![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
189 Cards in this Set
- Front
- Back
|
FEV1 less than 40% of predicted = ???? |
FEV1 greater 80% of predicted= normal
FEV1 60% to 79% of predicted = Mild obstruction
FEV1 40% to 59% of predicted = Moderate obstruction
FEV1 less than 40% of predicted = Severe obstruction |
|
|
FEV1 40% to 59% of predicted = ??? |
FEV1 greater 80% of predicted= normal
FEV1 60% to 79% of predicted = Mild obstruction
FEV1 40% to 59% of predicted = Moderate obstruction
FEV1 less than 40% of predicted = Severe obstruction |
|
|
FEV1 greater 80% of predicted=??? |
FEV1 greater 80% of predicted= normal
FEV1 60% to 79% of predicted = Mild obstruction
FEV1 40% to 59% of predicted = Moderate obstruction
FEV1 less than 40% of predicted = Severe obstruction |
|
|
FEV1 60% to 79% of predicted = ????? |
FEV1 greater 80% of predicted= normal
FEV1 60% to 79% of predicted = Mild obstruction
FEV1 40% to 59% of predicted = Moderate obstruction
FEV1 less than 40% of predicted = Severe obstruction |
|
|
acute reversible airway obstruction... smooth muscle hyper responsiveness |
asthma |
|
|
asthma classification --> mild intermittent |
- Day: symptoms a twice week or less - Brief symptoms (from a few hours to a few days) - Night: symptoms twice a month or less - No symptoms and normal lung function between asthma "attacks” - Spirometry results are > 80% of normal |
|
|
asthma classification --> mild persistent |
- Day: symptoms more than twice a week - Night: symptoms are more than twice a month - Symptoms may affect activity and limit exercise tolerance - Spirometry results are > 80% of normal |
|
|
asthma classification --> moderate persistent |
- Day: symptoms occur every day - Daily use of short acting inhaler - Night: symptoms are more than once a week - Worsening symptoms that affect activity and limit exercise tolerance - Spirometry results are between 60% and 80% of normal |
|
|
asthma classification --> severe persistent |
- Day: symptoms are continual every day - Night: symptoms are frequent > 4 times/month - Spirometry results are 60% or less of normal |
|
|
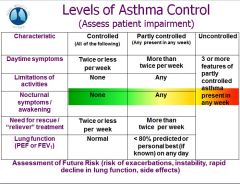
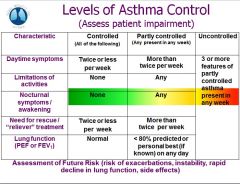
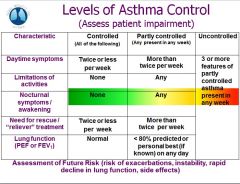
levels of asthma control - controlled |
|
|
|
levels of asthma control - partly controlled |
|
|
|
levels of asthma control - uncontrolled |
|
|
|
which abx do you avoid with asthmatic patients? |
Avoid clarithromycin and erythromycin and azole antifungals with theophylline
--> Azithromycin okay |
|
|
which abx are good for asthmatics? |
Avoid clarithromycin and erythromycin and azole antifungals with theophylline
--> Azithromycin okay |
|
|
what is the analgesic of choice for asthamtics |
Avoid use of aspirin and NSAIDS in sensitive patients
-–> Acetaminophen analgesic of choice for those patients |
|
|
how to manage acute asthma attack |
- Administer short acting β2 agonists - Establish and maintain a patent airway - Administer oxygen 6-10 liters via face mask, nasal hood or cannula.
If symptoms worsen --–> Administer epinephrine subcutaneously (1:1,000 solution, 0.01 milligram/ kilogram of body weight to a maximum dose of 0.3 mg). |
|
|
if acute asthma attack worsens.... |
- Administer short acting β2 agonists - Establish and maintain a patent airway - Administer oxygen 6-10 liters via face mask, nasal hood or cannula.
