![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
127 Cards in this Set
- Front
- Back
|
Which 2 cardiac rhythms require defibrillation? |
Ventricular fibrillation & pulse-less ventricular tachycardia |
|
|
Which cardiac rhythms potentially require cardioversion with a defibrillator? |
Cardioversion mode may be used for rapid symptomatic cardiac arrhythmias e.g. atrial fibrillation, supraventricular tachycardia, or ventricular tachycardia with a pulse. |
|
|
When would you use a defibrillator for external pacing (transcutaneous pacing)? |
External pacing is typically used in symptomatic bradycardias & atrioventricular heart blocks that are unresponsive to drug therapy. |
|
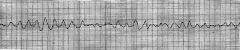
What is this trace showing? |
Ventricular fibrillation --> a rapid, ineffective quivering of the ventricles which will not pump blood. Electrical activity originates in the ventricles & spreads in a chaotic, irregular pattern throughout both ventricles. |
|
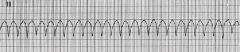
What is this trace showing? |
Ventricular tachycardia --> a fast heart rhythm that originates from an ectopic focus in one of the ventricles. Pulseless VT is identified if the patient has no pulse & requires immediate defibrillation. Pulsatile VT is identified if the patient has a pulse; consider vagal maneuvers, anti-arrhythmic medications, & cardioversion. |
|
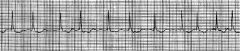
What is this trace showing? |
Atrial fibrillation --> a rapid, irregular rhythm that originates from an ectopic focus in the atria, impairing atrial contraction & effective emptying. If the patient is symptomatic, consider medication to control the heart rate or cardioversion. This is an irregularly irregular rhythm. |
|
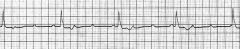
What is this trace showing? |
Third-degree atrioventricular block / complete heart block --> an abnormally slow heart rate in which the impulses generated in the SA node do not pass through the AV node to the ventricles, therefore there is complete AV dissociation. If the patient is unstable (reduced LOC, hypotension, cardiac failure, acute pulmonary oedema, chest pain) consider medication to increase rate or commence transcutaneous pacing. |
|
|
What is the correct positioning of the defibrillator pads? |
- Right sternal region on the mid-clavicular line & the second intercostal space - Left mid-axillary line on the 6th intercostal space |
|
|
What the amount of energy recommended by the Australian Resuscitation Council for defibrillation? |
200J |
|
|
What is the correct positioning of the defibrillator pads in the anterior-posterior position? |
- Anterior pad on the left parasternal region over the apex of the heart - Posterior pad on the left scapular region, directly opposite the anterior pad |
|
|
How do you assess airway patency? |
Look: is there obvious chest movement? Listen: if the patient is making audible words then they have a patent airway Are there gurgling or snoring sounds? This could mean partial obstruction by the tongue Feel at the mouth for expired air Assess for hypoxia (i.e. pulse oximetry) |
|
|
Are any of these manoeuvres safe to use in a patient with suspected cervical spine injury? A. Head tilt B. Chin lift C. Jaw thrust |
Both chin lift & jaw thrust can be used in patients with suspected C-spine injury, but not head tilt |
|
|
How do you select the appropriate size of Guedel / oropharyngeal airway adjunct? |
Line up the tip so it sits just behind the angle of the jaw & check to see if the other end is sitting parallel with the lips |
|
|
When inserting a nasopharyngeal airway, which way should the bevel be facing? |
It is inserted with the bevel facing the septum & then rotated to avoid trauma to the nasal turbinates |
|
|
When is a nasopharyngeal airway not recommended? |
When the patient has a base of skull fracture. |
|
|
What are the two classifications of airway obstruction? |
