor Digitorum Profundus (digits 2 & 3) Nerve: Roots: Trunk: Cord: Action: Test: |
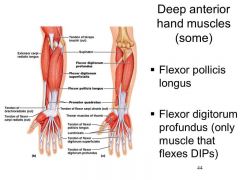
Flexor Digitorum Profundus (digits 2 & 3) Nerve: Anterior interosseous Roots: C7-C8 Trunk: Middle & Lower Trunk Cord: Lateral & Medial cord Action: Finger flexion - digits 2-3 Test: Have the patient flex the distal phalanx of the index finger or middle finger with the middle phalanx held in the fully extended position. image 90 |
|
|
Pronator Quadratus: Nerve: Roots: Trunk: Cord: Action: Test: |
Pronator Quadratus Nerve: Anterior interosseous Roots: C7-C8 Trunk: Middle & Lower Trunk Cord: Lateral & Medial Cord Action: Forearm pronation Test: Have the patient pronate the forearm with the elbow flexed. image 108 |
|
|
What are the functional components of hypoglossal nerve (Cranial Nerve 12)? |
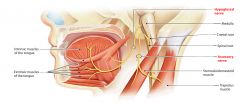
1. General somatic efferent: Supplies all of the intrinsic and extrinsic muscles of the tongue except the palatoglossus.
image 111 |
|
|
Flexor digit superficialis Nerve: Roots: Trunk: Cord: Action: Test: |
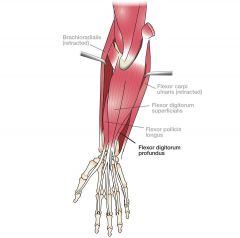
Flexor digit superficialis Nerve: Median Roots: C7-C8-T1 Trunk: Middle & Lower Trunk Cord: Lateral and Medial Cord Action: Finger flexion Test: Have the patient flex one of the fingers at the proximal interphalangeal joint with the proximal phalanx and distal phalanx held in the fully extended position. image 112 |
|
|
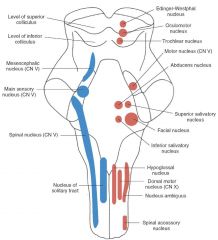
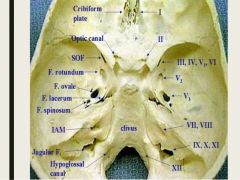
Which cranial nerves originate from these structures? Midbrain Pons Medulla Oblongata |
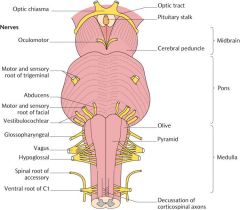
Midbrain: 3 and 4 Pons: 5, 6, 7, 8 Medulla Oblongata: 9, 10, 11, 12 image00 |
|
|
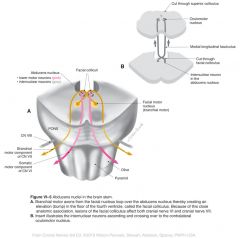
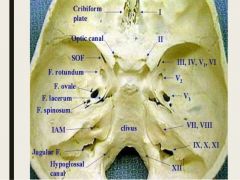
Which cranial nerves originate from the anterior pontomedullary junction? Which is most medial? Which is most lateral? |
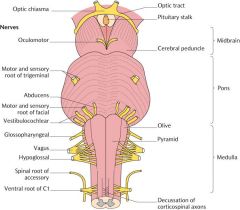
Cranial Nerves 6, 7, and 8 arise from the pontomedullary junction. 6 is most medial. 8 is most lateral. image03 |
|
|
Broca's area: What are the Brodmann's area numbers? Which gyrus is it located on? What structures in that gyrus does it occupy? |
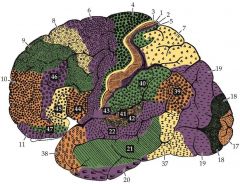
Brodmann's area numbers: 44, 45 Gyrus: Inferior Frontal Gyrus Structures: Pars triangularis and Pars opercularis image01 |
|
|
What are the seven segments of the internal carotid artery? |
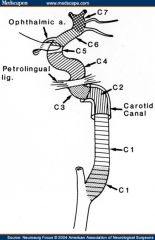
1. Cervical 2. Petrous (horizontal) 3. Lacerum 4. Cavernous 5. Clinoid (clinoid processes arise from the sphenoid bone) 6. Ophthalmic (supraclinoid) 7. Communicating (terminal) image02 |
|
|
What is the origin of: Right common carotid Left common carotid Vertebral arteries |
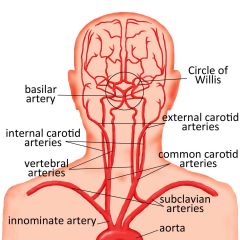
Right Common Carotid: Brachiocephalic (innominate) artery Left Common Carotid: Aorta Vertebrals: Subclavian arteries |
|
|
Wernicke's Encephalopathy: Deficiency of what vitamin? Name the classical clinical triad. Name 4 other clinical symptoms |
Vitamin: Vitamin B1 (thiamine) Triad: 1. Confusion 2. Ophthalmoplegia 3. Ataxia (axial, not appendicular) Other signs/symptoms: 1. Nystagmus 2. Hypothermia 3. Hypotension 4. Memory deficits |
|
|
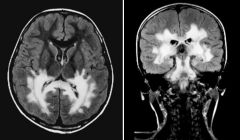
Wernicke's Encephalopathy: Name 3 parts of the brain where abnormal signal can be seen on MRI? Why do you need to give thiamine before glucose? |
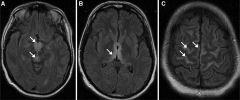
Abnormal signal on MRI: 1. Medial thalami 2. Mamillary bodies (part of the hypothalamus, can enhance) 3. Periaqueductal region Thiamine before glucose: Glucose is metabolized to pyruvate. Pyruvate can be metabolized to lactic acid (can be lethal) or enter the TCA cycle where it is metabolized to acetyl CoA. Thiamine cofactor is needed for the TCA cycle. |
|
|
What is decerebrate posturing and where is the lesion?
What is decorticate posturing and where is the lesion?
What does progression from decorticate to decerebrate posturing indicate? |
Decerebrate posturing: Extension of all four limbs. The lesion is below the red nucleus.
Decorticate posturing: Flexion of the forelimbs and extension of the hind limbs. The lesion is above the red nucleus.
Progression can indicate uncal or tonsillar herniation. |
|
|
Gerstmann Syndrome: What are the four primary symptoms? Where is the lesion? |
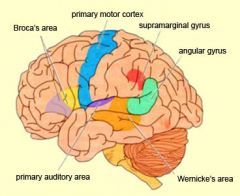
Symptoms: 1. Dysgraphia 2. Dyscalculia 3. Finger agnosia (inability to distinguish the fingers on the hand) 4. Left-right disorientation Lesion: Dominant hemisphere (left): Angular and supramarginal gyri near the temporoparietal junction. image07 |
|
|
Kluver-Bucy Syndrome: What are the four primary symptoms? Where is the lesion? |
Symptoms: 1. Hyperphagia 2. Hypersexuality 3. Hyperorality 4. Visual Agnosia (inability to recognize familiar objects or people) 5. Docility Lesion: Bilateral lesions of the medial temporal lobe. |
|
|
Neurofibromatosis 2: Name the Gene Name the Chromosome Name the Inheritance pattern |
Gene: Merlin (Tumor suppressor protein) Chromosome: 22 (q12.2) Inheritance pattern: Autosomal dominant |
|
|
Neurofibromatosis 1: Name 6 ophthalmic manifestations. |
1. Lisch nodules (melanocytic hamartomas that are usually yellow to brown and are dome shaped elevations projecting from the iris). 2. Plexiform neurofibromas (plexus like growth) 3. Choroid hamartomas (hamartoma = benign focal malformation that resembles a neoplasm) 4. Optic nerve gliomas (occur in 15-40% of children with NF1) 5. Prominent corneal nerves 6. Retinal tumors (e.g. astrocytic hamartomas, retinal capillary hemangiomas) |
|
|
Neurofibromatosis 2: Name 4 common tumor types |
1. Vestibular schwannoma (also referred to as acoustic schwannoma, but arises from the vestibular division) 2. Meningioma 3. Neurofibroma 4. Glioma 5. Other schwannomas |
|
|
Vertebral anatomy: What connects the body to the transverse processes? What connects the transverse processes to the spinous process? Where do the ribs articulate with the vertebrae? |
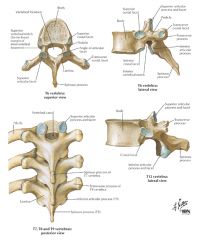
1. The body is connected to the transverse processes by the pedicles. 2. The transverse processes are connected to the spinous process by the lamina. 3. The ribs articulate at transverse costal facet on the transverse processes and at the superior and inferior costal facets on the body. image10 |
|
|
Which cranial nerves run through the lateral wall of the cavernous sinus from superior to inferior? Which cranial nerve runs through the middle of the cavernous sinus? |
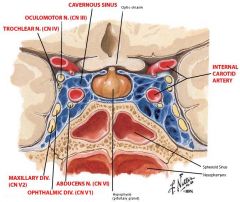
Lateral wall: Oculomotor nerve (most superior) Trochlear nerve V1 (ophthalmic division of CN 5) V2 (maxillary division of CN5, most inferior) Middle of the cavernous sinus Abducens nerve (alongside the internal carotid artery) image 11 |
|
|
What is the term for: 1. Motor restlessness / inability to sit still? 2. Impaired sense of taste? 3. What is the term for inability to recognize and interpret objects, people, sounds, or smells despite intact primary sense organs? |
1. Akathisia 2. Ageusia 3. Agnosia |
|
|
Phenytoin: 1. What is the mechanism of action? 2. What seizure types is it approved for? 3. Name 9 manifestations of phenytoin toxicity 4. What is the formula for additional IV doses of phenytoin to get the level into the therapeutic window? |
1. Sodium channel blocker (especially at high rates of firing) 2. Partial or generalized tonic-clonic seizures (primary or secondary) 3. Nystagmus, ataxia, dysarthria, diplopia, nausea, dizziness, drowsiness, cognitive difficulties, coma. 4. Additional IV dose (mg / kg) = 0.7 (desired concentration - measured concentration) |
|
|
Name the ten retinal layers from anterior to posterior (closest to the vitreous body to farthest away). |
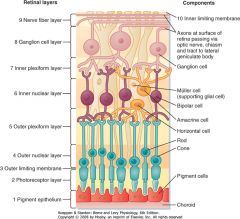
1. Inner limiting membrane (basement elaborated by Muller cells) 2. Nerve fiber layer (axons of the ganglion cell nuclei) 3. Ganglion cell layer (nuclei of the ganglion cell, axons become the optic nerve) 4. Inner plexiform layer (synapse between the bipolar cells and the dendrites of the ganglion and amacrine cells) 5. Inner nuclear layer (contains the nuclei of the bipolar, amacrine, and horizontal cells) 6. Outer plexiform layer (projections of rods and cones and synapses with the bipolar cell dendrites) 7. Outer nuclear layer (cell bodies of the rods and cones) 8. External limiting membrane (layer that separates the inner segment portions of the photoreceptors from their cell nucleus) 9. Layer of rods and cones (rod cells and cone cells) 10. Retinal pigment epithelium (single layer of cuboidal cells) image 14 |
|
|
What is the term for the following? 1. Lack of awareness of or indifference to to one's own neurological deficit, seen with non-dominant parietal lesions. 2. Inability to recognize part of one's own body seen with non-dominant parietal lobe lesions (less commonly with premotor cortex lesions). 3. Functional stance and gait characterized by bizarre movements, typically swaying wildly and nearly falling, but then recovering at the last minute. |
1. Anosognosia 2. Asomatognosia 3. Astasia-abasia |
|
|
What are the functional components of Cranial Nerve III (oculomotor nerve)? |
General Somatic Efferent: Innervation of the levator palpebrae superioris, superior rectus, medial rectus, inferior rectus, and inferior oblique muscles. General Visceral Efferent: Preganglionic parasympathetic fibers arise in the Edinger-Westphal nucleus and go on to innervate the ciliary ganglion (goes on to innervate the sphincter pupillae [pupil constriction], and ciliaris [makes lens more convex]) |
|
|
Huntington's Disease
1. Name the gene, chromosome, and gene product, and mode of inheritance.
2. Name the 3 main clinical features of the disease.
3. What structures are primarily affected and how?
4. What is seen on MRI and PET?
|
1. Gene: Huntingtin Chromosome: 4 (4p16.3), unstable expansion of CAG repeat sequence on exon 1 Gene product: Huntingtin protein: overexpressed, may play a role in endocytosis and intracellular trafficking (it is a component of microtubules and vesicle membranes) Mode of Inheritance: Autosomal Dominant (everyone with 40+ repeats develops disease)
2. Motor (Chorea, choreathetosis, dysphagia and dysarthria) Cognitive (deficits in frontal executive functions like judgment/planning/organization, poor attention and concentration, reduced verbal fluency) Psychiatric (Frontal lobe dysfunction causing apathy, disinhibition; depression; anxiety; psychosis)
3. Caudate and putamen are mainly involved - neuronal loss and gliosis with macroscopic atrophy
4. MRI: selective caudate (and possibly putaminal) atrophy PET: bilateral caudate hypometabolism may be an earlier and more sensitive marker.
|
|
|
Name the origin of the anterior choroidal artery. Name 7 structures supplied by the anterior choroidal artery. |
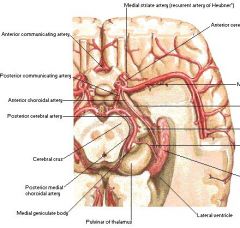
Origin: Internal carotid artery (rarely the MCA) Supplies: 1. Optic tract 2. Posterior limb of the internal capsule 3. Cerebral peduncle (red nucleus, substantia nigra) 4. Choroid plexus 5. Medial temporal lobe (hippocampus, amygdala) 6. Globus pallidus 7. Lateral geniculate body image 16 |
|
|
Huntington's Disease
1. Name the gene, chromosome, and gene product, and mode of inheritance.
2. Name the 3 main clinical features of the disease.
3. What structures are primarily affected and how?
4. What is seen on MRI and PET?
|
1. Gene: Huntingtin Chromosome: 4 (4p16.3), unstable expansion of CAG repeat sequence on exon 1 Gene product: Huntingtin protein: overexpressed, may play a role in endocytosis and intracellular trafficking (it is a component of microtubules and vesicle membranes) Mode of Inheritance: Autosomal Dominant (everyone with 40+ repeats develops disease)
2. Motor (Chorea, choreathetosis, dysphagia and dysarthria) Cognitive (deficits in frontal executive functions like judgment/planning/organization, poor attention and concentration, reduced verbal fluency) Psychiatric (Frontal lobe dysfunction causing apathy, disinhibition; depression; anxiety; psychosis)
3. Caudate and putamen are mainly involved - neuronal loss and gliosis with macroscopic atrophy
4. MRI: selective caudate (and possibly putaminal) atrophy PET: bilateral caudate hypometabolism may be an earlier and more sensitive marker.
|
|
|
Where does the superior oblique insert relative to the vertical axis? What are the primary, secondary, and tertiary actions of the superior oblique muscle? What is the innervation of the superior oblique muscle? |