If symptoms worsen --–> Administer epinephrine subcutaneously (1:1,000 solution, 0.01 milligram/ kilogram of body weight to a maximum dose of 0.3 mg). |
|
|
Oral Health Changes in Individuals with Asthma |
Prolonged use of β2 agonists inhalers and anticholenergics - Increased rate of caries development - Children with asthma have the highest caries risk - Sugar containing medications
Reduced salivary flow due to inhaler use, - Dry mouth associated with albuterol use. Increased levels of gingivitis or gum disease. |
|
|
inhaled corticosteroids |
increased risk of candidiasis from steroids in aerosols |
|
|
General Oral Health Care Instructions for asthmatics |
Prescribe fluoride supplements for all asthmatic patient on β2 agonists/ anticholenergics
Instruct patients to rinse their mouths after using a steroid inhaler –Prevention of fungal infections –Monitor and treat as needed
Reinforce oral hygiene instructions to help minimize gingivitis |
|
|
Chronic obstructive pulmonary disease (COPD) |
Slowly progressive disease
Gradual irreversible loss of lung function
Includes -Chronic obstructive bronchitis -Emphysema, -Combinations of both All have three main symptoms -Coughing -Breathlessness -Wheezing |
|
|
mucus and inflammation |
bronchitis |
|
|
loss of elasticity + collapsed airways |
emphysema |
|
|
Clinical Features of COPD Patient
|
Mild COPD
Moderate COPD
Severe COPD -Cyanosis, peripheral edema, and polycythemia in advanced disease |
|
|
pink puffer` |
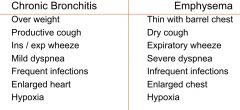
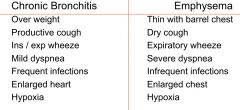
emphysema --> CO2 retention,... no cyanosis... pursed lip breathing - increased mucus, barrel chest - no real inspiratory symptoms... but expiratory wheeze |
|
|
blue bloater |
bronchitis
- color cyanotic - recurrent cough + sputum - hypoxia.. hypercapnia - use of accessory muscles to breathe - overweight... heavy smokers.. lot of infections
INSPIRATORY AND EXPIRATORY SYMPTOMS
|
|
|
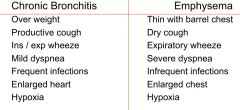
bronchitis vs emphysema |
|
|
|
bronchitis |
|
|
|
emphysema |
|
|
|
which analagesics would you avoid for asthmatics? |
Avoid use of aspirin and NSAIDS in sensitive patients
-–> Acetaminophen analgesic of choice for those patients |
|
|
Conditions that Increase Risk of Transmission to TB Disease
|
• Diabetes mellitus |
|
|
strongest risk factor for progression to TB disease |
• Diabetes mellitus |
|
|
most common way of testing for TB |
mantoux skin test --> does NOT distinguish between LTBI and TBD |
|
|
Reading the Tuberculin Skin Test |
Read reaction 48-72 hours after injection
Measure only induration
Record reaction in millimeters |
|
|
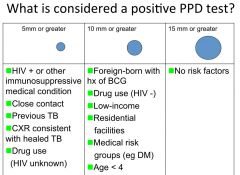
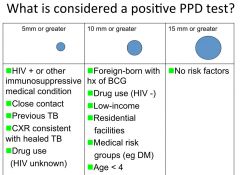
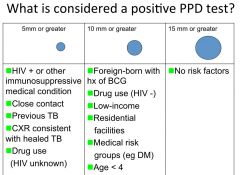
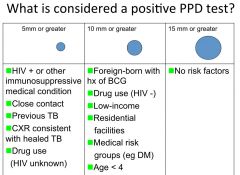
whats a positive PPD test? |
|
|
|
positive PPD test for someone with HIV |
|
|
|
positive PPD test for someone with no risk factors |
|
|
|
positive PPD test for low income drug user |
|
|
|
how do u confirm TB dx? |
use a culture |
|
|
who is infectious for TB? |
active symptoms of TB --> coughing
sputum positive for AFB & : - not receiving therapy - on therapy for < 3 weeks - poor clinical response to therapy (still have systemic symptoms) |
|
|
medical management for active TB disease |
4 drugs for 4 months in initial regimen - Isoniazid (INH) - Rifampin (RIH) - Pyrazinamide (PZA) - Ethambutol (EMB) or Streptomycin (SM)
2 Drugs for 4-18 months - Isoniazid - Rifampin |
|
|
medical management for active TB - 1st 4 drugs |
4 drugs for 4 months in initial regimen - Isoniazid (INH) - Rifampin (RIH) - Pyrazinamide (PZA) - Ethambutol (EMB) or Streptomycin (SM)
2 Drugs for 4-18 months - Isoniazid - Rifampin |
|
|
medical management for active TB - final 2 drugs |