Anatomical obstruction --> results from mechanical blockage of the airway Functional obstruction --> results from conditions that reduce muscle tone in the upper airway e.g. sedation, narcosis, coma |
|
|
As a rough guide, below which GCS is patient not able to protect their airway |
GCS 8 or below will not be able to protect their own airway & intubation may be required (depending on context & whether the cause of the ALOC is rapidly reversible or not) |
|
|
How do you create a protected airway in an unconscious patient (i.e. GCS <9)? |
A cuffed endotracheal tube. A laryngeal mask airway (LMA) will only create a patent airway, not a protected one, as patient's can still aspirate. |
|
|
How do you assess breathing? |
Look: respiratory rate, chest expansion, work of breathing, accessory muscle use, do they look breathless or like they are working hard? Listen: chest auscultation, speech (words, phrases, sentences?) Feel: trachea midline, tracheal tug, chest percussion Assess: pulse oximetry, also consider spirometry (peak flow rate), CXR |
|
|
What should you do if a patient has a low pulse oximeter reading? |
- Check a waveform exists - Check that the oximeter is on properly - Ensure that the inspiratory oxygen is sufficient - Check that peripheral circulation is adequate - If doubt exists, check ABG |
|
|
Define hypoxaemic respiratory failure & list the possible mechanisms |
Hypoxaemia = low arterial PO2 (PaO2 <60mmHg) There are five mechanisms: - Shunt - Ventilation-perfusion mismatch - Impaired diffusion - Hypoventilation (usually causes hypercapnia as well) - Low FiO2 |
|
|
How do you treat hypoxaemia? |
SUPPLEMENTAL OXYGEN If it's due to hypoventilation or low FiO2 then it should respond rapidly, however hypoxaemia due to a shunt is harder to treat with supplemental oxygen. Use minimal O2 in patients with hypoxic respiratory drive - target SaO2 92% In all patients, use the least supplemental oxygen required to maintain appropriate oxygen saturations. |
|
|
What is the recommended oxygen flow rate when using nasal prongs? |
1 - 4 L/min FiO2 0.24 - 0.32 Flows above 6L/min via NP leads to drying of the nasal mucosa & discomfort |
|

What sort of mask is this? |
Hudson mask |
|
|
What oxygen flow rates are appropriate with a Hudson mask? |
6 - 10L/min (NOTE: never use a flow rate <5L/min as it will lead to rebreathing) FiO2 will vary depending on oxygen flow rate, respiratory rate, & patient maximum inspiratory flow rate. Flow rates of 6 - 10L/min will result in an FiO2 of 0.4 - 0.5 |
|

What sort of mask is this? |
A non-rebreather mask |
|
|
What FiO2 & oxygen flow rates are appropriate for a non-rebreather oxygen mask? |
FiO2 will vary depending on oxygen flow rate, respiratory rate, & patient maximum inspiratory rate. Flow rates of 10 - 15L/min will achieve an FiO2 of 0.5 - 0.8 |
|

What sort of mask is this? |
A Venturi mask |
|
|
What FiO2 & oxygen flow rates are appropriate for a Venturi mask? |
These masks can reliably deliver FiO2 values of 0.24 - 0.6 (the only system when FiO2 is known & can be carefully titrated). Devices vary but oxygen flow rate may be 3 or 6L/min (flow rate needs to be changed depending on required FiO2) |
|
|
What is the required oxygen flow rate for a self inflating bag? |
Always 15L/min flow rate FiO2 is 0.9 - 1.0 The self inflating bag provides a means to ventilate patients i.e. will work in apnoeic patients. |
|
|
Define hypercapnic respiratory failure & the causes. |
Hypercapnic respiratory failure = PaCO2 >50mmHg Increased PaCO2 implies a failure of ventilation PaCO2 is inversely proportional to alveolar ventilation (Va) If ventilation doubles then PaCO2 halves Possible causes of ventilation failure include: - Reduced respiratory drive e.g. sedation, coma, narcosis - Neuromuscular weakness e.g. spinal injury, GBS - Ventilatory failure e.g. kyphoscoliosis - Other medical causes e.g. COAD, asthma |
|
|
How can you tell if a patient's hypercapnia is chronic or acute? |
