![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
235 Cards in this Set
- Front
- Back
|
What are the general features of large/ elastic arteries? |
Internal elastic lamina (between intima and media) External elastic lamina (between media and adventitia) Very thick tunica media, layers of elastic fibres alternating with smooth muscle - SM allows constriction/ dilation, provides structural integrity |
|
|
Muscular arteries are distributing arteries that transition between large and small arteries. What are the general features of muscular arteries? |
Smaller diameter, fewer elastic fibres than elastic arteries More SM - allows vasoconstriction and vasodilation - haemostasis Internal and external elastic lamina present |
|
|
Small arteries/ arterioles are key point of control for blood flow through SM. What are the general features of small arteries? |
Up to 8 layers of SM in media Internal elastic lamina |
|
|
Small arteries/ arterioles are key point of control for blood flow through SM. What are the general features of arterioles? |
1-2 (5 max) layers of SM in media Adventitia sparse, poorly developed - linked by connective tissue |
|
|
What is the general structure of veins? |
Acompany artiers, much thinner wall Thinner media, some have valves to prevent backflow |
|
|
What are the general features of venules? |
Endothelium and basal lamina Pericytes (contractile) Sensitive to H2 and 5-HT, increased permeability to fluid and WBCs during allergic and inflammatory reactions No real media, just 1-2 SM layers |
|
|
What are the general features of capillaries? |
Endothelium and basal lamina Needs gaps for diffusion - fenestrae |
|
|
What is a continuous capillary and where are they found? |
No fenestrae or gaps Found in CNS, PNS, muscle |
|
|
What is a fenestrated capillary and where are they found? |
Thin endothelium Fenestrations of 80-100nm Found in small intestine, kidney, glands |
|
|
What is a sinusoidal capillary and where are they found? |
Have fenestrae and large gaps Specialised - thin walled, large diameter |
|
|
What is blood flow (Q) through each circulation equal to? |
Q=(D)P/R Pressure gradient (delta-P) - difference in pressure between aorta and vena cava R - resistance of vessels Blood flow also proportional to 1/R |
|
|
How is Resistance (R) calculated? |
R = 8Ln/ πr^4 (n - eta - viscosity of blood) |
|
|
What is the most important physiological factor affecting resistance and why? |
Radius - length and blood viscosity generally constant |
|
|
What is the effect of vessel radius on blood flow? |
The narrower the vessel, the faster the velocity of flow |
|
|
What is the main resistance to flow in the systemic circulation? |
Arterioles - pressure drop across them larger than any other vessel class Control TPR to match blood flow to local need |
|
|
What factors modulate vascular tone and how can they be overridden? |
Local: - Myogenic response - vasoconstriction - Metabolites - vasodilation External: - Nerves - ANS - Hormones - circulating and local NO Metabolites can override myogenic e.g. working skeletal muscle |
|
|
What is the myogenic response? |
Intrinsic activity of SM, safety mechanism to prevent damage to delicate blood vessels Flow constant with increasing pressure, done through stretching |
|
|
What are the metabolism-derived vasodilators? |
CO2 H+ (decreased pH) = lactate K+ Osmolality Temperature Decreased oxygen All have effect during exercise, increases blood flow to working muscle |
|
|
What are the three types of autonomic vasomotor nerves? |
Sympathetic fibres (most important and most widespread) Sympathetic vasodilator fibres Parasympathetic vasodilator fibres |
|
|
What is the effect of sympathetic fibres on blood vessels? |
Noradrenaline binding to α1-adrenergic receptors on SM causes vasoconstriction via increase in Ca2+ |
|
|
How does the effect of sympathetic fibres change for blood vessels in the heart? |
These vessels have little if any SNS innervation. Here circulating adrenaline binds to β2-adrenergic receptors on SM to cause vasodilation |
|
|
What is the effect of sympathetic vasodilator fibres on blood vessels?