4 drugs for 4 months in initial regimen - Isoniazid (INH) - Rifampin (RIH) - Pyrazinamide (PZA) - Ethambutol (EMB) or Streptomycin (SM)
2 Drugs for 4-18 months - Isoniazid - Rifampin |
|
|
how is infecticity for TB checked |
checked with 3 consecutive negative sputums |
|
|
preventative therapy for latent TB infection |
- ALL pts with positive PPD should be treated !!!!!! - prevent conversion to active disease with Isoniazid (INH) ----> 6 months for +PPD ----> 9 months for +PPD and +CXR (may add rifampin) ----> 12 months for HIV+ and +PPD ----> 18 months for HIV+ +PPD and +CXR |
|
|
adverse rxns to isoniazid (inh) |
- patients can't drink alcohol - hepatotoxic (check LFTs monthly) - 20% develop hepatititis even without alcohol ---> nausea, vomitting, abdominal pain, dark urine - peripheral neuropathy (INH given with vit B6 to prevent this) |
|
|
are surgical masks protective against TB ? |
NO !!! --> special N95 or N99 fitted respirators required |
|
|
systemic signs suspicious of TB disease |
- persistent productive cough (>3 weeks) - hemoptysis - weight loss or loss of appetite - fever - night sweats - chest pain |
|
|
+PPD / +CXR pt maangement |
verify: - no symptoms of active disease - INH for 6 months - 1 year - history of follow-up negative chest x-ray
treat as normal pt |
|
|
+PPD / -CXR pt maangement |
verify: - no symptoms of active disease
Ask about history of prophylaxis - INH for 6 months - 1 year
treat as normal pt |
|
|
patients taking isoniazid (INH) for Tb... must avoid what |
acetaminophen !!!!! |
|
|
pts taking streptomycin must avoid what ? |
aspirin !!!! |
|
|
what is the main cause of chronic liver disease? |
hep c |
|
|
what hemostatic defects will occur in liver disease? |
- Reduced clotting factors |
|
|
infectious hepatitis |
infectious hepatitis - viral hepatitis - mono - secondary syphilis - TB
non-infectious (chemical) hepatitis - excessive or prolonged use of toxic substances ---> drugs (acetaminophen, ketoconazole, alcohol) |
|
|
noninfectious hepatitis |
infectious hepatitis - viral hepatitis - mono - secondary syphilis - TB
non-infectious (chemical) hepatitis - excessive or prolonged use of toxic substances ---> drugs (acetaminophen, ketoconazole, alcohol) |
|
|
infectivity of hep-c |
cal live outside body for up to 16 hours... and in a syringe for up to 63 days
high viral laods of ~800,000 .. (HIV is ~5,000) |
|
|
HBsAg |
Hep B surface antigen
presence indicates current Hep b infection (either acute or chronic carrier state) |
|
|
presence indicates current Hep b infection (either acute or chronic carrier state) |
HBsAg |
|
|
Hep b anti-Hbs |
presence indicates immunity to Hep B infection (ONLY if Hep surface antigen is negative)
positive if received Hep B vaccine |
|
|
IgM vs IgG |
Igm --> acute... recent
IgG --> disease control / immunity |
|
|
HBeAg |
presence indicates HIGHLY INFECTIVE stage of Hep B |
|
|
presence indicates HIGHLY INFECTIVE stage of Hep B |
HBeAg |
|
|
Anti-HCV |
presence indicates current or past hep c infection
does NOT differentiate between the acute/chronic/resolved infection |
|
|
HCV-RNA |
hep c RNA polymerase chain rxn
--> presence indicates actively replicating hep c virus |
|
|
IgM anti HBc |
IgM anti HBc --> acute infection
IgG anti-Hbc --> immunity |
|
|
IgG anti-Hbc |
IgM anti HBc --> acute infection
IgG anti-Hbc --> immunity |
|
|
clinical significance of hep c viral load |
- confirms active infection - predictor of treatment response - confirm HCV medications are working - dictate treatment duration for some HCV medications
***Does not correlate with disease progression |
|
|
does the hep c iral load correlate with disease progression |
- confirms active infection - predictor of treatment response - confirm HCV medications are working - dictate treatment duration for some HCV medications