Look at the HCO3 for clues - if bicarbonate is high then high PaCO2 is likely chronic |
|
|
What are the 3 components of general anaesthesia? |
Unconsciousness Muscle relaxation Analgesia |
|
|
What are the phases of anaesthesia? |
Pre-operative --> patient assessment & preparation, equipment preparation Peri-operative --> pre-induction, induction, maintenance, emergence Post-operative |
|
|
What are the elements of a pre-anaesthetic assessment? |
Patient questionnaire --> previous surgeries, family history, medications etc Medical assessment --> past medical / surgical history, medication review Focused anaesthetic assessment --> previous anaesthetics, family history of difficulties with anaesthetics Concurrent illness --> systems review, exercise tolerance (indicator of cardiorespiratory reserve, ability to climb 2 flights of stairs is an acceptable reserve) Medication history --> prescription & non-prescription, alcohol, tobacco, herbal, allergies / ADRs Dentition --> note caps, crowns, or unhealthy teeth, risk of damage from airway instrumentation Investigations as required --> not usually needed for healthy patients undergoing minor surgery GORD --> risk of aspiration under anaesthesia, check for severity, commence / continue anti-reflux therapy |
|
|
Describe the ASA scoring system. |
1. Fit & well 2. Mild systemic disease, no functional impairment 3. Systemic illness affecting everyday life 4. Systemic illness that is a constant threat to life 5. Moribund - not expected to survive with or without surgery 6. Brain dead organ donor E. Can be added to any number to denote 'emergency surgery' - i.e. no pre-operative workup done |
|
|
What are some of the signs of impending deterioration? |
Deranged vital signs --> blood pressure, heart rate, respiratory rate, temperature --> very high or very low Nonspecific physical signs --> e.g. patient is peripherally shut down or is working hard at breathing e.g. patient looks sick |
|
|
What is the most sensitive trigger / indicator of impending arrest? |
Tachypnoea |
|
|
What is the definition of sepsis? |
Life threatening organ dysfunction caused by a dysregulated host response to infection. |
|
|
How can you tell whether a patient with an infection has sepsis? |
qSOFA --> quick Sepsis-related Organ Failure Assessment Two or more of the following: 1. Respiratory rate >22 2. Altered mental state 3. Systolic BP < 100mmHg |
|
|
Define Acute Respiratory Distress Syndrome (also known as non-cardiogenic pulmonary oedema). |
An acute process, occurring within 7 days of a known trigger (e.g. shock, trauma, severe pneumonia). There is significantly impaired oxygenation (PaO2/FiO2 <300) & bilateral diffuse infiltrates will be seen on CXR. It is NOT caused by a cardiac problem. |
|
|
What are some of the possible triggers of ARDS? |
Direct lung injury --> aspiration of gastric contents, near drowning, smoke or toxic chemical inhalation, pulmonary contusion, pneumonia Indirect lung injury --> shock, sepsis, pancreatitis, massive tranfusion, fat embolism |
|
|
How is septic shock defined? |
Sepsis with hypotension (MAP < 65mmHg or SBP < 90mmHg) and raised serum lactate (> 2mmol/L). Classically high cardiac output, low vascular resistance ('warm shock'), extravasation of fluid, hypovolaemia. |
|
|
Describe the management of septic shock. |
1. Correct the underlying cause 2. Appropriate abx therapy early 3. Fluid resuscitation - isotonic crystalloids or colloids 4. Correction of shock: vasopressors (noradrenaline, metaraminol), inotropes |
|
|
Define acute kidney injury. |
Either: - Increase in serum creatinine by >26 umol/L (>0.3 mg/dL) in 48hrs OR - Urine volume <0.5mL/kg/hr for >6hrs |
|
|
Describe the management of acute kidney injury. |
1. Correct the underlying cause 2. Exclude other treatable causes e.g. ureteric / urethral obstructions 3. Avoid further nephrotoxins e.g. gentamicin, radiographic contrast 4. Aim for euvolaemia, correct hypovolaemia 5. Maintain renal perfusion pressure, avoid hypotension 6. Dialysis if required |
