Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
71 Cards in this Set
- Front
- Back
|
Diagnosis of Dental Protrusion
|
1) Lips at rest more than 4mm apart
2) Strain to bring lips to closure 3) Prominence of lips in profile view Diagnosis must be made clinically, not from Ceph |
|
|
Incisor and Gingival Display
|
Ideal - Slightly below gingival margin
Max - Up to 4mm display of gingiva or 4mm lip coverage of incisor crown. More will start to appear unattractive. |
|
|
Tooth Ratios
|
Height-Width: Width of tooth should be 80% of Height
Apparent proportions - Every distal maxillary tooth should show 62% of the tooth mesial in frontal view. |
|
|
Connectors
|
The apparent contact between two teeth
Highest in centrals and moves incisally as you go posterior |
|
|
Minimal Diagnostic Records
|
Minimum
- Trimmed Casts - Pan with appropriate BW's and PA's - Data from Facial Form analysis Lateral Ceph and Facial/intraoral photos needed for all patients except mino or adjunctive treatments 3D imaging is needed for impacted teeth, skeletal asymmetry, and other special problems |
|
|
Quick check for Tooth size discrepancy
|
Anterior Size discrepancy
- Compare Upper and Lower laterals - Upper should be wider, or discrepancy almost surely exists Posterior Size discrepancy - Compare Upper and Lower 2nd Premolars - Should be about equal size Tooth size discrepancy of 1.5mm or more should be included in the problem list |
|
|
American Standard Ceph Arrangement
|
Patient Facing right
X-ray source is 5ft away from Mid-Saggital Plane Mid-Saggital plane to Film is 15cm. Can vary, but must be the same for any one patient every time. |
|
|
Three major Ceph Impositions
|
1) On anterior cranial base along SN line
- Shows overall pattern of changes in the face 2) On contour of palate behind maxillary incisors - Shows changes of maxillary teeth relative to maxilla 3) On inner surface of symphysis, outline of canal, and unerupted 3rd molar crypts - Shows changes of Condyle and Ramus, and changes to mandibular teeth relative to mandible. |
|
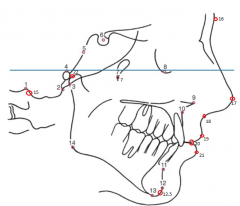
Name All 23 points and Define
|
1) Bolton Point Bo - Highest point in the upward curvature of retrocondylar fossa of occipital bone
2) Basion Ba - Anterior margin of Foramen Magnum. Base of clivus. 3) Articulare Ar - Intersection between shadow of zygomatic arch and posterior border of ramus 4) Porion Po - Midpoint of upper contour of EOM 5) Spheno-Occipital Synchondrosis SO 6) Sella S 7) Pterygomaxillary Fissure Ptm 8) Orbitale Or - Most inf part of orbital Rim 9) ANS 10) Point A 11) Point B 12) Pogonion Pog - Most anterior point of chin 12.5) Gnation aka Prognathion Gn - Most anterior inferior point of chin 13) Menton Me - Most inferior point of chin 14) Gonion Go - Midpoint of contour of connecting ramus and body 15) Opisthion Op - Posterior margin of Foramen Magnum 16) Glabella G - Most anterior part of forehead. Has Soft tissue counterpart 17) Pronasale Pr - Nasal tip 18) Subnasale Sn - Junction of columella with Philthrum 19) Labrare Superios Ls - Junction of upper lip and philthrum 20 ) Stomion - Upper and lower lips meet 21) Labrare Inferioris Li - Junction of lower lip and philthrum 22) Condylion Co - Most posterior superior point of condyle |
|
|
Steiner Analysis and Limitations
|
SNA/SNB/ANB, and Incisor to NA/NB Line
Limitations 1) As vertical distance between A, B and Nasion increases, the ANB angle will decrease 2) As Jaws become more protrusive, ANB will increase even if their horizontal relationship is unchanged 3) If Nasion is abnormally positioned anteroposteriorly, size of angle will also be affected. |
|
|
Sassouni Analysis
|
First to emphasize vertical as well as horizontal relationships