***Does not correlate with disease progression |
|
|
does hep c viral load give info about dental tx? |
- confirms active infection - predictor of treatment response - confirm HCV medications are working - dictate treatment duration for some HCV medications
***Does not correlate with disease progression |
|
|
does hep c viral load give info about degree of liver damage? |
- confirms active infection - predictor of treatment response - confirm HCV medications are working - dictate treatment duration for some HCV medications
***Does not correlate with disease progression |
|
|
HCV Tx |
- iterferon + Ribavirin (+/- Protease Inhibitor) for 24-48 weeks
- 2 pegylated interferons FDA-improved - pegasys - PEG-intron
4 ribavirins ( copegus, rebetol, ribasphere, generic ribavirin)
2 protease inhibitors - boceprevir (victrelis) - telaprevir (incivek) |
|
|
4 ribavirins |
- iterferon + Ribavirin (+/- Protease Inhibitor) for 24-48 weeks
- 2 pegylated interferons FDA-improved - pegasys - PEG-intron
4 ribavirins ( copegus, rebetol, ribasphere, generic ribavirin)
2 protease inhibitors - boceprevir (victrelis) - telaprevir (incivek) |
|
|
2 pegylated interferons |
- iterferon + Ribavirin (+/- Protease Inhibitor) for 24-48 weeks
- 2 pegylated interferons FDA-improved - pegasys - PEG-intron
4 ribavirins ( copegus, rebetol, ribasphere, generic ribavirin)
2 protease inhibitors - boceprevir (victrelis) - telaprevir (incivek) |
|
|
hematologic side effects of hep c combination therapy |
- anemia --> fatigue --> risk of MI and other cardiovascular abnormalities
neutropenia --> risk of infection
thrombocytopenia --> risk of bleeding |
|
|
Non-Alcoholic Related Fatty Liver Disease |
- obesity, diabetes, dyslipidemia, metabolic syndrome
medications --> amiodarone, tamoxifen, costicosteoids, HAART, tetracycline, calcium channel blockers
- malaise, fatigue, achy , abdonimaal tenderness, enlarged liver
- elevated liver enzymes, bilirubin, cholesterol, triglycerides
- CAN progress to cirrhosis and end stage liver disease !!!! **** |
|
|
can NARFLD progress to cirohhsis ? |
- obesity, diabetes, dyslipidemia, metabolic syndrome
medications --> amiodarone, tamoxifen, costicosteoids, HAART, tetracycline, calcium channel blockers
- malaise, fatigue, achy , abdonimaal tenderness, enlarged liver
- elevated liver enzymes, bilirubin, cholesterol, triglycerides
- CAN progress to cirrhosis and end stage liver disease !!!! **** |
|
|
cirrhosis |
injury & death of heptocytes --> excessive fibrosis
increased resistance to bloodflow thru liver - portal hypertension
varices to relieve pressure --> esophagus , umbilicus, rectum
ascites
splenomaegaly
encephalopathy
|
|
|
decreased albumin production |
--> decreased oncotic pressure
--> increased hydrostatic pressure |
|
|
major cause of mortality in end stage liver disease |
bacterial infections... because decreased neutrophil activity |
|
|
extra-oral features suggestive of advanced alcohol use |
- attention/ memory deficits - spider angiomas - peripheral edema - ascites - palmar erythema - ecchymoses + petechiea - jaundice - bilateral enlarged patorid gland enlargement |
|
|
- attention/ memory deficits - spider angiomas - peripheral edema - ascites - palmar erythema - ecchymoses + petechiea - jaundice - bilateral enlarged patorid gland enlargement |
extra-oral features suggestive of advanced alcohol use |
|
|
intra-oral features suggestive of advanced liver disease |
- parotid gland involvement - glossitis - angular chelitis - gingival bleeding - intraoral petechiea + ecchymoses - jaundiced mucosa - xerostomia - candida infections - lichen planus (hep c) |
|
|
carriers of viral hepatitis |
NO infection control modifications necessary