|
|
What are 3 ways to optimise cardiac output? |
1. Optimise preload by adequate filling (i.e. fluid loading) 2. Optimise cardiac output with inotropes 3. Optimise BP with vasopressors |
|
|
What indicators can you use to help gauge the severity of a patient's dyspnoea? |
- Respiratory rate - Work of breathing - Tracheal tug, accessory muscles - Ability to speak - words, sentences, phrases - Mental status - Arterial oxygenation - oximetry - Onset acute or acute-on-chronic? - Peak expiratory flow rate (PEF) for asthmatics - compare to normal PEF |
|
|
What's the initial management of severe acute asthma? |
- Oxygen via mask - Salbutamol 5mg nebulised with 3mL saline (repeat up to 3 times, then regularly every 15 - 60min) - Ipratropium 500ug nebulised QID (bronchodilator) - Give prednisone 50mg PO or hydrocortisone 250mg IV - Consider IV magnesium bolus |
|
|
Compare moderate to severe asthma (heart rate, PEF, ability to speak etc). |
Moderate asthma --> speaks phrases, HR 100 - 120 (note that salbutamol increases HR), PEF 50 - 75%, wheeze often moderate to loud Severe asthma --> speaks words, HR >120, PEF < 50% predicted (or <100L/min), wheeze often absent, SaO2 low |
|
|
What are the features of life-threatening asthma? |
- Inability to perform a PEF, or PEF <30% predicted - Silent chest or feeble respiratory effort - Bradycardia, dysrythmia, hypotension - Exhaustion, confusion, or decreased LOC - PaO2 < 60mmHg, or PaCO2 > 45mmHg |
|
|
What are some of the markers of severity in pneumonia? |
- Confusion - SaO2 <90% on air - Resp rate > 30 - Hypotension - Multiple lobes involved These are associated with ICU requirement |
|
|
What are the physical signs of a pneumothorax? |
- Reduced chest expansion on affected side - Increased percussion note - Reduced breath sounds - Tension pneumothorax suggested by --> extreme respiratory distress, elevated JVP, hypotension, tracheal shift to contralateral side |
|
|
What is the management of acute pulmonary oedema? |
- High flow oxygen - GTN sublingual or IV (must be monitored) - Diuresis (IV frusemide) - Non-invasive ventilation (CPAP) - If hypotensive, consider inotropes & urgent cardiology involvement (poor prognosis) - Treat the underlying cause of the oedema e.g. heart failure due to ischaemia, may need urgent revascularisation |
|
|
What is the normal range of pH on an ABG? |
pH: 7.35 - 7.45 |
|
|
What is the normal range of CO2 on an ABG? |
PCO2: 35 - 45mmHg |
|
|
What is the normal range of O2 on an ABG? |
PO2: 75 - 100mmHg |
|
|
What is the normal range of HCO3 on an ABG? |
HCO3: 22 - 28mmol/L |
|
|
What is the normal range of base excess on an ABG? |
Base excess: -2 to +2mmol/L |
|
|
How do you know that full respiratory compensation has occurred in metabolic acidosis/alkalosis? |
The PCO2 level will be the same is the last 2 digits of the pH. E.g. pH 7.26 pCO2 26mmHg PO2 85mmHg HCO3 15mmol/L Base excess -8mmol.L |
|
|
How do you determine the magnitude of acidosis / alkalosis? |
For metabolic disorders, the base excess indicates the magnitude. For respiratory disorders, the PCO2 indicates the magnitude. |
|
|
What are some of the possible causes of a metabolic alkalosis? |
Metabolic alkalosis is generally caused by loss of H+ ions from the gut or kidney, or the shift of H+ ions into cells. Alkalosis will also be perpetuated by hypovolaemia. Gut loss --> NG suction, vomiting Renal loss --> aldosterone excess (steroid therapy), diuretics Shift into cells --> insulin therapy, hypokalaemia |
|
|
What are the 2 different ways the anion gap can be calculated? |
(Na + K) - (HCO3 + Cl) --> ref range 10 - 14mmol/L OR Na - (HCO3 + Cl) --> ref range 6 - 10mmol/L |
|
|
What are some possible causes for wide anion gap acidosis? |