- Theorized that in a well-proportioned face, the inclination of SN, Frankfort, Palatal plane, Occlusal plane, and Mandibular plane will converge toward a single point. - If any one plane misses general area of intersection, will stand out. - If they converge closely with high divergence, will contribute to skeletal deep bite - If converge far with low divergence, will have skeletal beep bite |
|
|
Harvold Analysis and Limitations
|
Describes degree of jaw disharmony like in Wits
- Measurements made from posterior wall of glenoid fossa to 3mm thick ANS and to Gnathion - Line also drawn from 3mm thick ANS to Menton to measure lower face height Limitations - Harvold did not account for the fact that as the vertical height decreases, chin will be placed more anteriorly. |
|
|
Wit's Analysis
|
Describes degree of jaw disharmony like in Harvold
- Unlike Harvold, Wit's analysis is influenced by teeth horizontal and vertically - Measures jaw discrepancies with perpendicular from Point A and B to the Functional Occlusal plane drawn along max intercuspation of posterior teeth Limitations - Fails to distinguish skeletal discrepancies vs dental discrepancies - Does not indicate which jaw is at fault if there is a skeletal problem |
|
|
McNamara Analysis and Strengths
|
Uses Frankfort plane and Basion-Nasion line as reference points
1) "Nasion Perpendicular" is drawn from Nasion down perpendicular to Frankfort Plane. Maxilla should be slightly ahead, with Mandible slightly behind 2) Compare Maxilla and Mandibular length using Harvold's approach with mandible positioned in space using ANS-Menton. 3) Upper incisor related to maxilla using line through point A perpendicular to Frankfort. Similar to Steiner, but does not use NA line. 4) Lower incisor is Ricketts analysis, relating lower incisors to A-Pogonion Line. Strengths 1) Relates jaw via Nasion Perpendicular. So anteroposterior differences in jaw relationships are measured along dimension in which they are visualized. Better to use true horizontal line rather than Frankfort, but cephs used to derive data were not taken in NHP. 2) Data is based on well-defined Bolton sample and are highly compatible. |
|
|
Template Analysis
|
First select a reference template according to patient's physical size and developmental age
- Use length of anterior cranial base, SN 1) Cranial base superimposition 2) Maxillary superimposition 3) Mandibular superimposition |
|
|
Roll Pitch and Yaw
|
Roll is sideway rotations along the Transverse Axis
Pitch is frontback rotations along the Anteroposterior Axis Yaw is spin rotation along the Vertical Axis |
|
|
Esthetic Lip positioning
|
Lower Limits
- Upper lip should be slightly forward from it's base at soft tissue point A - Lower lip should be atleast as prominent as chin Upper Limits - Should both be behind E line from tip of nose to Pogonion |
|
|
Limits of Mandibular Expansion
|
Incisors: Up to 2mm or could result in fenestration and recession
- Must be prudent. Incisors tipped labially and still crowded will probably be unstable to more labial tipping. Canines: No expansion is stable Premolars & Molars: Up to 2-3 mm* - Increased risk of fenestration beyond 3mm of tooth movement. |
|
|
Contemporary Extraction Guidelines
|
Less than 4mm arch length discrepancy
- Extraction rarely indicated except for severe incisor protrusion - Try to IPR instead 5-9mm - Both possible - Depend on facial characteristics - Non-exo usually requires transverse expansion of premolars and molars, and molar distalization, which increases treatment time. More than 10mm - Exo almost always required. - Crowding virtually equals amount of tooth mass removed, so no lip changes occur. |
|
|
Incisor retraction and Lip movement
|
As a general rule, lips will move 2/3 the distance of incisors.