Insertion: Behind and somewhat lateral to. Primary: Intorsion [Strongest in abduction] Secondary: Depression [This is strongest when the eye is adducted because the tendon pulls directly over the vertical axis so none of the action is dissipated in intorsion or abduction] Tertiary: Abduction Innervation: Trochlear Nerve (cranial nerve IV) image 18 |
|
|
Huntington's Disease 1. Name the gene, chromosome, and gene product, and mode of inheritance. 2. Name the 3 main clinical features of the disease. 3. What structures are primarily affected and how? 4. What is seen on MRI and PET? |
1. Gene: Huntingtin Chromosome: 4 (4p16.3), unstable expansion of CAG repeat sequence on exon 1 Gene product: Huntingtin protein: overexpressed, may play a role in endocytosis and intracellular trafficking (it is a component of microtubules and vesicle membranes) Mode of Inheritance: Autosomal Dominant (everyone with 40+ repeats develops disease) 2. Motor (Chorea, choreathetosis, dysphagia and dysarthria) Cognitive (deficits in frontal executive functions like judgment/planning/organization, poor attention and concentration, reduced verbal fluency) Psychiatric (Frontal lobe dysfunction causing apathy, disinhibition; depression; anxiety; psychosis) 3. Caudate and putamen are mainly involved - neuronal loss and gliosis with macroscopic atrophy 4. MRI: selective caudate (and possibly putaminal) atrophy PET: bilateral caudate hypometabolism may be an earlier and more sensitive marker. |
|
|
What does I VINDICATE stand for? |
I: Iatrogenic V: Vascular I: Infectious, Inflammatory N: Neoplastic D: Degenerative I: Idiopathic C: Congenital A: Autoimmune T: Trauma / Toxins E: Endocrine (metabolic) |
|
|
What are the functional components of Cranial Nerve V (trigeminal)? |
Special visceral efferent (innervate muscles of the pharyngeal arches in humans via trigeminal motor nucleus): Mastication muscles: masseter, temporal, medial pterygoid, lateral pterygoid. Other muscles: Tensor veli palanti, mylohyoid, anterior belly of the digastric, tensor tympani Mnemonic: My Tensors Dig Ants 4 My MoM General somatic afferent: Touch (via main sensory nucleus), proprioception (via mesencephalic nucleus), and pain/temperature (via spinal nucleus) for the face, mouth, nasal passages, anterior 2/3 of tongue, and the supratentorial dura mater. image 20 |
|
|
Lateral Medullary Syndrome: 1. Name 3 arteries that can be implicated 2. Name 7 symptoms including which side is affected and the affected structure. 3. Name the eponym. |
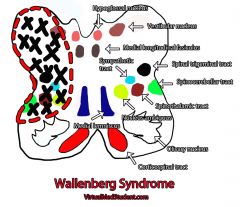
Arteries: 1. Vertebral artery distal branches 2. Superior lateral medullary artery (vertebral branch) 3. Posterior inferior cerebellar artery (less commonly) Symptoms: 1. Pain and temperature loss of ipsilateral face (spinal nucleus) 2. Arm and leg ataxia ipsilaterally (cerebellum) 3. Nystagmus ipsilaterally (vestibular nucleus) 4. Nausea/vomiting/vertigo ipsilaterally (vestibular nucleus) 5. Hoarseness/dysphagia ipsilaterally (nucleus ambiguus of the Vagus nerve) 6. Horner syndrome ipsilaterally (descending sympathetics) 7. Contralateral pain/temperature sensory loss (ascending spinothalamic tract) 3. Wallenberg syndrome image 21 |
|
|
1. What is the term for uncontrolled, often obsessive use of obscene language occasionally seen in Tourette syndrome?
2. What is the term for impaired ability to perform rapid alternating movements (e.g. pronation/supination of the forearm), which indicates cerebellar dysfunction?
3. What is the term for pain or discomfort in response to a stimulus (e.g. touch) that would not be expected to cause pain? |
1. Coprolalia
2. Dysdiadochokinesia
3. Dysesthesia |
|
|
1. What are the 5 components of the basal ganglia? 2. What makes up the striatum? 3. What makes up the lentiform nucleus? 4. Which is more lateral, the putamen or the globus pallidus? |
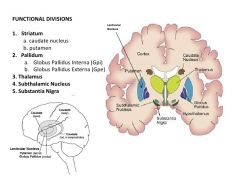
1. Caudate nucleus, putamen, globus pallidus (interna/externa), subthalamic nucleus, substantia nigra 2. Striatum = the caudate nucleus and putamen. 3. Lentiform nucleus = putamen and globus pallidus. 4. The putamen is most lateral, the globus pallidus interna is most medial. image 23 |
|
|
In a complete 3rd nerve palsy: 1. What direction does the eye go and why? 2. What is the status of the eyelid and pupil? 3. What is the topography of the parasympathetic fibers and the somatic fibers? |
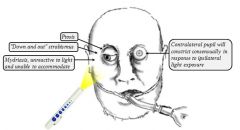
1. The eye will be down and out. Out because the lateral rectus is no longer opposed by the medial rectus. Down because of the unopposed depressive action of the superior oblique. 2. There will be ptosis due to palsy of the levator palpebrae superioris (superior branch of the 3rd nerve). There will be mydriasis (pupillary dilation) due to loss of the parasympathetic supply from the 3rd nerve. 3. The parasympathetic fibers run on the outside of the nerve. This is why in compressive lesions a pupillary abnormality may be seen before motor abnormalities. image 25 |
|
|
1. Where does the middle cerebral artery usually bifurcate into superior and inferior divisions? 2. What structures are supplied by the superior division of the MCA? 3. What structures are supplied by the inferior divisions of the MCA? |
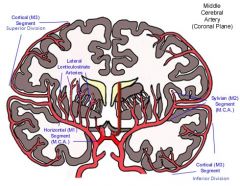
1. In the Sylvian fissure. 2. The superior division supplies the cortex above the sylvian fissure including the lateral frontal lobe and usually including the peri-Rolandic cortex. 3. The inferior division supplies the cortex below the Sylvian fissure including the lateral temporal lobe and a variable portion of the parietal lobe. image26 |
|
|
1. What does the superior cerebellar peduncle attach to? What are the two main tracts running through it? 2. What does the middle cerebellar peduncle attach to? What fibers does it carry? 3. What does the inferior cerebellar peduncle attach to? What fibers does it carry? |
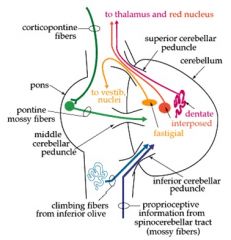
1. It attached to the midbrain. The two main tracts are the cerebellothalamic tract (efferent) to the contralateral thalamus and the cerebellorubral tract to the red nucleus. 2. The middle cerebellar peduncle attaches to the pons. It carries fibers from the pontine nuclei (which receive ipsilateral input from the primary motor cortex via the corticopontine fibers) to the contralateral cerebellar cortex via the pontocerebellar fibers. 3. It connects to the upper medulla. It carries afferent fibers from the posterior spinocerebellar tract (proprioceptive information from lower trunk and legs), cuneocerebellar tract (proprioceptive information from the arms and neck), trigeminocerebellar tract (proprioceptive information from the face), olivocerebellar tract (error signal in movement, comes from contralateral inferior olivary nucleus), and the vestibulocerebellar tract (vestibular information for the vestibular cerebellum) image 27 |
|
|
Internal Capsule: 1. What is the blood supply to the (a) anterior limb; (b) genu; (c) posterior limb? 2. What fibers run through the anterior limb? 3. What fibers run through the genu? 4. What fibers run through the posterior limb? |
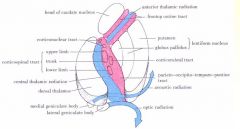
1. (a) lenticulostriate branches of the middle cerebral artery (superior half) and recurrent artery of Heubner from the anterior cerebral artery (inferior half); (b) lenticulostriate branches middle cerebral artery; (c) lenticulostriate branches of the middle cerebral artery (superior half) and anterior choroidal artery (inferior half) 2. Anterior thalamic radiation, frontopontine tract (to the nuclei pontis) 3. Corticobulbar tract 4. Corticospinal tract (arm/thorax/leg from ventral to dorsal), corticorubral tract, central thalamic tract, optic radiations, acoustic radiations from the medial geniculate nucleus to the temporal lobe. image 28 |
|
|
1. Where does the superior rectus insert relative to the vertical axis? 2. What are the actions of the superior rectus muscle? 3. What is the innervation of the superior rectus muscle? |