|
Sympathetic cholinergic (use ACh) Found in arterioles of skeletal muscle (alerting response), external genitalia, sweat glands |
|
|
What is the effect of parasympathetic vasodilator fibres? |
Parasympathetic cholinergic Lead to NO production e.g. found in salivary glands |
|
|
Why are capillaries ideal for efficient exchange of metabolites and gasses? |
Narrow, short, thin with large SA for exchange Low blood velocity due to large CSA This gives 1-2 secs for RBCs in vessel |
|
|
Why is resistance to flow in capillaries very low even though the radius is small? |
Short length, vessels arranged in parallel |
|
|
What is the main role of veins and venules? |
Act as blood reservoir - hold up to 70% of blood at rest High capacitance vessels - easily stretch without great increase in pressure (high compliance) |
|
|
How can veins constrict and what is the purpose of this? |
Due to ANS - sympathetic supply, α-adrenergic receptors Pushes blood back to heart (venous return) aided by one way valves (important in posture, exercise, haemorrhage |
|
|
What are the portions of the respiratory tract? |
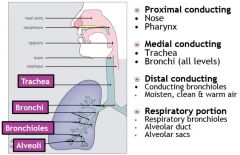
Image |
|
|
What is hyaline cartilage? |
C-shape in trachea |
|
|
How does epithelium change on decending the bronchial tree? |
Columnar --> cuboidal Fewer goblet cells |
|
|
How does cartilage change on descending the bronchial tree? |
Reduced Bronchioles have not cartilage - high in elastin and SM instead |
|
|
What joins the 'C' of the trachea? |
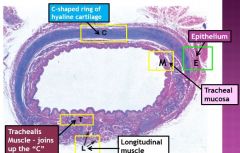
Trachealis muscle (in front of longitudinal) |
|
|
What type of epithelia is present in the trachea? |
Ciliated pseudostratified columnar - Mucous transport (goblet cells), filtering, moistening |
|
|
What warms the air entering the trachea? |
Capillary plexus in conducting portion (lamina propria) |
|
|
What components make up the distal conducting portion of the bronchial tree? |
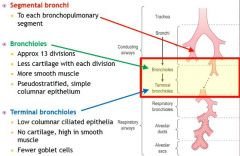
Image |
|
|
How do bronchioles differ from the trachea? |
No cartilage support No goblet cells Increase in ciliated cells |
|
|
What can be said about terminal bronchioles? |
Smallest diameter of conducting portion Divide into respiratory bronchioles No goblet cells/ cilia |
|
|
What components make up the respiratory portion of the bronchial tree? |
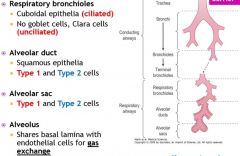
Image |
|
|
How many terminal bronchioles supply a respiratory lobule? |
One |
|
|
How many respiratory bronchioles supply an acinus? |
One |
|
|
What do terminal bronchioles subdivide into? |
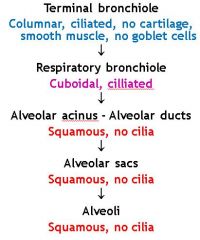
Image |
|
|
What is a pneumocyte? |
alveolar cell |
|
|
What is significant about the basal lamina underlying alveolar epithelium? |
Fuses into a single structure with surrounding capillaries - makes blood-air barrier extremely thin - No connective tissue in these regions |
|
|
What is contained in the interstitial space within the blood-air barrier? |
Capillaries Lymphocytes Mast cells Connective tissue - Fibroblasts - Elastic fibres - Collagen fibres |
|
|
What four phases comprise the respiratory cycle? |
Ventilation Gas exchange 1 Gas transport (Hb) Gas exchange 2 (to tissues) |
|
|
What is the pressure gradient during inspiration? |
Alveolar < atmospheric |
|
|
What is the pressure gradient during expiration? |
Alveolar > atmospheric |
|
|
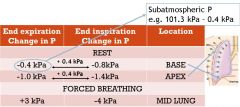
What is normal atmospheric pressure? |
101.3 kPa |
|
|
What is the pressure difference during quiet breathing? |
+/- 0.1 kPa |
|
|
What is the pressure difference during forced breathing? |
+/- 2.5 kPa |
|
|
How is the pressure difference across the airways generated? |
Increased volume of the thoracic cage and therefore the lungs - Ribs life upwards and outwards |
|
|
What are the accessory muscles used during respiration? |
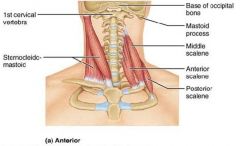
Scalene - elevate 1st and 2nd ribs Sternocleidomastoids - move sternum |
|
|
What muscles are used during quiet breathing? |
Diaphragm Parasternal Internal intercostals |
|
|
What muscles are used during vigorous breathing? |
Diaphragm Parasternal Internal intercostals External intercostals Accessory muscles |
|
|
What is the mechanism of forced expiration? |
Internal intercostals and abdomen contract, increasing intra-abdominal pressure Pushes diaphragm back up into the thorax |
|
|
What causes pneumothorax? |