The anion gap is elevated because of the presence of an unmeasured anion. There are 4 types of unmeasured anion: 1. Ketones --> DKA, starvation ketoacidosis, alcoholic ketoacidosis 2. Lactate --> lactic acidosis due to shock, sepsis, ischaemia etc. 3. Renal failure --> sulphates, phosphates, & others 4. Drugs / poisons --> methanol, ethylene glycol, salicylates |
|
|
What are some possible causes for normal anion gap acidosis? |
Normal anion gap acidosis usually involves loss of bicarbonate from the gut or kidneys. Loss from the gut --> diarrhoea, ileostomy, pancreatic fistula Loss from the kidneys --> renal tubular acidosis, K+ sparing diuretics (aldosterone blocking drugs) Excess chloride --> normal saline resuscitation |
|
|
How do you calculate the inspired partial pressure of oxygen (PiO2)? |
PiO2 = FiO2 x (PB - 47) FiO2: fraction of inspired oxygen PB: barometric pressure 760mmHg 47: humidified air has a fixed water vapour pressure of 47mmHg at 37C |
|
|
How do you calculate the alveolar PAO2? |
PAO2 = PiO2 - (PaCO2/R) PaCO2: arterial CO2, obtained from ABG R: respiratory quotient, assumed to be 0.8 |
|
|
How do you calculate the alveolar-arterial (A-a) gradient? |
A-a gradient = PAO2 - PaO2 A-a gradient = [(FiO2 x 710) - (PaCO2/0.8)] - PaO2 |
|
|
What is the normal A-a gradient? |
5 - 10mmHg in a young healthy person on room air |
|
|
What are some of the risk factors for ischaemic stroke? |
Hypertension Smoking Diabetes Carotid artery stenosis Atrial fibrillation Coronary heart disease Elevated cholesterol Blood dyscrasias Obesity Physical inactivity Oral contraceptives or HRT |
|
|
What investigations should be performed for a transient ischaemic attack (TIA)? |
CT head ECG Carotid duplex studies +/- echocardiography +/- procoagulant screen Note: TIA is associated with a 10% risk of completed CVA within 90 days (highest risk within 48hrs) |
|
|
What is the FAST campaign? |
Public education for signs of stroke: Face - facial asymmetry / drooping Arms - can they lift their arms? Speech - is their speech slurred? Time - call 000, time is brain tissue |
|
|
What is involved in early management of stroke? |
Check BGLs --> if hypo then treat to normal levels Neurological assessment IV access --> FBC, Chem20, coags Activate stroke team Urgent CT scan 12 lead ECG Control temperature --> hyperthermia associated with poorer outcome |
|
|
What is the target blood pressure when managing patients with ischaemic stroke? |
Systolic BP up to 220mmHg & diastolic BP up to 120mmHg Note: aggressive control of hypertension may reduce perfusion to the ischaemic penumbra & has a poorer outcome in clinical trials. |
|
|
What are the common locations for aneurysms that cause subarachnoid haemorrhage? |
Internal carotid - 40% Anterior communicating - 35% |
|
|
What are some of the risk factors for development of an aneurysm? |
Hypertension Polycystic kidney disease Family history Smoking |
|
|
What is the appropriate management for a patient with a subarachnoid haemorrhage? |
Intubate if GCS < 9 Control BP - target SBP <150mmHg before the aneurysm is secured Provide analgesia Refer to neurosurgeon for aneurysm clipping or angiographic coiling Nimodipine to reduce vasospasm risk Consider seizure prophylaxis - empiric phenytoin |
|
|
What is the Monro-Kellie doctrine? |
The brain is housed in a rigid container (the skull). Contents: neural tissue (brain) - 1400mL; CSF - 75mL; blood - 100 - 150mL An increase in the volume of one component requires a decrease in the volume of the other two to maintain pressure at normal values. |
|
|
What is the normal CSF pressure? |
5 - 13 mmHg (or 7 - 18cm H2O) |
|
|
Cerebral blood flow is regulated by & dependent on: |
- Cerebral metabolism & functional activity - PaCO2 - Arterial oxygen content - Mean arterial pressure |
|
|
Describe the GCS criteria used to classify a traumatic brain injury as mild, moderate, or severe. |
GCS 13 - 15: mild (80% of cases) GCS 9 - 12: moderate (10% of cases) GCS < 9: severe (10% of cases) |
|
|
What are some specific management tasks for managing severe traumatic brain injury? |