1. Its insertion is anterior to and somewhat medial to the vertical axis. 2. Primary action is elevation (strongest when abducted). Secondary action is intorsion (when adducted) Tertiary action is adduction (in primary gaze due to the insertion being medial to the vertical axis) 3. It is innervated by the superior division of the oculomotor nerve. image30 |
|
|
Name the 4 primary clinical features of Supranuclear Palsy |
1. Supranuclear ophthalmoplegia (vertical saccades, especially downward, are affected more than horizontal movements. Saccades affected more than pursuit.) 2. Parkinsonism and early falls (hyperextended posture during walking, impaired reflexes with retropulsion) 3. Pseudobulbar palsy (emotional incontinence, drooling, increased jaw jerk) 4. Cognitive disturbance (frontal release signs, personality change, frontal-executive dysfunction). |
|
|
Broca's Aphasia: 1. Where is the lesion? 2. Characteristics: Fluency Naming Comprehension Repetition Paraphasic Errors |
1. Damage to the inferior and middle posterior frontal lobe (Broca's area) 2. Fluency: Nonfluent Naming: Impaired Comprehension: Intact Repetition: Impaired Paraphasic Errors: Rare |
|
|
Transcortical Motor Aphasia: 1. Where is the lesion? 2.Characteristics: Fluency Naming Comprehension Repetition Paraphasic Errors |
1. Areas anterior and superior to Broca's area and in the subcortical white matter. 2. Fluency: Nonfluent Naming: Impaired Comprehension: Intact Repetition: Intact Paraphasic Errors: Rare |
|
|
Wernicke's Aphasia: 1. Where is the lesion? 2. Characteristics: Fluency Naming Comprehension Repetition Paraphasic Errors |
1. Posterior 2/3 of the superior temporal gyrus (auditory association cortex) 2. Fluency: Fluent Naming: Impaired Comprehension: Impaired Repetition: Impaired Paraphasic Errors: Common |
|
|
Trancsortical Sensory Aphasia: 1. Where is the lesion? 2. Characteristics: Fluency Naming Comprehension Repetition Paraphasic Errors |
1. Lesions of the posterior middle temporal gyrus, angular gyrus, and corresponding deep white matter. 2.Fluency: Fluent Naming: Impaired Comprehension: Impaired Repetition: Intact Paraphasic Errors: Common |
|
|
What are the functional components of the VI cranial nerve (abducens)? |
General somatic efferent: Supplies the lateral rectus of the eye. Image 32 |
|
|
What are the functional components of the VII cranial nerve (facial)? |
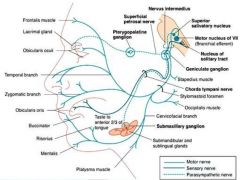
1. Branchial motor (special visceral efferent): Supply the stapedius, stylohyoid, posterior belly of the digastric, facial expression muscles, buccinator, platysma, and occipitalis. 2. Visceral motor (General visceral efferent): For stimulation of the lacrimal, submandibular, and sublingual glands, as well as the mucous membrane of the nose, and the hard and soft palates. 3. General sensory (General somatic afferent): To supply the skin of the concha of the auricle, a small area of skin behind the ear, and possibly to supplement V3, which supplies the wall of the acoustic meatus and external tympanic membrane. 4. Special sensory (Special afferent): For taste from the anterior two-thirds of the tongue and the hard and soft palates. |
|
|
Cluster Headache Treatment
1. Name 4 abortive treatments
2. Name 5 prophylactic treatments. |
1. Oxygen (7-10 L/minute for 15 minutes)
2. Sumatriptan (6 mg subcutaneously effective in most patients)
3. Lidocaine (intranasal lidocaine drops may help).
4. Dihydroergotamine (DHE): 1 mg intramuscularly or intravenously is rapidly effective.
Prophylactic treatments: Verapamil, ergotamine, lithium carbonate, methysergide, valproic acid.
|
|
|
Cluster Headache 1. How long do cluster periods usually last? 2. How frequent are attacks and how long do they last? 3. Describe the pain/patient behavior. 4. Name 8 associated symptoms. |
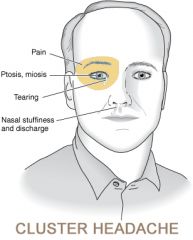
1. Weeks to months separated by remissions. 2. Attacks within a cluster may occur daily or several times daily. Length = 15-180 minutes. 3. Unilateral, orbital or temporal and severe. Patients tend to pace. 4. Conjunctival injection, lacrimation, nasal congestion, rhinorrhea, forehead/facial sweating, miosis, ptosis, eyelid edema. image 34 |
|
|
Cluster Headache Treatment 1. Name 4 abortive treatments 2. Name 5 prophylactic treatments. |
1. Oxygen (7-10 L/minute for 15 minutes) 2. Sumatriptan (6 mg subcutaneously effective in most patients) 3. Lidocaine (intranasal lidocaine drops may help). 4. Dihydroergotamine (DHE): 1 mg intramuscularly or intravenously is rapidly effective. Prophylactic treatments: Verapamil, ergotamine, lithium carbonate, methysergide, valproic acid. |
|
|
Tension Type Headache: 1. Location 2. Quality 3. Severity 4. Associated symptoms 5. Precipitating factors 6. Abortive treatment 7. Prophylactic treatment |
1. Location = bilateral occipital, frontal, or frontal-occipital, but may occur in any location 2. Quality = dull ache or pressure 3. Severity = mild-moderate 4. Associated symptoms = tenderness to palpation, absence of nausea/vomiting/photophobia, not aggravated by physical activity 5. Precipitating factors = sleep deprivation 6. Abortive treatment = NSAIDs, ASA, Tylenol 7. Tricyclic antidepressants, AEDs (especially topiramate, gabapentin, valproic acid), SSRIs, beta blockers, calcium channel blockers |
|
|
1. What is the definition of glial cells? 2. What are astrocytes and what are their functions? 3. What are microglia and what is their function? |
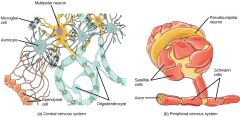
1. Glia are non-neuronal cells that maintain homeostasis, form myelin, and provide support and protection for neurons in the central and peripheral nervous systems. They include oligodendrocytes, astrocytes, microglia, and ependymal cells in the CNS. They include Schwann cells and satellite cells in the PNS. 2. Astrocytes are characteristic star-shaped glial cells in the brain and spinal cord. They make up 20-40% of all glial cells. Functions include biochemical support of endothelial cells, provision of nutrients to nervous tissue, maintenance of extracellular ion balance, roles in the repair/scarring process of the CNS. 3. Microglia are the resident macrophages of the brain and spinal cord. They make up 10-15% of all brain cells. Their function is to scavenge the CNS for plaques, damaged or unnecessary neurons and synapses, and infectious agents. image 36 |
|
|
1. What are the 3 anatomic divisions of the cerebellum and where do they receive their input from? |