Air between pleural layers breaks fluid linkage, lung collapses due to elastic recoil |
|
|
How much blood can the pleural layer hold? |
3L |
|
|
How is pneumothorax and haemothorax treated? |
Insert chest drain to remove air/ blood Re-expand the lung |
|
|
What must respiratory muscles work to overcome during inspiration? |
Elastic recoil of lungs, thorax (80%) Airways resistance (15%) Tissue resistance (5%) - Deformation of tissue in lung and thorax |
|
|
What is functional residual capacity (FRC)? |
Volume of air remaining in the lungs at the end of a normal resting respiration |
|
|
What is intrapleural pressure? |
Equal to intrathoracic pressure (not a constant value) |
|
|
What factors cause variation in intrapleural pressure? |
Stage in respiration (inspiration vs expiration) Position in lung (apex vs base) Pattern of breathing (forced vs rest) |
|
|
At rest, is intrapleural pressure higher at the base of the lung or the apex? |
Apex |
|
|
How can intrapleural pressure be measured? |
Directly by injecting a bubble between the pleural layer and measuring the pressure in the bubble with a manometer Indirectly through intra-oesophageal pressure |
|
|
What is compliance? |
The ease with which the lungs can be inflated |
|
|
How is compliance measured? |
V/P (change in lung volume / change in intrapleural pressure) |
|
|
What does a high/ low compliance indicate? |
High = easier to inflate *impossible to empty lungs |
|
|
What is specific compliance? |
Takes into account individual variability = Compliance/ lung volume (one lung) |
|
|
What are the values for compliance in a healthy person? |
2L / kPa compliance 0.8 L / kPa / L. lung volume specific compliance |
|
|
What disease could cause an abnormally high compliance? |
Emphysema - lungs are flabby, easier to expand |
|
|
What disease could cause an abnormally low compliance? |
Alveolar fibrosis - lungs are rigid, harder to expand |
|
|
What is responsible for elastic recoil in the lungs? |
Elastic fibres in the lungs - Elastin and collagen fibres in alveolar walls and around vessels and bronchi Surface tension - Liquid film lining the alveoli |
|
|
What is surface tension? |
The measure of the the force acting to pull/ hold a liquid's surface molecules together Attractive forces between adjacent molecules in liquid are much stronger than those between liquid and gas |
|
|
What is surfactant? |
Mixture of phospholipids (90%) and proteins secreted by type II alveolar cells |
|
|
What is the function of surfactant? |
To reduce surface tension forces in alveoli - Reduces work of breathing - Helps prevent fluid accumulating in alveoli - Helps keep alveoli uniformly ventilated |
|
|
What is surface tension of water and surfactant proportional to? |
Surface area |
|
|
What is laplace law? |
P = 2T/r Small R = very low surface tension Large R = low surface tension *Never high surface tension |
|
|
How is airways resistance distributed? |
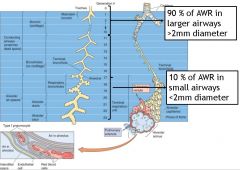
Image |
|
|
Which bronchial generation has the greatest airway resistance? |
3rd |
|
|
What factor does airway resistance change proportionally to? |
Inversely proportional to cross sectional area: High CSA = low resistance |
|
|
What can be said about airway resistance in asthma and COPD? |
Increased, making it harder to breathe Reversible in asthma, not in COPD |
|
|
How is airway resistance measured? |
= Driving pressure / gas flow |
|
|
What is driving pressure? |
The difference between mouth pressure (atomspheric) and the average pressure across all alveoli in the lung (FEV1.0, PEF) |
|
|
What is FEV1.0? |
Greatest volume of air expired in the first second starting from the position of maximal inspiration and expiring as hard and fast as possible |
|
|
What is PEF? |
Maximum flow rate during a forced expiration |
|
|
How is airway resistance related to lung volume? |
Resistance decreases as lung volume increases Airways distend as lungs inflate - wider airways have lower resistance |
|
|
What four factors affect AWR? |
Lung volume (mechanical tethering) Foreign body in airway SM contraction * Fluid in airway* - Increased secretions - Increased blood vessel permeability * - controlled by ANS |
|
|
How does PNS innervation affect bronchial tone? |
Release of acetylcholine stimulates muscarinic receptors Increases Ca2+ to cause bronchoconstriction |
|
|
How does SNS innervation affect bronchial tone? |