- Variable. Thicker lips will respond less to incisor retraction than thin lips. |
|
|
Effects of Reverse Pull Headgear and Ideal candidate
|
1) Forward movement of maxilla largely dependent on patient age. Should begin by 10 latest
2) Forward movement of maxillary teeth relative to maxilla 3) Downward and Backward rotation of mandible due to reciprocal force placed on chin Ideal candidate should have: 1) Retrusive or normal maxillary teeth. Not protrusive. 2) Short or normal anterior vertical dimension. Not long. |
|
|
Class 3 Camouflage and Ideal candidate
|
Can be accomplished by proclining upper incisors and retracting mandibular incisors into an extraction space
- Often fails especially when patient has a large and prominent mandible - Retracting lower anterior teeth makes chin more prominent. Improves occlusion while make jaw discrepancy more obvious. Ideal Candidate 1) Reverse overjet largely due to protrusive mandibular teeth and retrusive maxillary incisors. 2) More maxillary deficiency than mandibular prognathism 3) Short anterior face height so downward and backward rotation of mandible would be favorable both anteroposterioly and vertically. - This combination is rare in European descent, but more frequent in Asians. |
|
|
Major goals of orthodontic treatment
|
Ideal Occlusion
Ideal Facial Esthetics Ideal Stability of results |
|
|
General Sequence for Cleft Patients
|
2-4 wks - Lip closure with possible infant orthopedics to bring back premaxilla
1 - 1.5 yrs - Palate closure 7-9 yrs - Scars from surgery results in anterior and lateral crossbite - Correct incisor position and prepare patient for alveolar bone graft during early mixed dentition. - Objective is to get a tooth to erupt in graft site to bring with it new bone. So graft must be done prior to eruption of lateral, or if lateral is missing, the canine. Adolescence - Comprehensive orthodontics with possible lip and nose revision Late adolescence - Orthognathic surgery - Then definitive restorative work can be carried out to replace missing teeth - Pharyngeal flap is needed after maxillary advancement to control leakage of air through the nose. |
|
|
Active Stabilization
|
Produced by metabolic activity in the PDL to resist small unbalanced forces. Up to 5-10 grams of force at most.
|
|
|
Orthodontic Force Duration Classification
|
Continuous - Force maintained at a good fraction of the original force between patient visits when appliance is reactivated
Interrupted - Force levels decline to zero between activations Intermittent - Force levels decline abruptly to zero intermittently when appliance is removed by patient and returns later. All patient removable appliances such as elastics, headgears, etc. |
|
|
Use of Heavy Forces
|
Heavy continuous force must be avoided
Heavy intermittent forces are less efficient, but can be clinically acceptable if there is a period of repair and regeneration before the next activation Should not be reactivated more frequently than 3 week cycles - Undermining resorption requires 1-2wks, then healing time is necessary - 4-6wk appointment cycle is more typical |
|
|
Drugs that affect orthodontic treatment
|
Prostaglandins and Relaxin could be used to increase tooth movement. Studies are underway, but most drugs currently inhibit tooth movement as a side effect.
PgE Inhibitors 1) Corticosteroids inhibits formation of Arachidonic acid 2) NSAIDs inhibit conversion of Arachidonic acid to Prostaglandins 3) Many other classes of drugs - Tricyclic antidepressants: Doxepin, Amitriptyline, Imipramine - Antiarrhythmic agents: Procaine - Antimalarial: Quinine, Quinidine, Chloroquine - Methylxanthines for Asthma Bisphosphonates - Elective extractions for Ortho should be avoided - Most of the drug is on the surface, so ortho treatment is possible after a 3 month drug holiday, or if patient switches to Evista, an estrogen analogue at least temporarily. |
|
|
Corticotomy accelerated intrusion
|
Posterior Intrusion via TADs are about 1mm a month, but no evidence supports more claim or more rapid intrusion via corticotomies.
|
|
|
Stationary Anchorage
|
Pit tipping against bodily movement.
|
|
|
Ortho Allergy
|
1) Latex in Gloves or Elastics.
2) Nickel in Bands, Brackets, or Wires. - Can use Titanium brackets and tubes with Beta-Titanium wires. |
|
|
Moving intruded teeth
|
Resorption is less likely when Calcium Hydroxide is maintained while tooth is being moved.