- Optimise oxygenation, ventilation, & blood pressure --> most important steps - Hyperventilation will transiently reduce ICP, should only be used for <1hr - Osmotherapy may be useful to reduce intracranial volume --> mannitol 0.5g/kg (i.e. 200mL of 20%) or 3% (hypertonic) saline - Phenytoin 15-20mg/kg slow IV bolus may reduce incidence of early seizures Management goals: - pO2 > 90mmHg - pCO2 ~ 35mmHg - BSL 4 - 10mmol/L - Avoid hyperthermia - ICP < 20mmHg - Cerebral perfusion pressure (CPP) > 60mmHg [CPP = MAP - ICP] |
|
|
What are the Canadian CT Head Rules high risk criteria? |
CT head is DEFINITELY required if: - GCS < 15 at 2hrs after injury - Suspected open or depressed skull fracture - Evidence of basal skull fracture (haemotympanum, racoon eyes, CSF otorrhoea or rhinorrhoea, Battles sign) - Vomiting > 2 episodes - Age > 65 - Amnesia for > 30min before impact - Dangerous mechanism (pedestrian struck, ejected from vehicle, fall from >3m or 5 stairs) |
|
|
List the possible poisons for the following toxidrome: Sympathetic activity --> tachycardia, hypertension, pupil dilation, pyrexia, flushing |
Amphetamines Ecstasy Ice Cocaine Cough & nasal decongestants Theophylline |
|
|
List the possible poisons for the following toxidrome: Parasympathetic activity --> diarrhoea, urinary incontinence, sweating, salivation, bronchorrhoea, bradycardia |
Organophosphates Anticholinesterases used for myasthenia gravis |
|
|
List the possible poisons for the following toxidrome: Anticholinergic activity --> tachycardia, hot dry skin, dry mouth - similar to sympathetic activity but with added weakness & seizures |
Tricyclic antidepressants (TCA) Antihistamines Antiparkinsonians Atropine Antispasmodics Phenothiazines Datura (Angel's Trumpet) |
|
|
List the possible poisons for the following toxidrome: Metabolic acidosis --> tachypnoea, Kussmaul breathing, decreased bicarbonate |
Ethanol Methanol Ethylene glycol (antifreeze) Iron Salicylate Carbon monoxide Cyanide |
|
|
Which poisons tend to cause vomiting? |
Theophylline Chloroquine Lithium Aspirin Iron Corrosives (bleach) |
|
|
Which poisons tend to cause acute renal failure, as evidenced by haematuria, myoglobulinuria, oliguria, or anuria? |
Ethylene glycol (antifreeze) Mushroom poisoning Snake bite |
|
|
List the possible poisons for the following toxidrome: Ataxia / nystagmus |
Alcohol Anticonvulsants Barbituates Antihistamines Organic solvents Carbon monoxide |
|
|
List the possible poison for the following toxidrome: Chemical pneumonitis --> cough, wheeze, non-cardiogenic pulmonary oedema, haemoptysis, CNS depression |
Kerosene Turpentine Eucalyptus oil |
|
|
What is the antidote for paracetamol overdose? |
N-acetylcysteine (NAC) IV infusion over 24hrs |
|
|
What is the antidote for opiate overdose? |
Naloxone |
|
|
What is the antidote for TCA overdose? |
Bicarbonate |
|
|
What is the antidote for beta blocker overdose? |
Calcium & glucagon |
|
|
What is the antidote for digoxin overdose? |
Digoxin antibodies |
|
|
What is the antidote for organophosphate poisoning? |
Atropine & pralidoxime |
|
|
What is the antidote for thyroxine overdose? |
Propanolol |
|
|
What is the antidote for iron toxicity? |
Desferrioxamine |
|
|
What are the features of paracetamol overdose? |
Toxic metabolite (NAPQI) may result in acute hepatic necrosis with acute liver failure. Associated with hypotension, hypoglycaemia, metabolic acidosis, & renal failure. Higher risk of liver injury in patients with: - Chronic alcohol abuse - Microsomal-inducing drugs e.g. carbamazepine - Reduced liver glutathione stores (prolonged fasting, malnourishment incl. HIV, malignancy, anorexia, bulimia) - Other acute liver injury (viral hepatitis, alcoholic hepatitis) |
|
|
What is the toxic dose of paracetamol in adults? |
10g (200mg/kg if under 50kg) In high risk groups the toxic dose is 100mg/kg or 4g |
|
|
What is the trimodal distribution of death in trauma cases? |