Little/ no SNS innervation Adrenaline, noradrenaline act on β2 adrenergic receptors Increase cAMP to cause bronchodilation |
|
|
How do peptinergic 'NANC' signals from the ANS affect bronchial tone? |
Substance P/ neurokinin - increase Ca2+, bronchoconstrict VIP/ VIP R - increase cAMP - bronchodilate |
|
|
What is the effect of histamine on the airways? |
Increases SM contraction Increases vascular permeability causing airway oedema Increases mucus secretion Produced locally in airways |
|
|
What stimulates histamine release in the airways? |
Physical stimuli (increased airflow) Cold air ATP released from damaged cells Antigen by cross-linking IgE on mast cell surface |
|
|
What is the effect of prostaglandins and thromboxanes on the airways? |
Contraction or relaxation of SM Produced locally in airways |
|
|
What is the effect of leukotrienes on the airways? |
Contraction or relaxation of SM (antagonists used as asthma treatment) Produced locally in airways |
|
|
What controls bronchial secretions? |
Mucus secreted by goblet cells PNS - increases by activating cholinergic path SNS - little effect. α1 inhibits, β2 stimulates |
|
|
How does increased mucus affect AWR? |
Decreases luminal diameter to increase resistance (like constriction) |
|
|
What is hypoxaemia? |
An acute imbalance between oxygen requirements, oxygen delivery and oxygen utilisation, often exaggerated by chronic illness |
|
|
Various pressures of the oxygen cascade (image) |
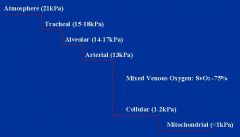
Image |
|
|
What are the different types of hypoxaemia? |
Hypoxic: V/Q mismatch Anaemic Stagnant (pump failure) Ischaemic (restricted flow) Cellular (failure of utilisation) |
|
|
What is COPD and what are the common symptoms? |
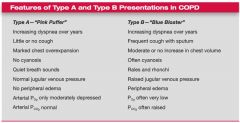
Chronic bronchitis + emphysema + airway obstruction Dyspnoea, cough with sputum production |
|
|
How is partial pressure calculated? |
% gas / atmospheric (101.3 kPa) e.g. oxygen = 21.3 kPa assuming dry air |
|
|
What would happen to 500mls air entering the alveoli? |
150mls trapped in anatomical dead space 350mls into alveolar air Alveolar compartment = ~2.5L |
|
|
What is expired gas comprised of? |
Gas from dead space and alveolar spaces |
|
|
What are the dimensions of the pulmonary blood-gas barrier? |
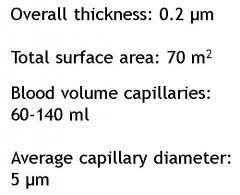
Image |
|
|
How does oxygen transfer across a capillary? |
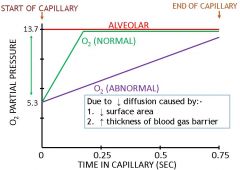
Graph |
|
|
How does carbon dioxide transfer across a capillary? |
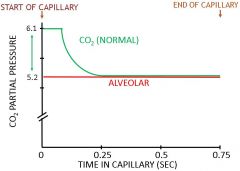
Graph |
|
|
What is diffusing capacity? |
Measure of the ability of the alveolar capillary membrane to conduct gases |
|
|
How is diffusing capacity (DL) estimated? |
Measure volume of gas diffusing from alveoli to pulmonary capillary per unit time Measure driving pressure (alveolar gas pressure - pressure of the gas in pulmonary capillary blood) |
|
|
Why is carbon monoxide used to calculate diffusing capacity? |
Driving pressure easy to calculate Reflects diffusion properties of blood gas barrier and not rate at which blood is flowing through pulmonary capilaries |
|
|
What is the normal value for DLCO? |
25 ml/min/mmHg |
|
|
What can cause a decrease in DLCO? |
Reduced SA for gas ex. (emphysema) Increased thickness of pathway (pulmonary fibrosis) V/Q mismatch |
|
|
What factors affect alveolar pressures? |
Rate of alveolar ventilation Rate of transfer of O2 and CO2 through respiratory membrane |
|
|
What are the main causes of hypoxaemia? |
Hypoventilation Shunt V/Q inequality |
|
|
What do PA and Pa correspond to? |
PA: Alveolar partial pressure Pa: Arterial partial pressure |
|
|
What is hypoventilation and what causes it? |
Reduced alveolar ventilation Increased AWR (asthma/ COPD) Drugs (morphine, barbituates) Paralysis of respiratory muscles |
|
|
What is a shunt (venous admixture) and what is a normal physiological example? |
Blood flow from venous side of circulation that does not pass a functional respiratory epithelium and then enters arterial side of circulation Normally occurring in bronchial circulation |
|
|
What is the effect of a venous admixture shunt? |
Poorly oxygenated blood depresses PaO2 of arterial blood Cannot be treated by 100% O2 as shunted blood bypasses ventilated alveoli, normal ones are saturated |
|
|
What is V/Q? |
Alveolar ventilation ______________________________ Cardiac output Normally = 4/5 = 0.8 |
|
|