- Definitive endo should be completed after ortho. |
|
|
Effects of Ortho on Tooth Structure
|
Roots are remodeled as well as bone
- If defects go into dentin, cementum will be deposited over it - If defects coalesce at the apex, peninsulas of root structure will resorbe and net loss of root length occurs - So Permanent loss of tooth structure related to ortho occurs at the Apex |
|
|
Types of Root resorption
|
Moderate Generalized
- Most teeth show some loss of length, and is correlated with treatment time - Up to 1-2 mm is normal Severe Generalized Resorption - Rare and Etiology is unknown - If there is evidence of root resorption or abnormal root anatomy before ortho treatment, then patient is at much higher risk of more resorption Severe Localized Resorption - Often caused by excessive heavy prolonged force, with prolonged treatment - Some individuals are simply more susceptible to resorption, may be related to genetics. - Risk is much higher in Maxillary Incisors, and in teeth forced against the Cortical Plate* |
|
|
Force prescription for Facemask
|
Restraining Growth
- 500-1000gm of total force. Half each side - Force direction slightly above occlusal plane through Molar center of resistance - At least 12 hrs a day every day early evening to morning - Typically 12 months of treatment. Stimulating growth - Should start at 10yrs latest - 500-1000gm of force total. Half each side - 4-5mm forward displacement is usually maximum without surgical intervention due to soft tissue matrix. |
|
|
Controlling Mandibular Growth
|
Restraining Mandibular Growth
- Currently no effective method in controlling excessive mandibular growth - Chin cup needs to be worn for much longer periods of time and is very uncomfortable - Chin cup also loads only a small area of the condyle, so it's more likely to rotate mandible downward. Can't be used on long face types Augmentation of Growth - Controversial. Growth is generally accelerated, but many studies show that ultimate sizes end up being the same - Herbst appliance is generally most effective in altering jaw growth due to the full time action - Amount of dental vs skeletal change is unpredictable - If patient uses musculature to posture mandible forward, you get more skeletal and less dental movement. If they rely on the Herbst passively, you will see more dental movement. |
|
|
Springback
|
The amount that a wire will return towards it's original shape after being bent past the Yield point
|
|
|
Ortho Bracket Size Measurements and Conversion
|
Measured in thousands of an Inch in the US. Mils can be used to remove decimal simplify. 0.016 = 16Mils
Measured in mm in Europe and rest of the world Conversion - Divide Mils by 4 and move decimal to Left - 16Mils = 0.4mm |
|
|
Surface Quality of Wires
|
Stainless Steel is smoothest with lowest friction
NiTi has most rough surface but medium friction TMA or Beta-Titanium has highest friction due to surface reactivity of titanium - Enough surface chemistry to cold weld the wire to bracket |
|
|
Ratio of PDL for significant differential in tooth movement
|
Atleast 2-1 without sliding
Atleast 4-1 with sliding - Sliding mechanics generally doubles the resistance |
|
|
Cantilever Spring applications, advantages and disadvantage
|
Used most frequently to bring down severely displaced or impacted teeth
Advantage - Long range of action with minimal decrease in force as tooth moves - Excellent control of force magnitude Disadvantage - Do not fail safely. If they are distorted, can produce significant movement in the wrong direction. - Moment on unerupted tooth rotates crown lingually as tooth is brought toward the occlusal plane |
|
|
Functional Appliance Categories
|
Passive Tooth-Borne
- Bionator, always removable - Twin Block, usually removable but can be fixed - Herbst usually fixed but can be removable Active Tooth-Borne - Modification of Bionators or Activators to include expansion screws or springs to move teeth - Produces mostly camouflage tooth movement and is no longer used much Tissue-Borne - Frankel is only tissue borne functional appliance - Most of appliance is in vestibule - Expands arches and stimulates jaw growth Hybrid - Made of different components to fit a specific need - Often used to treat jaw asymmetry |
|
|
Clear Aligner Applicability
|
Performs well:
- Mild-Moderate crowding with IPR or Expansion - Absolute intrusion of 1-2 teeth - Posterior expansion - Close mild-moderate spacing - Tip molar distally Does not perform well - Large expansion for blocked out teeth - High Canines - Extrusion - Leveling - Severe rotation, especially round teeth - Translation of molars - Molar uprighting |
|
|
How to manage Debonding White spots
|
1) Give it 6 months to remineralize. Avoid products with high Fluoride because it will arrest remineralization. Can consider Recaldent or MI Paste Plus