First peak --> 50% of cases --> early deaths, pre-hospital, severe injuries, difficult to prevent death Second peak --> 30% of cases --> 1 - 6 hours after injury, potentially preventable if managed well Third peak --> 20% of cases --> days to weeks after injury, ICU deaths, difficult to prevent |
|
|
What are the 3 main trauma centres in Qld? |
PAH, RBWH, Townsville General |
|
|
Describe the approach to the major trauma patient. |
- Primary survey --> ABCDE - Focused radiology --> CXR & pelvis X-ray - Secondary survey --> head to toe - Detailed radiology once patient stable --> CT, extremity injury radiology |
|
|
What are some of the life threatening chest injuries that may be seen in a major trauma case? |
Pneumothorax & tension pneumothorax Massive haemothorax Multiple rib fractures with flail Pulmonary contusion Sucking chest wound Aortic injury Myocardial contusion |
|
|
When performing ALS on a patient with a shockable rhythm, which drugs are use & when? |
Adrenaline 1mg after 2nd shock, & then every 2nd cycle Amiodarone 300mg after 3rd shock |
|
|
When performing ALS on a patient with a non-shockable rhythm, which drugs are use & when? |
Adrenaline 1mg immediately, & then every 2nd cycle |
|
|
What are the 4 H's & T's to consider & correct in an arrested patient? |
Hypoxia Hypovolaemia Hyper / hypokalaemia & other metabolic disorders (e.g. acidosis) Hypo / hyperthermia Tension pneumothorax Tamponade Toxins Thrombosis (pulmonary / coronary) |
|
|
Describe post-resuscitation care in a patient who had arrested. |
Re-evaluate ABCDE 12 lead ECG Treat precipitating causes Re-evaluate oxygenation & ventilation Temperature control (cool) |
|
|
How is amiodarone given in an arrest situation? |
300mg bolus --> drawn up in 20mL 5% dextrose (not saline) & give over 2 minutes with large flush |
|
|
When you would consider giving atropine in a MET call situation? |
Severe bradycardia Dose: 1mg repeated to a maximum of 3mg Note that <0.5mg may worsen bradycardia |
|
|
What drug do you administer in an arrest due to hyperkalaemia? |
Use calcium (5 - 10mL of 10% calcium chloride), large volume flush, bicarbonate |
|
|
What drug do you administer in an arrest due to calcium channel blocker overdose? |
5 - 10mL of 10% calcium chloride |
|
|
What drug do you administer in an arrest due to Torsades? |
Magnesium |
|
|
What drug do you administer in an arrest due to hypokalaemia? |
Potassium |
|
|
What are the effects of local anaesthetic toxicity? |
Caused by either IV or intra-arterial injection, or excessive infiltration. CNS effects --> circumoral tingling, dizziness, tinnitus, restlessness, progresses to shivering, muscle twitches, then generalised seizures & unconsciousness CVS effects --> affected at higher systemic doses than CNS, initially hypertension & tachycardia with CNS excitation, then arrhythmias, hypotension, & cardiac arrest |
|
|
What is the treatment for local anaesthetic toxicity? |
Stop administration of drug Airway Breathing Circulation Intralipid injection (acts as a lipid sink for LA agent) |
|
|
What is an IABP and when is it used? |
IABP = intra-aortic balloon pump It is used when ___- |
|
|
What is the immediate management of Acute Coronary Syndromes (UA, NSTEMI, STEMI)? |
Oxygen only if desaturating Nitroglycerin - if ischaemic type chest pain, then IV if persisting pain after 3 doses SL, or there is HTN or heart failure. Caution in RV infarction or severe AS, as the hypotension may cause decompensation Morphine - only if severe uncontrolled pain Beta blocker (metoprolol or atenolol) - if ongoing chest pain, HTN, or tachycardia not caused by heart failure. Avoid if haemodynamics unstable Statin - high dose, regardless of lipid levels Antiplatelet - aspirin 300mg + clopidogrel 600mg Anticoagulation - therapeutic clexane (? heparin if for invasive Mx) |
|
|
What is a TIMI score and how do you calculate it? |
TIMI: Thrombolysis in Myocardial Infarction study group risk score. Assesses outcomes in patients with UA or NSTEMI.