How can alveolar ventilation be calculated? |
(Tidal volume - dead space) x resp. rate |
|
|
What will V/Q = if ventilation is obstructed and why? |
V/Q = 0 PAO2 falls, PACO2 rises Less O2 taken up in overperfused alveoli, less CO2 blown off Airway limitation (asthma, COPD) Lung collapse Loss of elastic tissue (emphysema) |
|
|
What will V/Q = if blood flow is obstructed and why? |
V/Q = infinite PAO2 rises, PACO2 falls No more O2 can be taken up as Hb saturated, extra CO2 blown off Pulmonary embolism Necrosis/ fibrosis of capillary bed |
|
|
V/Q mismatch diagram |
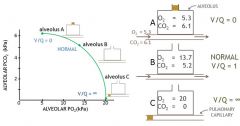
Image |
|
|
What is the effect of emphysema on V/Q? |
Destruction of alveoli leads to underventilation - lowers V/Q Loss of capillaries leads to underperfused alveoli - raises V/Q Overall gas exchange effectiveness reduced to 1/10th normal |
|
|
What mechanisms reduce V/Q differences between alveoli? |
Low alveolar pO2 causes constriction of pulmonary arteries, reduces perfusion to match Low alveolar pCO2 causes constriction of alveolar ducts, reduces ventilation to match Last out, first in principle |
|
|
How do arterial gas pressures vary in different areas of the lungs? |
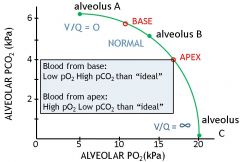
Image |
|
|
Oxygen response curve |
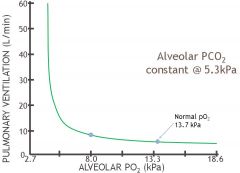
Image |
|
|
Carbon dioxide response curve |
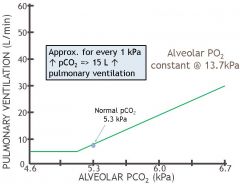
Image |
|
|
How does ventilation respond to [H+]? |
No stimulation of ventilation until arterial pH reduced by 0.1pH unit Fall in arterial pH of 0.4pH units required for 2-3 fold increase in ventilation |
|
|
Response to CO2 in presence of hypoxia |
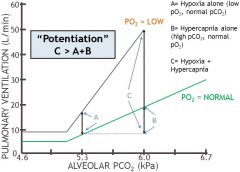
Image |
|
|
How do chemical stimuli affect ventilation? |
pO2 regulates ventilation but only at very low levels Approx every 1kPa change in pCO2 increases ventilation by 15L/ min [H+] needs big changes to influence Increase CO2 in presence of hypoxia: potentiation |
|
|
What are the peripheral chemoreceptors involved in ventilation? |
Carotid bodies Aortic bodies |
|
|
What are carotid bodies comprised of and what are their features? |
Glomus cells - Chemosensitive - Secrete neurotransmitters - Activate afferent nerve terminals from cranial nerve IX (glossopharyngeal) |
|
|
What do glomus cells respond to? |
Decreased PaO2: most sensitive Increased PaCO2: relatively weak Decreased pHa: relatively weak |
|
|
What is the clinical relevance of glomus cells? |
COPD - Decreased PaO2 (hypoxia) - Increased PaCO2 (hypercapnia) Compensation: - Choroid plexus increases amount of bicarbonate to buffer excess CO2 - Patient desensitised to CO2 so control of ventilation lies with peripheral chemoreceptors detecting hypoxia |
|
|
Where do the nerves that innervate the respiratory muscles originate from? |
Diaphragm: C3-5 External intercostals: T5-6 Internal intercostals (lateral): T11-12 |
|
|
Respiratory muscles output graph |
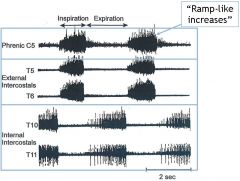
Image |
|
|
What are the brain's respiratory centres? |
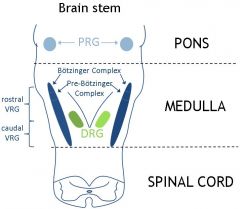
PRG - Pontine resp. group VRG - Ventral resp. group DRG - Dorsal resp. group |
|
|
What is the function of the Pontine respiratory group? |
Influence pattern of ventilation 'Phase switching' |
|
|
What is the function of the Ventral respiratory group (medulla)? |
Contains I (insp.) and E (exp.) neurons Amplitude (depth) Rhythm generation (pre-Botzinger complex) |
|
|
What is the function of the Dorsal respiratory group (medulla)? |
I neurons only Integrate sensory information(solitary tract) |
|
|
What are the 7 forms of respiratory neurogenic input? |
1) Cortical factors 2) Reflexes from lung receptors 3) Baroreceptor reflexes 4) Reflexes from muscles and joints 5) Reflexes from periphery 6) Protective reflexes 7) Co-ordination with other functions |
|
|
What are the 4 reflexes from lung receptors? |
Irritant receptors C-fibre receptors Hering-Breuer inflation (stretch) receptors J-receptor reflexes |
|
|
Hering-Breuer inflation reflex |

Image |
|
|
What is the J-receptor reflex? |
J receptor = juxtapulmonary capillary receptor Stimulated by pulmonary capillary hypertension and oedema in the alveolar walls |
|
|
What are the baroreceptor reflexes? |
Decreased ABP --> Increased ventilation |
|
|
What are the reflexes from the periphery? |
Pain and heat --> increase ventilation |
|
|
What are the protective reflexes? |
