Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
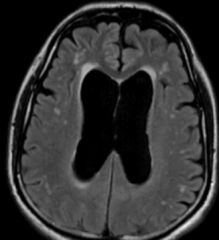
What is shown? What can this cause?
|
Hydrocephalus
|
|
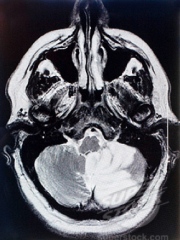
What is shown? What kind of dementia may this cause?
|
Huge cerebellar infarct. May cause vascular dementia.
|
|

What is shown?
|
Metastatic breast cancer
|
|
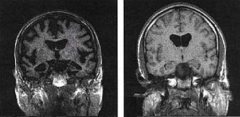
What is shown on the left?
|
Alzheimers. Massive brain atrophy.
|
|
What is shown? What symptoms could this cause? What is the most likely cause of this injury?
|
Subdural hematoma. Can cause focal neuro symptoms. Most likely the result of tearing of bridging veins.
|
|
|
Long acting ACh-esterase inhibitor, muscarinic modulator, nicotinic agonist, may also be a MAOI, ↓ GABA release, ↑ release of NE, DA, 5-HT. Used in the tx of Alzheimers.
|
Tacrine
|
|
|
What ACh-esterase inhibitor has poor bioavailability (extensive 1st pass metabolism) & many adverse effects including hepatotoxicity? Used in the tx of Alzheimers.
|
Tacrine
|
|
|
This drug reduces deterioration in cognitive performance in the 1st 3 mos of Tx but shows no evidence it delays the long-term course of AD.
|
Tacrine
|
|
|
ACh-esterase inhibitors approved for both mild to severe symptomatic management of Alzheimers.
Does not alter long term prognosis, but improves global fxn, cognition & behavior. Delays tims to institutionalization |
Donepezil
|
|
|
What ACh-esterase inhibitor has 100% bioavailability, higher CNS affinity (fewer side effects) and is metabolized by cytochrome P450? Used in the tx of Alzheimers.
|
Donepezil
|
|
|
While metabolized by cytochrome p450 this ACh-esterase inhibitor is NOT hepatoxic. Used in the tx of Alzheimers.
|
Donepezil
|
|
|
This ACh-esterase inhibitor is a natural alkaloid dervied from daffodils and is approved for mild to moderate AD.
|
Galantamine
|
|
|
What ACh-esterase inhibitor may also be beneficial in Tx symptoms of vascular dementia & dementia w/ Lewy bodies?
|
Galantamine
|
|
|
What ACh-esterase inhibitor requires multiple daily dosages (a slow titration) to limit GI side-effx? It also has partial metabolism via CYP450 & renal excretion. Used in the tx of Alzheimers.
|
Galantamine
|
|
|
What ACh-esterase inhibitor is approved or both mild to moderate AD and Parkinson's disease?
|
Rivastigmine
|
|
|
What ACh-esterase inhibitor is NOT metabolized by CytP450 and therefore has fewer drug interactions? How is it metabolized? Used in the tx of Alzheimers.
|
Rivastigmine
Metabolized by cholinesterase at CNS sites |
|
|
What are the side efx associated w/ Rivastigmine? (Used in the tx of Alzheimers.)
|
GI. Available as a patch with fewer side effx.
|
|
|
What ACh-esterase inhibitor is in Phase III trials for Lewy Body dementia, vascular dementia, & mild cognitive impairment?
|
Rivastigmine
|
|
|
What class ofAlzheimer's drugs are used for mild to moderate AD, severe AD by delay/preventing symptoms from becoming worse? They may help control some behavioral symptoms, ↑effects of reamining NT afferents, and may reduce A-beta 1-42 by stimulating Ig production?
What are the drugs in this class? |
Acetylcholinesterase inhibitos
Tacrine, Donepezil, Galatamine, Rivastigmine |
|
|
What drug used in the tx of Alzheimers is an NMDA-receptor antagonist?
|
Memantine
|
|
|
What NMDA-receptor antagonist is approved to modertae-severe AD (pending for mild AD)?
|
Memantine
|
|
|
What are the benefits of Memantine? What is its MOA?
|
• Improved cognitive & psychomotor fxn
• Reduction of care dependence • Neuroprotective, slows disease progression • Very few side effx • Not metabolized by Cyt P450 • Extended release formulation is available |
|
|
What drug used in the tx of Alzheimer's disease has very good tolerability (side effx similar to placebo) and few drug interaxns? Why is this?
|
Memantine
• Not metabolized by CytP450 |
|
|
What neurological disease presents with memory loss as the first symptom w/ a MMSE showing epsodic memory loss?
|
Alzheimer's disease
|
|
|
What neurological disease will show entorhinal cortex & hippocampal atrophy in imaging?
|
Alzheimer's disease
|
|
|
What will the MMSE, neuropsych & neuro exam show in Alzheimer's disease?
|
MMSE will show episodic memory loss, but neuropsych & neurology exam will initially be normal
|
|
|
What neurological disease first presents with apathy, poor judgment/insight/speech/language & hyperorality?
|
Fronto-temporal dementia
|
|
|
What will the MMSE and Neuropsych exam show for Fronto-temporal dementia?
|
MMSE: shows deficits in frontal/executive fxn & language but spares drawing
Neuropsych exam show apath, disinhibition, hyperorality, euphoria, depression |
|
|
What neurological disease may show vertical gaze palsy, axial rigidity, dystonia, alien hand, or motor neuron disease in the neurology exam?
|
Fronto-temporal dementia
|
|
|
What neurological disease will show frontal, insular and/or temporal atrophy w/ sparing of the posterior parietal lobe in imaging?
|
Fronto-temporal dementia
|
|
|
What neurological disease will first present w/ visual hallucinations, REM sleep disorder, delirium, Capgras' synrome, or Parkinsonism?
|
Lewy-body dementia
|
|
|
What will the MMSE and Neuropsych exam show for Lewy-body dementia?
|
• MMSE will show deficits in drawing & frontal/executive fxn. May show delirium. Memory is spared.