Anterior Lobe: Anterior to the primary fissure, receives majority of input from the spinocerebellar tracts. Posterior Lobe: Between the primary and dorsolateral fissures. Receives majority of input from the neocortex. Flocculonodular lobe: Receives input from the vestibular nuclei. image 37 |
|
|
What are the 3 functional subdivisions of the cerebellum? What part of the cerebellum composes them? What is their function? |
1. Vestibulocerebellum: Flocconodular lobe. -Orients eye movements during movement -Coordinates position of the head and limbs in response to position and motion through connections with the medial and lateral vestibulospinal tracts -Has a role in smooth pursuit 2A. Spinocerebellum: Vermis - Monitors ongoing execution of movement (especially proximal limbs and axial musculature) -Role in maintenance of muscle tone 2B. Spinocerebellum: Paravermis - Monitors ongoing execution of limb movements - Postural tone - Modulates descending motor systems 3. Cerebrocerebellum: Lateral cerebellar hemispheres (posterior lobes) - Initiation, planning, and timing of movement: precision in control of rapid movements and conscious assessment of errors in movement (fine dexterity) |
|
|
Paraneoplastic Syndromes. ANNA-1 (anti-Hu): 1. What does ANNA-1 stand for? 2. What is the antigen? 3. What neoplasm is usually seen? 4. Name 6 neurologic syndromes seen with it. |
1. Anti-neuronal nuclear antibody 2. Nucleus, all neurons. 3. Small cell lung carcinoma 4. Encephalomyelitis, cerebellar degeneration, sensory neuronopathy, autonomic neuropathy, mononeuritis multiplex, sensorimotor neuropathy |
|
|
What are the functional components of the vestibulocochlear nerve (Cranial Nerve 8)? |
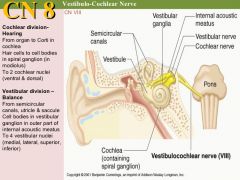
1. Special sensory afferent: auditory information from the cochlea 2. Special sensory afferent: balance information from the semicircular canals image39 |
|
|
What are the primary muscle(s) for the following movements? 1. Up and abducted. 2. Abducted 3. Down and abducted. 4. Up. 5. Down. 6. Converged. 7. Up and adducted. 8. Adducted. 9. Down and adducted. |
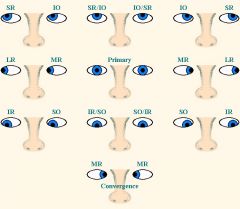
1. Superior rectus (up and abducted). 2. Lateral rectus (abducted). 3. Inferior rectus (down and abducted). 4. Superior rectus / inferior oblique (up). 5. Inferior rectus / superior oblique (down). 6. Medial rectus (converged). 7. Inferior oblique (up and adducted). 8. Medial rectus (adducted). 9. Superior oblique (down and adducted). Image 40 |
|
|
1. What are the classic features of Miller Fisher Syndrome? 2. What four antibodies have been described with Guillain Barre syndrome? 3. Which antibody is linked with the Miller Fisher variant? |
1. (a) Ataxia, (b) ophthalmoplegia, (c) areflexia 2. Ganglioside antibodies to GM1, GD1A, GT1A, and GQ1b. 3. GQ1b (elevated in 80% of cases). |
|
|
Acid Maltase Deficiency 1. What is the affected gene product? 2. What is the inheritance pattern? 3. What is the muscle pathology? 4. What is the age of onset and what determines the age of onset? |
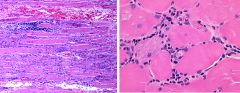
1. Acid alpha glucosidase, which is a lysosomal hydrolase. 2. Autosomal recessive. 3. Small amounts of glycogen are normally present and degraded to glucose by lysosomal acid maltase. But if acid maltase is deficient, glycogen accumulates in lysosomes and cytoplasm and can cause muscle fiber damage from intracellular glycogen accmulation and possibly lysosomal rupture with enzyme release. 4. Severe infantile form (Pompe's disease, first few months of life), childhood (first decade of life) or Adult onset (usually by 3rd-4th decade). Determined by the amount of residual enzyme activity. image 45 |
|
|
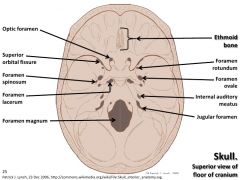
Name the 10 major bones of the skull. |
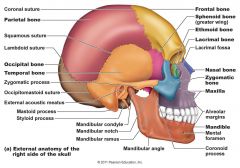
1. Frontal bone 2. Zygomatic bone 3. Maxilla 4. Mandible 5. Ethmoid bone. 6. Lacrimal bone. 7. Sphenoid bone. 8. Temporal bone. 9. Parietal bone. 10. Occipital bone. image 42 |
|
|
Acid Maltase Deficiency 1. What is the affected gene product? 2. What is the inheritance pattern? 3. What is the muscle pathology? 4. What is the age of onset and what determines the age of onset? |

1. Acid alpha glucosidase, which is a lysosomal hydrolase. 2. Autosomal recessive. 3. Small amounts of glycogen are normally present and degraded to glucose by lysosomal acid maltase. But if acid maltase is deficient, glycogen accumulates in lysosomes and cytoplasm and can cause muscle fiber damage from intracellular glycogen accmulation and possibly lysosomal rupture with enzyme release. 4. Severe infantile form (Pompe's disease, first few months of life), childhood (first decade of life) or Adult onset (usually by 3rd-4th decade). Determined by the amount of residual enzyme activity. image 45 |
|
|
What are the clinical features of acid maltase deficiency? |
1. Severe infantile form: Cardiomegaly, macroglossia, hepatomegaly, progressive weakness/hypotonia, death. 2. Childhood: Delayed motor development, slowly progressive proximal muscle weakness, respiratory muscle weakness, calf hypertrophy. Respiratory failure usual cause of death. 3. Adult-onset: Proximal muscle weakness and atrophy with possible face/tongue involvement. Almost all eventually have respiratory involvement, which leads to death. Possible macroglossia. |
|
|
Where does the inferior oblique insert relative to the Y axis? What are the primary, secondary, and tertiary movements of the inferior oblique? |
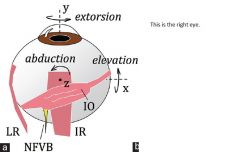
1. Posterior and lateral to. 2. Extorsion (strongest in abduction) Elevation (strongest in adduction) Abduction (strongest in primary position) image 44 |
|
|
Friedreich's Ataxia 1. What is the usual mutation and what is the gene product? 2. What age does it usually start and with what signs? 3. What is the prognosis? 4. Name 3 manifestations outside the nervous system. |
1. GAA triplet repeat in the FRDA gene causing decreased frataxin protein expression. May cause excess intramitochondrial iron and subsequent oxidative stress. 2. Puberty -- gait disorder and clumsiness 3. Slow, variable progression. Age at death is usually late 30s. Wheelchair dependent usually by 2nd decade. 4. Skeletal abnormalities (kyphoscoliosis, pes cavus, pes planus, equivarus), diabetes mellitus, hypertrophied cardiomyopathy/subaortic stenosis. |
|
|
Where do the cervical nerve roots exit relative to their corresponding vertebrae? What about thoracic and lumbar nerve roots? |

Cervical nerve roots go out above their corresponding vertebra (e.g. C2 nerve root exits at C1-C2, C8 exits at C7-T1). Thoracic nerve roots exit below their corresponding vertebra (e.g. T1 exits at T1-T2, T12 exits at T12-L1). Lumbar roots similarly exit below corresponding vertebra. image 48 |
|
|
Dermatomyositis 1. How is the rash described? 2. When does the rash occur? 3. Where is the rash located? |

1. A heliotrope rash, after the violet color of the heliotrope plant. 2. Accompanies or precedes weakness. 3. Periorbital regions (with edema), anterior neck and upper chest (V sign), shoulders (shawl sign), buttocks, knuckles, elbows, knees, extensor surfaces of fingers (Gottron's sign) image 49 |
|
|
Dermatomyositis 1. What is the pattern of muscle weakness/myalgias? 2. Name 3 cardiac manifestations. 3. Name 4 other systems that may be affected. |

1. Proximal pattern. 2. Pericarditis, myocarditis, cardiomyopathy with CHF. 3. Interstitial lung disease, GI, Renal, Joints (arthralgias). image 50 |
|
|
Red Nucleus 1. Where is it located? 2. Why is it red? 3. What is its function in vertebrates without a corticospinal tract? 4. Where do its inputs come from? 5. Where do its efferents go? |
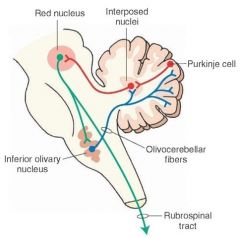
1. It is located in the rostral midbrain, somewhat medial and dorsal to the substantia nigra. 2. Due to the presence of iron. 3. It controls walking. It is vestigial in humans but does control crawling in babies. 4. The contralateral cerebellum and the ipsilateral motor cortex. 5. Inferior olive of the same side (ultimately influences the cerebellum). Also, to the rhomboencephalic reticular formation and spinal cord of the contralateral side to form the rubrospinal tract (largely vestigial in humans). image 52 |
|
|
1. What is the characteristic muscle histopathology finding in dermatomyositis? 2. What treatment strategies are used for dermatomyositis? |
1. The pathology of dermatomyositis includes inflammation, vasculitis, and perifascicular atrophy. The inflammatory cells are predominantly B-cells (with smaller numbers of CD4-positive T-cells) and are found around blood vessels, in the septa between muscle fascicles, and in fibroadipose tissue around muscle. The key pathological change of dermatomyositis is a vasculitis, which involves endomysial and perimysial capillaries and arterioles. 2. Corticosteroids, steroid sparing agent (azathioprine or methotrexate), rituximab, Plaquenil for rash. |
|
|
Adrenoleukodystrophy 1. What is the inheritance pattern? 2. What does the ALD gene code for? 3. What is the pathology of the disease? 4. How does it affect the brain and spinal cord? |
1. X-linked recessive. 2. A peroxisomal membrane protein with homology to ATP binding cassette transporter superfamily of proteins. 3. Very long chain fatty acids accumulate in the brain, plasma, and adrenal glands leading to membrane instability (cause of accumulation unclear). 4. There is a rapidly progressively inflammatory myelinopathy in the parieto-occipital region of the brain (possibly autoimmune). There is a noninflammatory distal axonopathy of the spinal cord tracts and, less so, of the peripheral nerves. image 53 |
|
|
1. Where are the raphe nuclei? 2. How many raphe nuclei are there? 3. Name 3 functions of the raphe nuclei. |
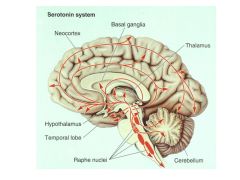
1. The raphe nuclei are the medial part of the reticular formation. The reticular formation is central and dorsal in the brainstem. The raphe nuclei extend throughout the entire brainstem. 2. Seven (2 in the midbrain, 2 in the pons, and 3 in the medulla). 3. 1. Supply the brain with serotonin which is involved in modulating the motor/somatosensory/limbic systems. 2. Projections terminate in the dorsal horn of the spinal cord and regulate release of enkephalins 3. Involved in a feedback loop with the suprachiasmatic nucleus - serotonin is involved in the sleep/wake cycle. image 54 |
|
|
1. Name 5 types of glial tumors. 2. Name 6 types of Neuroepithelial tumors with neuronal features. 3. Name 6 types of primitive neuroectodermal tumors (PNETs) |
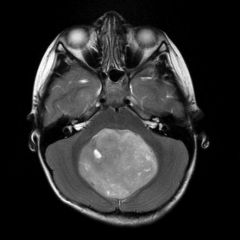
1. Astrocytoma, oligodendroglioma, mixed oligoastrocytoma, pleomorphic xanthoastrocytoma, ependymoma 2. Ganglion cell neoplasms, central neurocytomas, dysembryoplastic neuroepithelial tumor (DNET), Dysplastic gangliocytoma of the cerebellum (Lhermitte-Duclos Disease), Desmoplastic infantile astrocytoma (DIA), and desmoplastic infantile ganglioma (DIG). 3. Medulloblastoma, Ependymoblastoma, Esthesioblastoma, Pinealblastoma, retinoblastoma, cerebral neuroblastoma (aka supratentorial PNET). image 57 (medulloblastoma) |
|
|
Prognostication after CPR 1.) What are some potential confounding factors? 2.) What signs on Day 1 are indicators of a poor outcome? 3.) What signs on Day 3 are indicators of a poor outcome? 4.) What is a poor outcome defined as? |
1.) Hypothermia, use or prior use of sedatives, use or prior use of neuromuscular blocking agents, organ failure (acute renal, or liver failure), shock (especially cardiogenic shock requiring inotropes). 2.) Serum NSE > 33 micrograms/mL (days 1-3, FPR = 0%). Myoclonus status epilepticus (day 1, FPR = 0%) SSEP absent N20 response (days 1-3, FPR = 0.7%) 3.) Absent pupil or corneal reflexes. Extensor or absent motor responses. 4.) Death, unconsciousness after one month, or unconsciousness/severe disability after six months.
|
|
|
Recurrent artery of Heubner 1. From what vessel does it arise? 2. What structures does it supply? |
1. The anterior cerebral artery. It arises from either the distal A1 or proximal A2 segment. 2. It supplies the anteromedial portion of the caudate nucleus, the anterior putamen, and parts of the globus pallidus. It also supplies the inferior portion of the anterior limb of the internal capsule. image 58 |
|