Laryngeal (protect lungs) Cough (protect lower airways) Sneeze (protect upper airways) |
|
|
What other functions do respiratory reflexes coordinate with? |
Speech (prolong expiration) Defaecation (expiration against closed glottis increases abdominal pressure) Sigh, hiccough, yawn |
|
|
What is the relative importance of chemical and neuronal control of ventilation? |
Chemical primary importance, adjusts to body's metabolic needs Neural secondary importance - modifies pattern rather than regulating overall level |
|
|
How is the increase in oxygen consumption during exercise achieved? |
Increase in ventilation (30-fold) Increase in CO (4-5-fold) |
|
|
What is minute volume? |
Volume of gas that goes in and out of the lungs in one minute |
|
|
What is tidal volume? |
Volume breathed in and out at rest |
|
|
What is vital capacity (VC)? |
Greatest volume that can be expired from a position of maximal inspiration |
|
|
How do breathing parameters change during exercise? |
Breathing rate: 10-12 --> 50 /min TIdal volume: 500ml --> 50% of VC (2-2.5L) |
|
|
Anaerobic threshold graph of gasses |
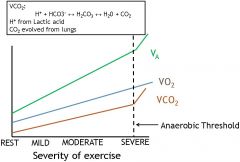
Image |
|
|
Anaerobic threshold graph of blood parameters |
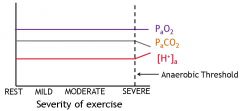
Image |
|
|
How is V/Q affected by exercise? |
Increases with exercise intensity (respiratory rate increases more than CO) Rest: 0.8 Mild/ moderate: 1.0 (ideal) Severe: 2-3 |
|
|
How is lung diffusing capacity (DL) affected by exercise? |
Increases with exercise intensity Measure of ability of lung to conduct gases, affected by SA available for exchange which increases 4-fold in severe exercise |
|
|
Pattern of ventilation in response to exercise |
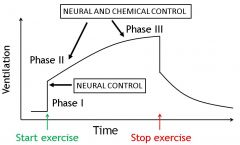
Image |
|
|
Which chemical factors affect the pattern of ventilation? |
Decreased PaO2, increased PaCO2, decreased pHa, increased body temperature - all unlikely Increased plasma [K+] - temporal relationship with ventilation - may have role in phases II and III |
|
|
Respiration summary |
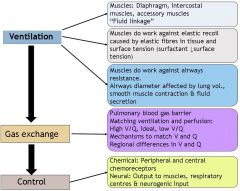
Image |
|
|
Which static lung volumes cannot be measured using spirometry? |
Residual volumes |
|
|
What is the normal FEV1/FVC ratio in health? |
0.8 Note: both measures of forced expiration |
|
|
What does a FEV1/FVC ratio of >0.7 indicate? |
Increase in FEV1 from decreased pulmonary compliance meaning restrictive disease |
|
|
What does a FEV1/FVC ratio of <0.7 indicate? |
Obstructive disease - only FEV1 that decreases therefore reducing the ratio |
|
|
If the FEV1/FVC ratio suggests an obstructive disease, how can asthma and COPD be distinguished from each other? |
Good history Reversibility test - bronchodilator before and 15 mins after spirometry test |
|
|
What is the measurable parameter for respiratory acidosis? |
High PCO2 (>40 mmHg) |
|
|
What is the primary defect in respiratory acidosis? |
Hypoventilation (decrease in minute ventilation) |
|
|
What are the causes of respiratory acidosis? |
Obstructive airway diseases Drugs (morphine, sedatives, anaesthesia) Inadequate ventilation CNS trauma Spinal cord injury above C4 Toxic insult (pesticides, snake venom) |
|
|
How is respiratory acidosis compensated for? |
Acute: intracellular buffering of CO2 due to Hb, protein, phosphate (not HCO3-) Chronic: Increased HCO3- generation in proximal tubule (glutamine breakdown) |
|
|
What is the measurable parameter for respiratory alkalosis? |
Low PCO2 (<40 mmHg) |
|
|
What is the primary defect in respiratory alkalosis? |
Hyperventilation (increase in alveolar ventilation) |
|
|
What are the causes of respiratory alkalosis? |
Panic attacks Asthma Mechanical ventilation Salicylate OD (chemoreceptors) Hypoxaemia (mountain sickness) Head injury Chronic liver disease Pregnancy |
|
|
How is respiratory alkalosis compensated for? |
Self-corrects as pCO2 potent driver of ventilation - decreases If chronic, inhibition of glutamine breakdown to HCO3- in kidneys |
|
|
What is the measurable parameter for metabolic acidosis? |
Low HCO3- (<24 mmol/L) |
|
|
What is the primary defect in metabolic acidosis? |
Decrease in HCO3 concentration in plasma |
|
|
What are the causes of metabolic acidosis? |
Increased acid production (lactic/ ketoacidosis) Acid ingestion (solvent abuse) Decreased renal acid secretion GI/ renal HCO3- loss (e.g. diarrhoea) |
|
|
How is metabolic acidosis compensated for? |