2) Bleaching to blend in the white spots 3) Micro-abrasion using pumice-HCL slurry followed by Recaldent or MI Paste Plus 4) Ultimate is Veneers or Crowns. Can manage first step. Should involve restorative dentist beyond that. |
|
|
Problems with Plastic Brackets
|
1) Staining and discoloration, esp in patients who smoke and drink
2) Poor dimensional stability. No possible to have precise slots with all the straight wire features 3) Plastics are rough and have high friction |
|
|
Problems with Ceramic Brackets
|
1) Loss of part of brackets during wire change or eating
2) Cracking of bracket when Torqued so ceramic brackets have to be bulkier to resist fraction 3) Can wear teeth 4) Also difficult to slide |
|
|
TAD Stability
|
Primary stability is maximal immediately after placement and tapers off as bone remodeling takes place
Secondary stability increases over time Overall stability decreases for the first 2 weeks and then reaches level greater than primary stability at 6 weeks |
|
|
Pitch of Screw Threads
|
Most of a screw's resistance comes from contact with cortical bone
- Tighter pitch gives better primary stability - Denser the bone, closer the threads should be |
|
|
Length of Screw
|
Short screws generally preform as well as long ones
- Ranges from 5-12mm. Generally between 6-8mm. - Can use long screw that passes all the way through to cortical bone on other side. Invasive. |
|
|
Diameter of screw
|
Ranges from 1.3mm to 2mm
- Below 1.3mm shows drop in success rate - Primary stability increases with Diameter size - Proximity is not a major factor in long term stability, and penetration of PDL does not lead to Ankylosis |
|
|
Taper of Screw
|
Greater microdamage to cortical bone with conical screws that are wider at the neck than cylindrical screws
- Conic screws increase primary stability but may affect secondary stability due to damage |
|
|
Form of Screw Tip
|
All mini-screws are self-tapping
- Thread Forming compresses bone around thread as the screw advances. Better for alveolar bone - Thread Cutting has cutting flutes at tip, and performs better on dense bone such as Mandibular Ramus, Buccal Shelf, Palate, and Zygomatic Butress |
|
|
Surface of Threaded Screw
|
Some studies show that roughened surface increases primary stability
Overall Clinical Stability is not affected by surface characteristics |
|
|
Miniplates Characteristics and Advantages
|
Usually placed at base of Zygomatic Arch or Mandible
- Ideal location for connector is at Junction of Fixed gingival tissue and Loose mucosa - Three screws is better than 2, but nothing additional is gained with 4 - Failure rate is increased in children generally before age 11 due to lack of bone maturity Advantages - Can tolerate more force - Has Locking mechanism to move attachment away from connector. Screw can also have this, but extension will create a moment to loosen the screw - Far above Apices of teeth so won't become a barrier to moving teeth mesial or distally |
|
|
Expansion Considerations
|
Early intervention is indicated if there is a shift or severe constriction
During early mixed dentition Should use expansion lingual arch - *Heavy RPE forces in primary or early mixed dentition will cause distortion of nose |
|
|
Treatments for Moderate posterior cross bite
|
1) Lateral Shift caused by interferences from primary canines or molars
- Equilibration of teeth to prevent shift 2) Expansion of constricted maxilla - W Arch or Quad Helix, activated 4-6mm wider than passive width - Expansion at 1mm each side, 2mm total per month till overcorrection. Takes about 2-3 months and retained for 3 months. - Quad helix is good for preventing Thumb suction. - Warn parents of imprints on tongue that can remain up to a year after. 3) Unilateral Crossbite - Different length arms on W-arch or quad helix - Cross elastics can reposition. Use latex elastic with 5mm lumen generating 170grams of force. |
|
|
Treatments for Anterior crossbite
|
Treat the arch that is causing the crossbite
- Protrusive and spaced lowers or Retrusive and crowded uppers If bodily movement and rotation is needed, use Banded and bonded fixed appliances If there is poor compliance, use Fixed maxillary lingual arch with fingersprings If good compliance, can use removable appliance - Maxillary with finger springs - Mandibular with labial bow |
|
|
Treatment for Open bite
|
First make sure patient wants to stop
1) Counseling to discuss and monitor habit for mature patient 2) Reminder therapy using waterproof bandaid or quad helix 3) Reward system 4) Elastic Bandage around elbows. Helping hand, not a punishment. 5) Appliance therapy - Make sure child understands it is a "helping hand" rather than punishment - Crib should be left in place for 6 months |
|
|
Ankylosed Primary teeth
|
Should be maintained till interference with eruption or drifting of other teeth begins to occur
If there is no successor, should still extract and not use space maintainer to allow other teeth to erupt in that area and bring bone. |
|
|
Tanaka and Johnston Prediction