• Neuropsych exam will show visual hallucinations, depression, sleep disorders, and delusions |
|
|
What neurological disease may show Parkinsonism in the neurology exam?
|
Lewy-body dementia (or Creutzfeld-Jakob)
|
|
|
What neurological disease will show posterior parietal atrophy (and hippocampi larger than in AD) in imaging?
|
Lewy-body dementia
|
|
|
What neurological disease will present with dementia, mood ∆s, anxiety, & movement disorders?
|
Creutzfeld-Jakob disease
|
|
|
What will the MMSE and Neuropsych exam show for Creutzfeld-Jakob disease?
|
• MMSE will show deficits in variable frontal/executive fxn, focal cortical, & memory
• Neuropsych will show depression & anxiety |
|
|
What neurological disease may show myoclonus, rigidity, & parkinsonism in the neurology exam?
|
Creutzfeld-Jakob disease
|
|
|
What neurological disease will show non-covulsive seizure activity and/or periodic discharges on the EEG?
|
Creutzfeld-Jakob disease
|
|
|
What neurological disease will show cortical ribboning & basal ganglia/thalamus hyperintensity on diffusion/flair MRI?
|
Creutzfeld-Jakob disease
|
|
|
What neurological disease will often first present with sudden, variable; apathy, falls, & focal weakness with stepwise deterioration?
|
Vascular dementia
|
|
|
What will the MMSE and Neuropsych exam show for Vascular dementia?
|
• MMSE will show deficits in frontal/executive fxn, cognitive slowing (sparing of memory)
• Neuropsych exam will show apathy, delusions, & anxiety |
|
|
What neurological disease will show motor slowing or spasticity but can also be normal?
|
Vascular dementia
|
|
|
What neurological disease will show cortical and/or subcortical infarctions, confluent white matter disease in imaging?
|
Vascular dementia
|
|
|
What class of dementias will show stepwise, sudden deterioration in cognition; episodes of confusion, aphasia, slurred speech, & focal weakness?
|
Cerebrovascular disease: Vascular dementia, multi-infarc dementia, Binswangers dementia
|
|
|
To w/u for dementia in all patients you must do a:
• Brain MRI (including FLAIR & DWI, w/ & w/o gad), • Serum electrolytes • Liver, renals & Thyroid fxn tests • Vitamin B12 & homocysteine and what other test? |
Urinalysis, culture
|
|
|
Definition: Reduced comprehension, coherence, ability to reason. Commonly encountered in clinical setting.
|
Altered Mental Status
|
|
|
Definition: Relatively acute decline in cognition (especially attention but all cognitive domains may be affected)
|
Delirium
|
|
|
Definition: Progressive decline in cognitive function (especially memory, but all domains may be affected)
|
Dementia
|
|
|
Definition: Cognitive deficits that interfere subtly with ADLs, possible precursor to dementia
|
Mild Cognitive impairment
|
|
|
What are the 4 DSM IV criteria for dementia?
|
1. Memory impairment
2. At least one of: Aphasia, Apraxia, Agnosia, Disturbance in executive fxning 3. The disturbance in 1 or 2. significantly intereferes w/ work, social activities, or relationships 4. Disturbance does not occur exclusively during delirium |
|
|
Definition: difficulty carrying out purposeful motor fxn b/c of planning, coordinating or executing action, not because of movement, senses or comprehension of command
|
Apraxia
|
|
|
Definition: Imparied ability to recognize of identify objects, even though sensory abilities are intact
|
Agnosia
|
|
|
What neurological disease will often first present with prominent deficits in executive fxn w/ memory initially intact?
|
Vascular dementia
|
|
|
In what dementia do behavioral symptoms predominate? What is another common presentation?
|
• Frontotemporal dementia
• May also present w/ aphasias (fluent & nonfluent) |
|
|
What clinical test/exam is most SPECIFIC for dementia? What clinical test/exam is most SENSITIVE for dementia?
|
• Specific: Short Portable Mental Status Questionnaire: 94% (followed by MMSE & clinical judgement, 82%)
• Sensitive: NINCDS criteria 92% |
|
|
What dementia progresses episodically? Which progresses rapidly?
|
• Alzheimers (episodically)
• Rapidly with Creutzfeld-Jakob disease |
|
|
What dementia may present w/ loss of position/vibratory sense?
|
B-12 deficiency
|
|
What is pictured? What are they caused by? What diseases can these be seen in ?
|
Lewy body inclusions, caused by α-synnuclein protein deposits in neuronal nuclei
• Seen in Parkinson's (substantia nigra) and Lewy Body Dementia (cortex) |
|

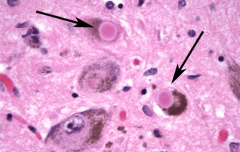
What is pictured on the L? on the R? What proteins are they derived from? Characteristic of what disease?
|
L: Neurofibrillary tangle (from abnormal tau protein - used to assemble microtubules)
R: Senile plaque of β-amyloid • Alzheimer's disease |
|
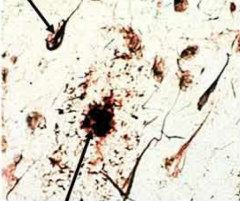
What is seen on the top? On the bottom? What proteins are involved? What disease are these characteristic of?
|
TOP: Neurofibrillary tangle (from abnormal tau protein - used to assemble microtubules)
BOTTOM: Senile plaque of β-amyloid • Alzheimer's disease |