Correcting high acid problem through other buffers or decreasing [H+] Also increasing ventilation rate |
|
|
What is the measurable parameter for metabolic alkalosis? |
High HCO3- (>24 mmol/L |
|
|
What is the primary defect in metabolic alkalosis? |
Increase in HCO3 concentration in plasma |
|
|
What are the causes of metabolic alkalosis? |
Increases GI acid loss (vomiting) Increased renal acid loss (hypokalaemia) HCO3- retention (inappropriate IV HCO3/ citrate) |
|
|
How is metabolic alkalosis compensated for? |
Change in equilibrium in intracellular buffers to release H+ Correcting hypokalaemia/ loss of Cl- (e.g. gastric vomiting) Also decrease in ventilation rate |
|
|
What is the effect of exercise and blood pressure? |
Increased pulse, systolic and diastolic pressures HR increases by relatively more |
|
|
What parameter does pulse pressure relate to? |
Cardiac output |
|
|
How does lying down affect pulse rate and blood pressure? |
HR ~25% lower BP unchanged Pulse pressure drops - opposite effect to exercise |
|
|
What is postural hypotension? |
More than 20 mmHg difference between lying and standing. Lower when standing due to baroreceptor reflex |
|
|
What are the three stages in kidney development? |
Pronephros (fore) Mesonephros (mid) Metanephros (hind) |
|
|
How is the pronephros formed? |
Derived from intermediate mesoderm Appears in developing cervical region Non-functional |
|
|
When does the pronephros appear? |
Beginning of week 4 with formation of nephrotomes which connect with left and right pronephric ducts, grow towards cloaca Degenerates by end of week 4 |
|
|
How is the mesonephros formed? |
End of week 4, pronephric duct stimulates intermediate mesoderm Forms 40 mesonephric tubules in thoracic region - wave of activity thoracic to lumbar |
|
|
What is the pronephric duct in the thoracic-lumbar region called? |
Mesonephric (Wolffian) duct |
|
|
When does the mesonephros degenerate? |
During weeks 10-12 Has some urinary function |
|
|
Vascularisation and morphology of mesonephros |
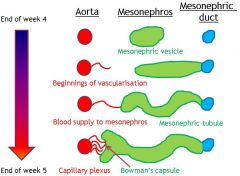
Image |
|
|
What does the metanephros develop from? |
Ureteric bud in future pelvic region |
|
|
How does the metanephros develop? |
Ureteric bud grows into surrounding mass of intermediate mesoderm - 'metanephric mass' Branches, forms lobules |
|
|
What are the common kidney developmental defects? |
Unilateral renal agenesis Unilateral renal hypoplasia Supernumerary kidney |
|
|
What is renal ectopia? |
Failure in migration - kidney can remain in pelvis instead of migrating to posterior abdominal wall |
|
|
What is abnormal kidney rotation? |
Hilum faces ventrally rather than medially |
|
|
What causes supernumary renal vessels? |
Failure of regression of transient renal vessels - ureter can be trapped by vessels - leads to hydronephrosis (buildup of urine) |
|
|
How does the bladder develop? |
Mesonephric ducts absorbed into bladder Trigone (smooth rectangular region) formed fro mesonephric ducts which give rise to vas deferens in the male |
|
|
What are the key parts of the bladder during development? |
Urachus - gives rise to medial umbilical ligament Urorectal septum - gives rise to perineal body |
|
|
How do the lungs develop at 4-5 weeks? |
Laryngotracheal origice (groove) appears in caudal pharynx Endoderm lining of groove will become pulmonary epithelium Groove becomes layngotracheal (respiratory) diverticulum (lung bud) Mesenchyme added, enlarges to form respiratory bud Whole respiratory tree develops from this bud |
|
|
What is the tracheoesophageal septum and how is it formed? |
Separates dorsal (gut) and ventral (larynx, trachea, bronchi, lungs) parts of tube Tracheoesophageal folds within the lung bud fuse to form tracheoesophaeal septum |
|
|
What is tracheoesophageal fistula (TEF)? |
Abnormal passage between oesophagus and trachea caused by defect in formation of tracheoesophageal septum Associated with oesophageal atresia |
|
|
What is Tracheal stenosis and tracheal atresia? |
Uncommon narrowing/ blockage of trachea due to not being equally separated from oesophagus. Associated with TEF |
|
|
What is tracheal diverticulum? |
Blind ended bronchus branches from trachea - susceptible to infection |
|
|
How many generations of branches are present in the lungs? |
23 |
|
|
Lung maturation timeline |
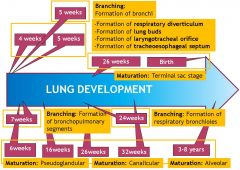
Image |
|
|
What is the intrinsic coagulation pathway? |