|
Like the Moyers', also uses lower incisors
1/2 the width of four lower incisors +11mm = Width of Upper canines and premolars in one quadrant +10.5mm = Width of Lower canines and premolars in one quadrant |
|
|
Space Maintainer
|
Band and Loop
- Used for only 1 missing tooth. - Can be banded to primary second or permanent first molar - Use a pair of band and loop if permanent incisors have not erupted - 18 month survival Partial Denture - Can be used when there are multiple missing teeth - Good for esthetics Distal shoe - Early loss of primary second molar - Should be banded instead of soldered to SSC for easy removal - Guide plane should extend into alveolar process and located 1mm below mesial marginal ridge Lingual Arch - Permanent incisors must have erupted - Should have ideal arch form, not contoured to malpositioned teeth - Should rest on Cingula of incisors 1-1.5mm off the soft tissue - Average 24 month survival time - Can use upper lingual arch or if bite is deep, use Nance TPA - Used when one side is intact and other side have more than 1 missing tooth. |
|
|
Minor Space regaining
|
Up to 3mm of space can be regained with simple appliances
1) Maxillary - Usually easier due to palate and head gears - Mostly due to forward tipping and mesiolingual rotation, but can be bodily - Fixed maintaner will be needed after Tipping: Removable appliance with fingerspring activated 2mm to get 1mm movement per month with spontaneous de-rotation Bodily: Fixed appliance with coil spring on segmental archwire, modified nance on primary first molars. 2) Mandibular - Harder than maxillary, and compliance is poor Unilateral: Coil spring with segmental archwire and Lingual arch Bilateral: Lip bumper or Adjustable lingual arch. Both will case forward movement of incisors |
|
|
Incisor Liability
|
Maxilla - 7mm
Mandible - 6mm Some crowding during mixed dentition is expected - Less than 2mm crowding can resolve spontaneously If it is a problem, can disk primary canines to make room. No IPR on permanent teeth should be done |
|
|
Taking advantage of lower molar shift
|
Can use lingual arch to hold back molars and use Leeway space to correct anterior crowding
- Will result in Molar class 2 that needs future correction. If parents insist on doing something earlier - Place lingual arch - Extract primary canines and disk to reduce width of primary molars - Then disk primary second molars to allow first premolars to erupt |
|
|
Straight Lower anterior teeth
|
A child with straight lower incisor segment without anterior arch curvature
- Extraction of primary canines will result in spacing or maintenance of same arch form Tipping spontaneously corrects when there is space. Rotated incisors do not self correct. - Correction of any rotations will still require fixed appliances. |
|
|
Treatment for trauma
|
Most injuries
- Reposition with finger position and stabilize for 7-10 days with light wire - If fractured alveolus, use Heavy wire stabilization for 6 weeks - Can use ortho to move teeth with light force. Must inform possibility of vitality loss * Prior to moving traumatized teeth, take multiple radiographs or a small field of view CBCT 2-3wks, 6-8wks, and 1 year. Intrusion - If under 12 years with open apex, allow the tooth to re-erupt and monitored. - If apex closed with less than 6mm intrusion, re-erupt but will probably be non-vital - More than 6mm should be surgically repositioned Extrusion - If not immediately repositioned, intrusion will cause loss of attachment and vitality - Should reduce tooth and restore Unrestorable injury - Root burial to maintain alveolus |
|
|
Transplantation
|
Best done with tooth has 2/3 to 3/4 root formation
- Decision must be made during mixed dentition - High success rate - Replace Maxillary anterior tooth with a maxillary premolar - Replace missing first molars with 3rd molars |
|
|
Serial Extraction Steps
|
1) Extract primary canines and allow incisors to align. May develop deep bite.
2) When there is 1/2 to 2/3 of root formation on first premolar, extract D's 3) Need premolar eruption before canines for extraction. Enucleation if premolar becomes impacted. Alternately, can leave primary canines and just extract D's. Will not get deep bite but will also not alleviate anterior crowding. |
|
|
Herbst Uses
|
Recommended for early permanent dentition to maximize mandibular protrusion
- Use in mixed dentition will result in more dental change Produces maxillary posterior intrusion, so use in patients with normal or slightly long anterior face height |
|
|
Mara uses
|
Affects mandible less than with Herbst or Twin block
Can tip teeth, and exerts a protrusive effect on mandibular dentition |
|
|
Early class 2 treatment
|
- Skeletal changes are eliminated by subsequent growth
- Does not reduce future need for extractions or surgery - May provide some psychosocial effects for a child being teased or is concerned about their appearance |