Name the structures in this picture: image 43a |
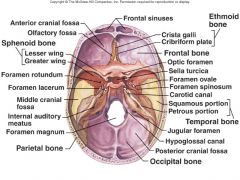
image 43 |
|
|
Posterior Choroidal Artery
1. Where does it arise from?
2. How many are there?
3. What is supplied by the medial posterior choroidal artery?
4. What is supplied by the lateral posterior choroidal artery?
|
1. It usually arises from the P2 segment of the posterior cerebral artery.
2. There are often up to 10 branches. They are grouped into the medial posterior choroidal artery and the lateral posterior choroidal arteries.
3. The midbrain tegmentum, posterior thalamus, pineal gland, and the choroid plexus of the 3rd ventricle.
4. The choroid plexus of the lateral ventricle.
image 61 |
|
|
Lamotrigine
1. What spectrum of seizure types can be treated?
2. What are the mechanisms of action?
3. Name 5 possible side effects.
4. What monitoring is necessary? |
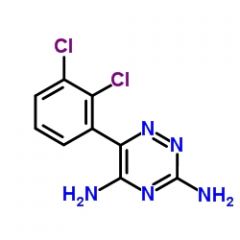
1. Partial, generalized tonic-clonic, absence, myoclonic, tonic, and atonic.
2. Inhibits sodium channels, especially at high rates of firing (like phenytoin and carbamazepine) and inhibits glutamate release.
3. Rash, dizziness, ataxia, blurred vision, diplopia.
4. No monitoring is needed. |
|
|
Posterior Choroidal Artery 1. Where does it arise from? 2. How many are there? 3. What is supplied by the medial posterior choroidal artery? 4. What is supplied by the lateral posterior choroidal artery? NEEDS PICTURE. |

1. It usually arises from the P2 segment of the posterior cerebral artery. 2. There are often up to 10 branches. They are grouped into the medial posterior choroidal artery and the lateral posterior choroidal arteries. 3. The midbrain tegmentum, posterior thalamus, pineal gland, and the choroid plexus of the 3rd ventricle. 4. The choroid plexus of the lateral ventricle. image 61 |
|
|
What is the difference between positive and negative myoclonus? |
1. Positive myoclonus is a sudden, brief, involuntary movement caused by contraction of certain muscle groups. Negative myoclonus is the same caused by inhibition of certain muscle groups (e.g. asterixis). |
|
|
Inclusion Body Myositis 1. What is the usual age of onset? 2. What is the pattern of weakness? 3. What are the usual CK levels? 4. Is there atrophy? |
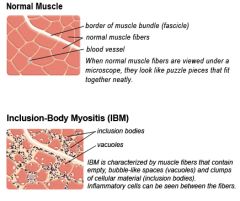
1. >30 years. 2. Both proximal and distal musculature is affected. Finger/wrist flexors (more than extensors) and quadriceps are often affected. 3. Normal or slightly elevated in 80% of patients. 4. Yes, often proportional to the weakness. |
|
|
Inclusion Body Myositis 1. What treatments are commonly used? 2. Do they work? |
1. Prednisone, methotrexate, and azathioprine are commonly used. IVIG is not recommended due to its expense and modest benefits. 2. IBM is not very responsive to immunosuppressive therapy. If there is no clinical worsening, this is often considered a success as improvement is not often seen. |
|
|
What are the functional components of the 9th (Glossopharyngeal) cranial nerve? |
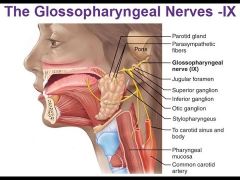
1. Special visceral efferent: Supplies the stylopharyngeus 2. General visceral efferent Supplies the otic ganglion, which sends fibers to stimulate the parotid gland. 3. General visceral afferent Carries sensory information (subconscious) from the carotid body and from the carotid sinus. 4. General somatic afferent Provides general sensation from the posterior one-third of the tongue, the skin of the external ear, and the internal surface of the tympanic membrane. 5. Special afferent Stimulates taste receptors in the posterior one-third of the tongue. |
|
|
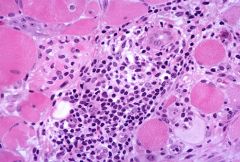
1. Which neurofibromatosis is associated with cafe au lait spots and what percentage of patients have them? 2. Name 3 other conditions where cafe au lait spots may be seen? 3. Can cafe au lait spots be seen in infancy? 4. What causes cafe au lait spots? |

1. Neurofibromatosis type 1. 95%. 2. Tuberous sclerosis, Fanconi anemia, and McCune-Albright syndrome. 3. They are most visible after age 2. They are faint in infants, but may be better appreciated with a Wood lamp. 4. An increase in melanin, typically with giant melanosomes. image 63 |
|
|
1. What does RCVS Stand for? 2. What are possible secondary causes of RCVS? |
1. Reversible cerebral vasoconstriction syndrome. 2. Vasoactive substances, blood products, and the postpartum state. (these are thought to be the cause 60% of the time) |
|
|
1. What is the primary symptom of RCVS? 2. What percentage of patients with RCVS do not have headache? 3. What complications are sometimes seen? |
1. Thunderclap headache (reaches peak intensity within seconds). Tends to recur over a span of days to weeks. 2. Less than 10 percent. 3. About 1/3 of patients have hemorrhagic or ischemic infarcts or cerebral edema. |
|
|
1. What is the primary diagnostic feature of RCVS? 2. Name 4 frequent other pathologies seen. |
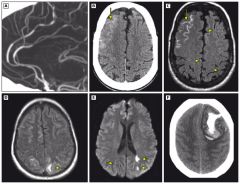
1. Abnormal cerebral angiography. Cerebral angiographic abnormalities are dynamic and progress proximally, resulting in a "sausage on a string" appearance of the circle of Willis arteries and their branches. Smooth, tapered narrowing followed by abnormal dilated segments of second- and third-order branches of the cerebral arteries is the most characteristic abnormality. 2. Ischemic stroke, cortical surface subarachnoid hemorrhage, reversible vasogenic brain edema, parenchymal hemorrhage. image 65 |
|
|
1. What is the treatment for RCVS? 2. What is the prognosis for RCVS? |
1. Supportive care only - no other treatment is known to be effective. 2. Most patients with RCVS have complete resolution of headaches and angiographic abnormalities within days to weeks. Less than 15 to 20 percent are left with residual deficits from stroke, and in most cases the deficits are relatively minor (ie, 90 to 95 percent have a modified Rankin scale score of 0 to 2 at discharge). Progressive vasoconstriction resulting in progressive symptoms or death can occur in rare cases. |
|
|
Neuroleptic Malignant Syndrome (NMS) 1. Name 5 early signs of neuroleptic malignant syndrome 2. What causes NMS? 3. What is its association with Parkinson medications? |
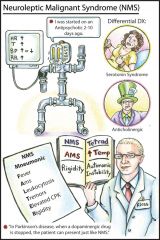
1. Muscle cramps, tremors, fevers, autonomic instability (e.g. unstable blood pressure), and mental status changes. 2. The cause is unknown, but it occurs in people taking neuroleptic agents. Every class of neuroleptics has been implicated, but it is most commonly seen with the "typical" agents such as haloperidol and fluphenazine. 3. It can sometimes be seen with withdrawal of antiparkinson medications, reductions in dose, or when switching from one agent to another. image 67 |
|
|
1. What is the most important intervention in neuroleptic malignant syndrome? 2. Name 3 potential pharmacologic treatments for NMS. 3. What is another potential treatment for NMS? |
1. Stop the neuroleptic. 2. Dantrolene (skeletal muscle relaxant that helps in malignant hyperthermia). Can cause liver toxicity. Bromocriptine (restore lost dopaminergic tone) Amantadine (alternative to bromocriptine) 3. Electroconvulsive therapy |
|
|
1. What is the classic laboratory abnormality in neuroleptic malignant syndrome? 2. Name 5 other potential laboratory disturbances. |
1. Elevated CK (often 1,000-100,000). 2. Leukocytosis, electrolyte abnormalities, transaminitis, elevated LDH, low serum iron. |
|
|
Serotonin syndrome 1. What is the triad of clinical symptoms? |
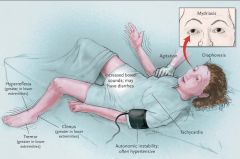
Triad 1. Cognitive: Confusion, hallucinations, agitation, hallucinations 2. Autonomic: Hyperthermia (can be higher than 106F), shivering, sweating, nausea, diarrhea, tachycardia 3. Somatic: Myoclonus, hyperreflexia, tremor. image 68 |
|
|
Lennox-Gastaut Syndrome
1. What is the clinical triad?
2. What is the usual age of onset?
3. Who's affected more commonly, boys or girls? |
1. Mental retardation, multiple seizure types, characteristic slow spike-and-wave (2 Hz) EEG
2. 2-8 years old.
3. Boys |
|
|
Lennox-Gastaut Syndrome
1. What is the clinical triad?
2. What is the usual age of onset?
3. Who's affected more commonly, boys or girls? |
1. Mental retardation, multiple seizure types, characteristic slow spike-and-wave (2 Hz) EEG
2. 2-8 years old.
3. Boys |
|
|
What are the functional components of the glossopharyngeal nerve (Cranial Nerve 9)? |