XII XIIa XIa IXa VIIIa (+ Ca, phospholipid) Xa Monitored by Activated Partial Thromboplastin Time (APTT) |
|
|
What is the extrinsic coagulation pathway? |
III (tissue factor) VII Xa Monitored by Prothrombin Time (PT) |
|
|
What is the function of coagulation factor Xa? |
Converts prothrombin (II) to thrombin (IIa) |
|
|
What is the common coagulation pathway? |
I (fibrinogen) + thrombin Fibrin + XIIIa Cross-linked fibrin Monitored by Thrombin Time (TT) |
|
|
What is the function of Anti-Thrombin (AT)? |
Inhibits factor X and thrombin Activity enhanced by heparin |
|
|
What are the functions of proteins C and S? |
Inactivate cofactors V and VIIIa Inhibits Vit K factors C initially activated by thrombin/ thrombomodulin on endothelial cell surface S acts as co-factor for C |
|
|
What is the basis of water distribution in the body? |
All compartments freely permeable, moves in presence of osmotic gradient Number of osmotically active particles determines compartment size Cell actively protects volume by gain/ loss of osmolytes Volume of interstitium and plasma determined by starling forces, dependent on oncotic pressure in plasma |
|
|
What is regulatory volume increase? |
Response to cell shrinkage (hypertonic environment) Sodium enters cells via Nc/Cl/K co-transporter Chloride enters cells via HCO3-/Cl- antiporters |
|
|
What is regulatory volume decrease? |
Response to cell swelling (hypotonic environment) Potassium and chloride both leave the cell via K/Cl symporters |
|
|
What is the importance of fluid volume control? |
Blood - control of BP, organ perfusion Interstitium - prevention of oedema Cells - protection against swelling/ shrinking Rapid changes in fluid balance that outstrip regulatory responses can be fatal |
|
|
What is iso-osmotic dehydration? |
NaCl loss = H2O loss Caused by vomiting, diarrhoea, blood loss and burns. Decreased extracellular fluid volume (iso-osmotic) |
|
|
What is hypo-osmotic dehydration? |
NaCl loss > H2O loss (cause of reduced osmolarity) Caused by adrenal insufficiency. Decreased osmolarity of both intracellular and extracellular fluid. Increased intracellular volume, decreased extracellular volume. Loss of hyperosmotic fluid (high solute). |
|
|
What is hyper-osmotic dehydration? |
NaCl loss < H2O loss Caused by fever, diabetes insipidus, diabetes mellitus. Increased intracellular and extracellular osmolarity. Decreased intracellular and extracellular osmolarity. Loss of hypo-osmotic fluid (low solute) |
|
|
What is central diabetes insipidus? |
Impaired ADH secretion, damage to hypothalamus or osmoreceptors Caused by head trauma, hypoxia, ischaemia |
|
|
What is nephrogenic diabetes insipidus? |
Impaired renal response to ADH, washout of medullary hypertonicity No functional V2 receptors Caused by lithium therapy, sickle cell anaemia, mutations in V2 receptors |
|
|
What are bucket handle respiratory movements? |
Change dimensions of thorax in lateral direction Elevation of rib shafts causes increase in volume laterally |
|
|
What are pump handle respiratory movements? |
Change dimensions of thorax in anteroposterior direction Elevation of ribs causes anterior and superior movement of sternum - increases volume |
|
|
Which ribs are typical? |
2-9 |
|
|
Which ribs are true? |
1-7 |
|
|
Which ribs are false? |
8-10 |
|
|
Which ribs are floating? |
11-12 |
|
|
Which muscles are used during inspiration? |
Diaphragm External intercostals Accessory muscles: - Sternocleidomastoids - Scalenes - Pectoralis minor - Quadratus lumborum |
|
|
Which muscles are used during expiration? |
Internal intercostals Abdominal muscles |
|
|
What is the action of intercostal muscles? |
To keep intercostal space (ICS) rigid Prevents spaces being blown out during expiration or in during inspiration |
|
|
What are the features of the innermost layer of intercostals? |
Deep to internal intercostals Comprised of: - Innermost intercostals - Subcostal and transverse thoracic |
|
|
What is the function of accessory muscles? |
May be used for quiet respiration in individuals with asthma, emphysema, neuromuscular disorders - Also during/ recovery from strenuous exercise |
|
|
Where are the accessory muscles located? |
Sternocleidomastoid - Sternum, clavicle, mastoid process Scalene - C1-5, ribs 1-2 Pectoralis minor Quadratus lumborum - 12th ribs - iliac crest Others e.g. serratus anterior and posterior |