1pt each for: Age 65 or older 3 or more cardiac risk factors Known CAD (stenosis 50% or higher) Elevated troponins Aspirin use in last 7 days Severe angina within last 24hrs ST segment deviation 0.5mm or greater 0 - 2: low risk 3 - 4: moderate risk 5 - 7: high risk |
|
|
What are the ECG findings consistent with a STEMI?
|
New or presumed new ST elevation at the J point in two anatomically contiguous leads that meet the following thresholds:
- 1mm or more in all leads other than V2/3 - In V2/3: 2mm or more in >40M, 2.5mm+ in <40M, 1.5mm+ in women |
|
|
What are the ECG findings consistent with a NSTEMI?
|
New or presumed new horizontal or down-sloping ST depression >0.5mm in two anatomically contiguous leads AND/OR T-wave inversion >1mm in two anatomically contiguous leads with prominent R waves or R/S ratio >1 |
|
|
Which leads correlate to which anatomical regions of ischaemia on an ECG? |
Anterior wall ischaemia: two or more precordial leads (V1 - V6)
Anteroseptal ischaemia: V1 - V3 Apical or lateral ischaemia: aVL and I, V4 - 6 Inferior wall ischaemia: II, III, aVF RV ischaemia: right sided precordial leads Posterior wall ischaemia: V1-2, posterior precordial leads |
|
|
What is the acute management of stroke?
|
NIHSS score Urgent CT head +/- neck angio and CTP Assess timeline Call on call Neuro consultant Thrombolysis vs clot retrieval - Acute lysis window: <4.5hrs - Extended lysis window: 4.5 - 9hrs - Clot retrieval window: <16hrs BP Mx, aiming SBP <180, DBP <110 - Avoid GTN, will drop BP too quickly - IV hydralazine (5mg increments) or metoprolol (1mg increments) is better |
|
|
What are the inclusion criteria for acute lysis of stroke at TUH?
|
Age >18 Clinical diagnosis of stroke with demonstrable neurological deficits NIHSS score 4 or higher Onset of symptoms 0 - 4.5hrs ago Non con CT head that does not show haemorrhage, tumour, or mass effect No early infarct oedema (hypointensity seen on non con CT head) confirmed with TUH radiologist |
|
|
What are the absolute exclusion criteria for acute lysis of stroke at TUH? |
Hx of ICH, AVM, aneurysm, or intracranial neoplasm Any intracranial surgery, serious head trauma, or prev CVA in last 3/12 MI in last 3/12 Any GI or GUT haemorrhage in last 3/52 Major surgery, serious trauma, or CPR >2min in last 2/52 Biopsy, non-compressible arterial puncture, or LP in last 2/52 Known hypersensitivity to alteplase or contrast Symptoms rapidly resolving HTN despite Rx (SBP >185, DBP <110) Presentation suggestive of SAH (even with normal CT) Evidence of active bleeding or acute trauma Suspicion of septic emboli Other likely Dx Anticoagulants and INR >1.5 Receiving heparin within 48hrs and APTT raised Platelets <100 BGL <3 or >22.2 Positive bHCG in females |
|
|
What is the Modified Rankin Score?
|
A scoring system that ranks the degree of disability or dependence in the ADLs of people who have suffered a stroke or other causes of neurological disability. 0 - no symptoms at all 1 - no significant disability despite symptoms, can carry out all ADLs 2 - slight disability, able to look after own affairs without assistance 3 - moderate disability, requiring some help, but able to walk without assistance 4 - moderately severe disability, unable to walk and attend to bodily needs without assistance 5 - severe disability, bedridden, incontinent, requiring nursing care 6 - dead |