Branchial Motor: Supply the stylopharyngeus. Visceral Motor: Supply the otic ganglion, which sends fibers to stimulate the parotid gland. Visceral sensory: Caries sensation (subconscious) from the carotid body and from the carotid sinus. General Sensory: Provides general sensation from the posterior 1/3 of the tongue, the skin of the external ear, and the internal surface of the tympanic membrane. Special sensory: Stimulates taste receptors in the posterior 1/3 of the tongue. image 69 |
|
|
Lennox-Gastaut Syndrome Name four common seizure types in addition to drop attacks. |
1. Tonic seizures (last a few seconds) 2. Atypical absence seizure (gradual onset/offset unlike typical absence seizures) 3. Atonic seizure (neck only or whole body) 4. Generalized tonic-clonic seizures. |
|
|
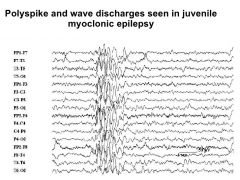
Juvenile Myoclonic Epilepsy 1. When do the seizures occur? 2. What are the myoclonic seizures like? 3. Are other seizure types observed? |
1. Usually predominantly upon awakening (can be triggered by sleep deprivation, alcohol, and photic stimulation). 2. Large-amplitude, bilateral, and simultaneous (both arms or both legs, usually focal). 3. Most patients have less frequent generalized tonic-clonic seizures and some have typical absence seizures. |
|
|
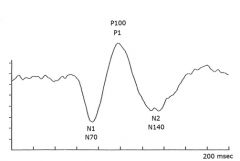
Visual evoked potentials
1. What are the 3 wave forms?
2. What portion of the visual system do VEPs have high sensitivity for?
3. What is the interpretation of bilateral P1 abnormalities? |
1. N1 (N75) = initial negative deflection P1 (P100) = positive deflection (most important) N2 (N145) = second negative deflection
2. High sensitivity for anterior visual pathway lesions (pre-chiasmal). Poor sensitivity for lesions of the postchiasmal and cortical visual pathways.
3. Bilateral P1 abnormalities are nonlocalizing. They may be seen with chiasmal, postchiasmal, or bilateral prechiasmal lesions. NOTE: The untested eye is covered during testing.
image 73 |
|
|
Visual evoked potentials 1. What are the 3 wave forms? 2. What portion of the visual system do VEPs have high sensitivity for? 3. What is the interpretation of bilateral P1 abnormalities? |
1. N1 (N75) = initial negative deflection P1 (P100) = positive deflection (most important) N2 (N145) = second negative deflection 2. High sensitivity for anterior visual pathway lesions (pre-chiasmal). Poor sensitivity for lesions of the postchiasmal and cortical visual pathways. 3. Bilateral P1 abnormalities are nonlocalizing. They may be seen with chiasmal, postchiasmal, or bilateral prechiasmal lesions. image 73 |
|
|
Von Hippel Lindau Disease 1. What is the inheritance pattern? 2. What are the hallmark lesions? 3. How do hemangioblastomas cause symptoms? |
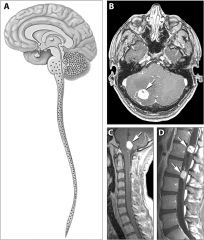
1. Autosomal Dominant 2. Retinal, cerebellar, and spinal cord hemangioblastomas. 3. The lesions are well-circumscribed, highly vascular, benign neoplasms. They cause symptoms due to mass effect from hemorrhage. image 76 |
|
|
Von Hippel Lindau Disease 1. What are the 7 main features of this disease? |
1. Hemangioblastomas of the central nervous system and retina. 2. Renal cell carcinomas (most patients die from this, median survival = 49 years) 3. Pheochromocytomas 4. Pancreatic islet cell tumors. 5. Endolymphatic sac tumors of the middle ear 6. Serous cystadenomas and neuroendocrine tumors of the pancreas 7. Papillary cystadenomas of epididymis and broad ligament. image 75 |
|
|
McArdle's Disease (Type V glycogenosis) 1. What is the deficient enzyme? 2. What are the main symptoms? 3. What is the usual age of onset? |
1. Myophosphorylase deficiency (is involved in degrading glycogen chains). 2. Exercise intolerance, myalgias, and cramps. 3. First decade (male predominance) |
|
|
McArdle's Disease (Type V glycogenosis)
1. How is the diagnosis established?
2. What does EMG show?
3. What is the treatment? |
1. Ischemic forearm test: blood pressure cuff placed, then 1 minute of rapid hand opening/closing, then measure ammonia/lactate levels. If there is a 3-5 order increase in ammonia levels with no change in lactate levels, this suggests a glycolytic disorder.
2. Often normal between episodes (decremental response after brief exercise due to energy failure and electrical silence of some muscle fibers).
3. High protein diet. Better exercise tolerance may be achieved with administration of oral glucose or fructose loads or glucagon administration. |
|
|
McArdle's Disease (Type V glycogenosis)
1. How is the diagnosis established?
2. What does EMG show?
3. What is the treatment? |
1. Ischemic forearm test: blood pressure cuff placed, then 1 minute of rapid hand opening/closing, then measure ammonia/lactate levels. If there is a 3-5 order increase in ammonia levels with no change in lactate levels, this suggests a glycolytic disorder.
2. Often normal between episodes (decremental response after brief exercise due to energy failure and electrical silence of some muscle fibers).
3. High protein diet. Better exercise tolerance may be achieved with administration of oral glucose or fructose loads or glucagon administration. |
|
|
Caloric Reflex Testing 1. What happens when cold calorics are done on an awake patient? 2. Is there nystagmus in a comatose patient? |
1. Based on cerebral input, the awake patient will compensate for the eye movements with fast saccades back to the midline. 2. There should not be -- the presence of nystagmus suggests the patient is only pretending to be comatose. |
|
|
Caloric Reflex Testing
1. What happens when cold calorics are done on an awake patient?
2. Is there nystagmus in a comatose patient?
|
1. Based on cerebral input, the awake patient will compensate for the eye movements with fast saccades back to the midline.
2. There should not be -- the presence of nystagmus suggests the patient is only pretending to be comatose. |
|
|
1. How is the Rinne test performed? 2. How is the Rinne test interpreted? |

1. Place the tuning fork on the mastoid process behind each ear until sound is no longer heard. Then place the fork immediately outside the ear and ask the patient to note when the vibration is no longer heard. 2. A normal (positive) test is when the tuning fork is heard better by the ear than on the bone (air conduction > bone conduction). An abnormal test is when the bone conduction is heard better and suggests a conductive hearing loss (a negative Rinne) |
|
|
1. What are the two defining features of Sturge Weber syndrome? 2. Name 4 possible neurologic features. 3. Name two possible ophthalmological features. |

1. A port wine stain (characterized by a facial capillary malformation along the ophthalmic branch of the trigeminal nerve) and an associated leptomeningeal capillary-venous malformation (leptomeningeal angioma) 2. Seizures, mental retardation, hydrocephalus, focal neurologic deficits. 3. Glaucoma and visual field defects (when the occipital cortex is affected). |
|
|
Sympathetic innervation of the eye
1. What is the path of the first order neuron?
2. What is the path of the second order neuron?
3. What is the path of the third order neuron?
4. Where do the vasomotor and sweat fibers branch off? |
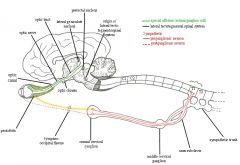
1. It originates in the posterior hypothalamus and descends through the brainstem to the first synapse, located in the lower cervical and upper thoracic cord (C8-T2)
2. These preganglionic neurons exit the spinal cord, travel near the apex of the lung, under the subclavian artery, and ascend the neck and synapse in the superior cervical ganglion, near the bifurcation of the carotid artery at the level of the angle of the mandible.
3. These postganglionic neurons travel with the carotid artery through the cavernous sinus to the orbit, where they travel with the ophthalmic division of the trigeminal nerve to their destinations.
4. They branch off at the superior cervical ganglion near the level of the carotid bifurcation and travel to the face with the ECA. |
|
|
1. How are cocaine eye drops used to test for Horner's syndrome? |
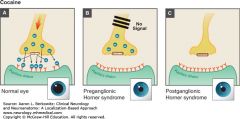
1. Cocaine blocks the reuptake of norepinephrine released at the neuromuscular junction of the iris dilator muscle, allowing for more local availability of norepinephrine. image 81 A sympathetically denervated eye will not respond to cocaine because there is no norepinephrine to begin with. The other pupil will become more dilated though, worsening the anisocoria. |
|
|
1. How are hydroxyamphetamine eye drops used to test for Horner's syndrome? |
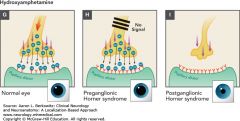
These drops can distinguish a lesion of the third-order neuron from lesions of the first- or second-order neurons. Hydroxyamphetamine causes release of stored norepinephrine in the third-order neuron. If, after installation of the hydroxyamphetamine the pupil dilates, it is a lesion of the 1st or 2nd order neurons. If it does not dilate, it is a lesion of the third order neuron. image 82 |
|
|
Adie's pupil 1. How does the pupil appear in the acute phase? 2. Where is the causative lesion? 3. What else does the patient sometimes complain of? |

1. Unilateral mydriasis with no constriction to light or accommodation due to paralysis of the iris sphincter and the ciliary muscle. 2. The lesion is in the postganglionic parasympathetic pathway to either the ciliary ganglion or the short ciliary nerves and is most often attributed to a viral etiology, though evidence is lacking. 3. Photophobia, visual blurring, and ache in the orbit. image83 |
|
|
Adie's pupil 1. How does the pupil respond to low-concentration pilocarpine (0.125%) in the subacute phase? 2. What happens in the chronic stage? 3. What is Holmes-Adie syndrome? |
1. Within a few days to weeks, denervation supersensitivity to cholinergic agonists develops. The tonic pupil will constrict but the normal pupil is unaffected by such a low concentration. 2. In the chronic stage, the pupillary light reflex rarely improves but the accommodation reflex improves though it often remains slower (tonic). This is termed light-near dissociation. 3. When Adie's pupil is associated with diminished or absent deep tendon reflexes. |
|
|
1. What are two other names for the primary visual cortex? 2. Where is the primary visual cortex? 3. What is the retinotopic representation on the visual cortex? |
1. The calcarine cortex and the striate cortex. 2. The medial surface and a small lateral surface of the occipital lobe, within the calcarine cortex. 3. The fovea is represented in the posterior part of the striate cortex, whereas the more peripheral regions of the retina are represented in progressively more anterior parts of the striate cortex. The upper visual field is mapped below the calcarine sulcus and the lower visual field above it. |
|
|
Optic Radiations 1. Where do the superior fibers travel and what information do they contain? 2. Where do the inferior fibers travel and what information do they contain? 3. Why might you get macular sparing with a homonymous hemianopsia? |
1. They travel through the parietal lobe and carry information from the inferior visual field. 2. They pass through the temporal lobe and carry information from the superior visual fields. 3. The macula may be spared in a PCA stroke because of collateral blood from the MCA. |
|
|
Nystagmus How do these qualities differ between central and peripheral nystagmus? 1. Fatigability 2. Latency 3. Suppression with visual fixation 4. Duration 5. Direction |
1. Fatigability Central is nonfatiguing, Peripheral is fatigable with repetition. 2. Latency Central has no latency, peripheral has latency typically of 2 to 20 seconds. 3. Visual fixation Central is not suppressed by visual fixation, peripheral is suppressed by visual fixation. 4. Duration Greater than 1 minute in central nystagmus, less than 1 minute in peripheral. 5. Direction Central may occur in any direction. Peripheral is usually unidirectional and usually horizontal, though can have a torsional component. |
|
|
1. In a unilateral peripheral vestibular lesion, which side do the eyes drift towards? 2. Does the nystagmus amplitude increase when looking towards the affected or unaffected ear? |
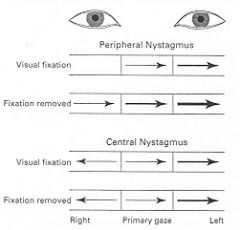
1. They drift towards the affected side (which is "pushing" less. 2. It increases when looking towards the unaffected ear. image 86 (arrows point towards the fast phase, arrow thickness represents the intensity of the nystagmus). |
|
|
What are the functional components of the 10th (Vagus) cranial nerve? |
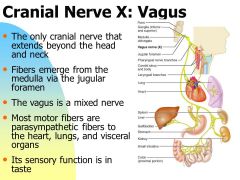
1. Branchial Motor (special visceral efferent): To the striated muscles of the pharynx, tongue (palatoglossus), and larynx (except the stylopharyngeus (CN 9) and the tensor veli palati (CN V3). 2. Visceral Motor (general viscerent efferent): To smooth muscle and glands of the pharynx, larynx, and thoracic and abdominal viscera. 3. Visceral sensory (visceral afferent): From the larynx, trachea, esophagus, and thoracic and abdominal viscera, stretch receptors in the walls of the aortic arch, chemoreceptors in the aortic bodies adjacent to the arch. 4. General sensory (general somatic efferent): From the skin at the back of the ear and in the external acoustic meatus, part of the external surface of the tympanic membrane, and the pharynx. image 87 |
|
|
1. What nucleus is involved in both taste and the baroreceptor reflexes? 2. What nucleus is responsible for innervation of the muscles of the larynx and pharynx? |
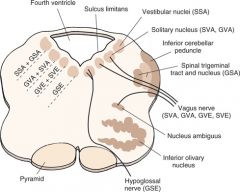
1. The nucleus tractus solitarius (also referred to as the solitary nucleus). 2. Nucleus ambiguus. image 88 |
|
|
1. Where does the ophthalmic division (V1) of the trigeminal nerve exit the cranium? 2. Where does the maxillary division (V2) exit the cranium? 3. Where does the mandibular division (V3) exit the cranium? |
1. Superior orbital fissure 2. Foramen rotundum 3. Foramen ovale |
|
|
1. What are the components of the ABCD2 score? 2. What is the 2 day risk of stroke for a score of 0-1, 2-3, 4-5, and 6-7? |
1. Age > 60 = 1 point Blood pressure > 140/90 = 1 point Clinical Symptoms: 1 point for speech impairment without weakness, 2 points for weakness. Duration of symptoms: 1 point for 10-59 minutes, 2 points for 60 minutes or more. Diabetes: 1 point 2. 0-1: 0% 2-3: 1.3% 4-5: 4.1% 6-7: 8.1% |
|
|
1. What are the afferent and efferent branches of the anal reflex arc (anal wink)? 2. What is the anal wink an indication of? 3. Name 4 symptoms associated with cauda equina syndrome. |

1. Afferent: pudendal nerve (S2-S4) Efferent: S2-S4. 2. The integrity of the sacral spinal cord segments and the sacral roots. 3. Saddle anesthesia, loss of reflexes (especially ankle jerk), leg weakness (LMN type), Bowel/bladder dysfunction. image 91 |
|
|
Polymyositis 1. What is the weakness pattern?
2. How does the CK do?
3. Name 3 other involved organs.
4. What does the EMG show? |

1. Symmetrical proximal weakness, including neck muscles.
2. Elevated (also they have myalgias)
3. Oropharyngeal/esophageal involvement with dysphagia, cardiac involvement, respiratory involvement.
4. Positive sharp waves, fibrillation potentials, rapid recruitment of short-duration polyphasic motor unit potentials.
image 92 |
|
|
Polymyositis 1. Where is the cellular infiltrate primarily? 2. Is there vasculopathy or immune complex deposition? 3. What is the main inflammatory cell type? |
1. The cellular infiltrate is predominantly within the fascicle with inflammatory cells invading individual muscle fibers. 2. No, this is in contrast to dermatomyositis. 3. Myofiber injury appears to be mediated directly by CD8+ cytotoxic T lymphocytes that surround and invade myofibers. image 94 |
|
|
Cranial Nerve Foramen 1. Olfactory Nerve 2. Optic Nerve 3. Oculomotor Nerve 4. Trochlear Nerve |
1. Olfactory Nerve: cribiform plate of the ethmoid bone. 2. Optic Nerve: Optic canal of the sphenoid. 3. Oculomotor Nerve: Superior orbital fissure 4. Trochlear Nerve: Superior orbital fissure image 93 |
|
|
Cranial Nerve Foramen 1. V1 2. V2 3. V3 4. Abducens Nerve |
1. V1: Superior orbital fissure 2. V2: Foramen rotundum 3. V3: Foramen ovale (with lesser petrosal from CN 9/glossopharyngeal) 4. Superior orbital fissure |
|
|
Cranial Nerve Foramen 1. Facial Nerve 2. Vestibulocochlear nerve 3. Glossopharyngeal |
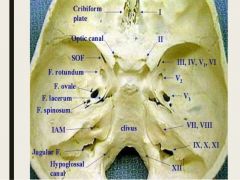
1. Internal acoustic meatus 2. Internal acoustic meatus 3. Jugular foramen |
|
|
Cranial Nerve Foramen 1. Vagus Nerve 2. Spinal accessory nerve 3. Hypoglossal |
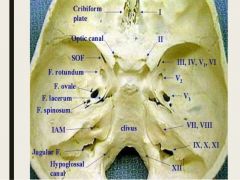
1. Juglar foramen 2. Jugular foramen (enters through the foramen magnum) 3. Hypoglossal canal |
|
|
What are the distinguishing factors histopathologically between dermatomyositis and polymyositis? |
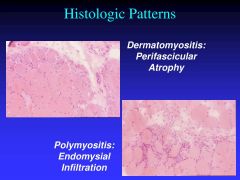
1. Dermatomyositis: Abnormal muscle fibers are usually grouped in one portion of the fascicle, suggestive of microinfarction mediated by blood vessel dysfunction vs. Polymyositis: In contrast to DM, abnormal necrotic and regenerating muscle fibers are scattered throughout the fascicle and are not limited to one portion. Muscle fiber size is variable. There are no signs of vasculopathy or immune complex deposition. Unlike DM, there is no perifascicular atrophy. image 96 |
|
|
1. What is a fascicle? 2. What is the perimysium? 3. What is the endomysium? |
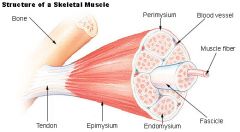
1. A fascicle is a bundle of skeletal muscle fibers surrounded by perimysium. 2. A sheath of connective tissue that groups muscle fibers into bundles. 3. A wispy layer of areolar connective tissue that ensheaths each individual myocyte. image 95 |
|
|
1. What is a cavernous malformation?
2. What do they look like on MRI?
3. What symptoms do they produce?
|
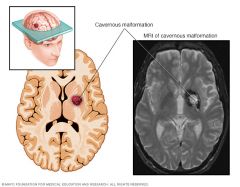
1. A cavernous malformation is a cluster of vascular channels, composed of dilated thin-walled vessels with no smooth muscle or elastic fibers, and with no intervening brain parenchyma separating the vascular structures.
2. They have a typical "popcorn-like" appearance with a dark rim on T2 consistent with hemosiderin. They might be more obvious on gradient echo images.
3. They are typically incidental, but may present with seizures or hemorrhage depending on the location of the lesion.
image 97 |
|
|
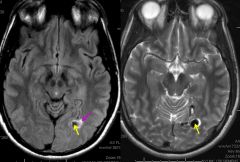
1. What is a dural arteriovenous fistula?
2. How do they affect fluid flow?
3. How might they present? |

1. A dural AVF is an acquired vascular lesion in which there is AV shunting from meningeal or dural arterial branches, with drainage towards a dural venous sinus.
2. They are associated with increased venous pressure and arterialization of the draining veins.
3. Tinnitus, headaches, seizures, and focal neurologic deficits from increased venous pressure and abnormal vascular hemodynamics. Intracranial hemorrhage can also occur.
Sometimes there are accompanying aneurysms (yellow arrow) and edema (pink arrow)
image 99 |
|
|
1. What is a dural arteriovenous fistula?
2. How do they affect fluid flow?
3. How might they present? |
1. A dural AVF is an acquired vascular lesion in which there is AV shunting from meningeal or dural arterial branches, with drainage towards a dural venous sinus.
2. They are associated with increased venous pressure and aterialization of the draining veins.
3. Tinnitus, headaches, seizures, and focal neurologic deficits from increased venous pressure and abnormal vascular hemodynamics. Intracranial hemorrhage can also occur.
Sometimes there are accompanying aneurysms (yellow arrow) and edema (pink arrow)
image 99 |
|
|
1. What is a venous angioma? 2. How does a venous angioma look on MRI? 3. What is a capillary telangiectasia? |
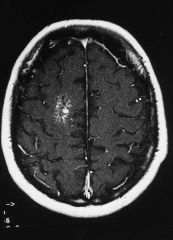
1. Venous angiomas or devlopmental venous anomalies are thin-walled venous structures with normal intervening brain tissue. They are asymptomatic with a very low risk of hemorrhage. 2. It has a caput medusa pattern. 3. Capillary telangiectasias are abnormally dilated capillaries that are separated by normal brain tissue. They rarely become symptomatic. |
|
|
1. What is the mnemonic for blood changes on an MRI over time? 2. What does it stand for? |
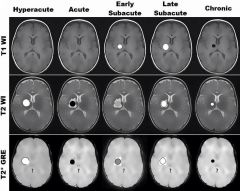
1. I Bleed, I Die, Bleed Die, Bleed Bleed, Die Die 2. I Bleed (hyperacute, <24 hours): T1 isointense T2 bright I Die (acute 1-3 days): T1 isointense T2 dark Bleed Die (early subacute 2-7 days): T1 bright T2 dark Bleed Bleed (late subacute 7 to 14-28 days): T1 bright T2 bright Die Die (chronic >14-28 days): T1 dark T2 dark image 101 |
|
|
1. Where do the anterior spinal arteries arise? 2. What does it supply? |
1. From the vertebral arteries (two branches come together to form the anterior spinal artery). The anterior spinal artery arises distal to the PICA and before the basilar. 2. It supplies the anterior two thirds of the spinal cord and the medial medulla. http://oxfordmedicine.com/mobile/view/10.1093/med/9780190214883.001.0001/med-9780190214883-chapter-1 |
|
|
1. Where do the posterior spinal arteries arise? 2. What do they supply? |
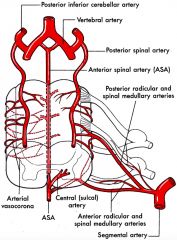
1. They arise from either the vertebral arteries or the posterior inferior cerebellar arteries. 2. It supplies the dorsal column of the medulla. At the spinal cord level it supplies the posterior third of the spinal cord (the dorsal and lateral column as well as the peripheral part of the anterior and central columns. image 103 |
|
|
1. What is the purpose of the segmental (radicular) arteries? 2. Name five vessels that they arise from. 3. Where do these feeder vessels arise? 4. What is their pathway? |
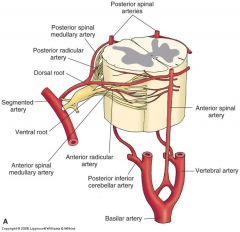
1. The spinal arteries are small caliber and often appear discontinuous. Thus, they require reinforcement from the segmental arteries. 2. Ascending cervical arteries Deep cervical arteries Posterior intercostal arteries Lumbar arteries Lateral sacral arteries 3. Most of them arise from the aorta. 4. They pass through the intervertebral foramen and divide into the anterior and posterior radicular arteries and have variable anastamoses with the spinal arteries. |
|
|
1. What is the dominant segmental artery? 2. Where does it arise from? |
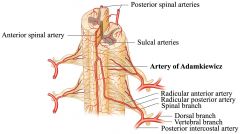
1. The artery of Adamkiewicz. 2. The artery of Adamkiewicz usually arises from a left posterior intercostal artery at the level of the 9th to 12th intercostal artery. The intercostal arteries branch from the aorta. It supplies the lower two thirds of the spinal cord via the anterior spinal artery. image 105 |
|
|
1. What are the three criteria for a diagnosis of brain death?
2. What other three features are required for a diagnosis of brain death? |
1. A catastrophic CNS condition leading to irreversible damage, examination findings of absent brainstem reflexes, and the presence of apnea on the apnea test.
2. 1: Absence of intoxication, neuromuscular blockade, pharmacologic sedation, or a medical condition that may obscure the clinical picture. 2: A normal or near normal core body temperature (>36 degrees Celsius) 3: Systolic blood pressure of more than 90 mm Hg or mean arterial pressure >60 mm Hg.
|
|
|
1. Ramsay Hunt syndrome occurs why?
2. What is the classic Ramsay Hunt triad?
3. Name 4 other frequently reported symptoms.
4. What other cranial nerves can be affected? |
1. When there is reactivation of latent VZV residing within the geniculate ganglion with subsequent spread of the inflammatory process to involve the 7th cranial nerve.
2. Ipsilateral facial paralysis, ear pain, and vesicles in the auditory canal/auricle.
3. Taste perception, hearing (tinnitus/hyperacusis), and lacrimation can be affected. Vertigo is also common.
4. V, IX, and X.
image 107
|
|
|
Name 4 ancillary tests that can be done to confirm death by neurologic criteria. |
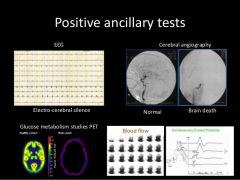
1. EEG showing electrocerebral silence in a recording of at least 30 minutes. 2. Transcranial doppler showing no flow signals, or abnormal signals including oscillating flow or short and low amplitude spikes in systole without diastolic flow. 3. Nuclear medicine scan showing no isotope uptake in the brain parenchyma or no intracranial flow. 4. Angiography demonstrating no flow in the circle of Willis. image 106 |
|
|
1. Ramsay Hunt syndrome occurs why? 2. What is the classic Ramsay Hunt triad? 3. Name 4 other frequently reported symptoms. 4. What other cranial nerves can be affected? |
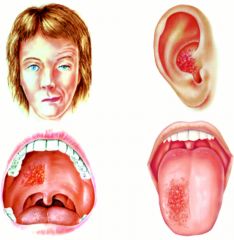
1. When there is reactivation of latent VZV residing within the geniculate ganglion with subsequent spread of the inflammatory process to involve the 8th cranial nerve. 2. Ipsilateral facial paralysis, ear pain, and vesicles in the auditory canal/auricle. 3. Taste perception, hearing (tinnitus/hyperacusis), and lacrimation can be affected. Vertigo is also common. 4. V, IX, and X. image 107 |
|
|
1. How does Ramsay Hunt syndrome compare to Bell's Palsy from HSV? 2. What treatment is there for Ramsay Hunt syndrome? |
1. More severe with increased rates of late neural denervation and a decreased probability of complete recovery. 2. Antiviral therapy is usually prescribed but there is limited data supporting it. |
|
|
What are the functional components of hypoglossal nerve (Cranial Nerve 12)? |
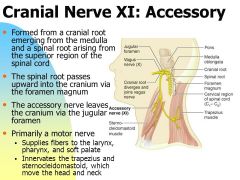
1. General somatic efferent: Supplies all of the intrinsic and extrinsic muscles of the tongue except for the the palatoglossus.
image 111 |
|
|
1. What are the clinical features of Tolosa Hunt Syndrome? 2. What causes Tolosa Hunt Syndrome? 3. What is the treatment? |
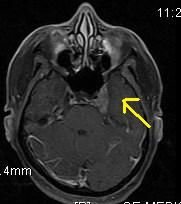
1. A constant pain behind the eye followed by paralysis of one or more of the extra-ocular muscles. It is usually unilateral. 2. Idiopathic granulomatous inflammation of the cavernous sinus. 3. It is generally treated with steroids (e.g. prednisone 100 mg daily for three days). Left untreated, it may resolve on its own after about 8 weeks. |
|
|
Bacterial Meningitis 1. What are the most common pathogens in the following age groups: Neonates Children (1 month or older) Very old / young 2. What about in adults in order of frequency? |
1. Infants: group B streptococcus, Escherichia coli, Listeria monocytogenes Children: Streptococcus pneumoniae and Neisseria meningitidis. Very Young / very Old: Listeria montocytogenes 2. S. pneumoniae and N. meningitidis, followed by Listeria monocytogenes, staphylococci, gram negative bacilli (including e coli, Klebsiella, Enterobacter, Pseudomonas aeruginosa), and Haemophilus influenzae (the incidence of the latter is <3% since the advent of the H. influenzae vaccine). |
|
|
What empiric antibiotics should be started for suspected adult bacterial meningitis? |
1. Third generation cephalosporin (such as ceftriaxone 2 g IV q12H) or fourth generation cephalosporin (cefepime 2 g IV q8H). To this, add vancomycin (15-20 mg/kg IV not to exceed 2 g per dose or 60 mg/kg per day - adjust dose to achieve vancomycin serum trough concentrations of 15-20 mcg/mL. If suspicion for listeria (age <1 month or >50 years), add ampicillin 2 grams every four hours. |
|
|
Abductor Pollicis Brevis Name the: Nerve: Roots: Trunk: Cord: Action: Test: |
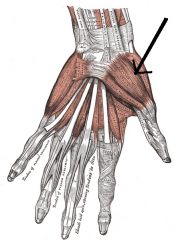
Abductor Pollicis Brevis Nerve: Median Roots: C8-T1 Trunk: Lower Trunk Cord: Medial Cord Action: Thumb abduction Test: Have the patient abduct the thumb at right angles to the palm. This action is accomplished by having the patient place the palm flat, facing upwards, and pointing the thumb at the ceiling.
image 113 |
|
|
1. At what forced vital capcity level should patients with MG or GBS receive ICU level monitoring? 2. At what FVC level is intubation typically necessary? 3. At what NIF is ICU level monitoring recommended? |
1. 20 cc's / kg 2. 10-15 cc's / kg 3. When the NIF is less negative than -20 |
|
|
Opponens Pollicis Name the: Nerve: Roots: Trunk: Cord: Action: Test: |
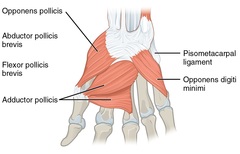
Nerve: Median Roots: C8-T1 Trunk: Lower Cord: Medial Action: Thumb Opposition Test: Have the patient touch the thumb to the base of the little finger image 114 |
|
|
1. Is the direct pathway excitatory or inhibitory? Why?
2. Do reductions in direct pathway activity lead to hyperkinetic or hypokinetic movement disorders? |
1. The direct pathway is excitatory because it inhibits the globus pallidus interna. The globus pallidus interna normally inhibits the thalamus, so thalamacortical activity gets increased by the direct pathway.
2. Hypokinetic movement disorders. Thalamic projections to the cortex are excitatory, so if there is less activation of the thalamus, hypokineses can result. LOOK FOR IMAGE |