cannot refuse care bc of high viral load |
|
|
pt w acute symptomatic hepatitis |
avoid elective care unless patient is clinically recovered |
|
|
medical consult for pt with fibrosis/cirhois of liver |
- CBC w differential - platelet count - INR + PTT - liver function tests |
|
|
what do liver functions tests measure? |
measure biosynthetic function
tests measuring detoxification and excretory fxn = ALT, AST, LDH, alkaline phosphatase, bilirubin, albumin |
|
|
primary liver enzymes |
- AST, ALT, LDH, alkaline phosphatase - present in liver cells - hepatocytes (the enzymes show up in the blood)
--> increase indicates primary liver disease (destruction of liver cells) |
|
|
increase of primary liver enzymes |
- AST, ALT, LDH, alkaline phosphatase - present in liver cells - hepatocytes (the enzymes show up in the blood)
--> increase indicates primary liver disease (destruction of liver cells) |
|
|
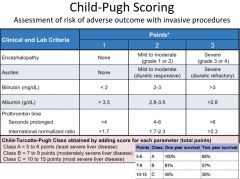
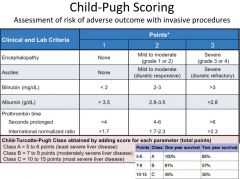
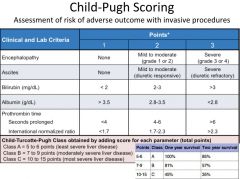
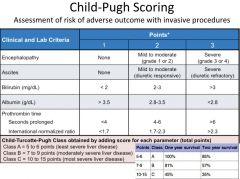
child-pugh scoring |
|
|
|
Child-pugh class a |
|
|
|
child-pugh class B |
|
|
|
when would you decrease dose or avoid drugs with a pt with liver fibrosis/cirrhosis ? |
when one or more is present: - aminotransferase levels are ≥ 4 times normal - serum bilirubin is ≥ 35 µm/1 or 2mg/dl - serum albumin levels are ≤ 35g/l |
|
|
when one or more is present: - aminotransferase levels are ≥ 4 times normal - serum bilirubin is ≥ 35 µm/1 or 2mg/dl - serum albumin levels are ≤ 35g/l |
you decrease dose or avoid drugs with a pt with liver fibrosis/cirrhosis |
|
|
in pts with liver disease... what analgesics would you AVOID? |
AVOID - ibuprofen - aspirin
DECREASE dose - acetaminophenen (always <4g/day in divided doses.... <2g/day in cirrhosis/heavy alcohol users) - codeine (7.5mg q8h) - meperidine |
|
|
in pts with liver disease... what analgesics would you DECREASE DOSE? |
AVOID - ibuprofen - aspirin
DECREASE dose - acetaminophenen (always <4g/day in divided doses.... <2g/day in cirrhosis/heavy alcohol users) - codeine (7.5mg q8h) - meperidine |
|
|
ibuprofen for pts with cirrhosis of liver |
AVOID - ibuprofen - aspirin
DECREASE dose - acetaminophenen (always <4g/day in divided doses.... <2g/day in cirrhosis/heavy alcohol users) - codeine (7.5mg q8h) - meperidine |
|
|
acetaminophen for pts with cirrohis of liver |
AVOID - ibuprofen - aspirin
DECREASE dose - acetaminophenen (always <4g/day in divided doses.... <2g/day in cirrhosis/heavy alcohol users) - codeine (7.5mg q8h) - meperidine |
|
|
in pts with liver disease... what DRUGS would you AVOID? |
AVOID these antifungals - ketoconazole - fluconazole
AVOID these antibiotics - tetracycline - metronidazole - vancomycin - azithromycin/claritromycin/ erythromycin
REDUCED dose - diazepam - barbituates |
|
|
in pts with liver disease... what DRUGS would you LOWER DOSE? |
AVOID these antifungals - ketoconazole - fluconazole
AVOID these antibiotics - tetracycline - metronidazole - vancomycin - azithromycin/claritromycin/ erythromycin
REDUCED dose - diazepam - barbituates |
|
|
azoles in pts with cirrhosis of liver |
AVOID these antifungals - ketoconazole - fluconazole
AVOID these antibiotics - tetracycline - metronidazole - vancomycin - azithromycin/claritromycin/ erythromycin
REDUCED dose - diazepam - barbituates |
|
|
diazepam and barbituates in pts with liver cirrhosis |
AVOID these antifungals - ketoconazole - fluconazole
AVOID these antibiotics - tetracycline - metronidazole - vancomycin - azithromycin/claritromycin/ erythromycin
REDUCED dose - diazepam - barbituates |
|
|
antibiotics for pts with liver cirrhosis |
AVOID these antifungals - ketoconazole - fluconazole
AVOID these antibiotics - tetracycline - metronidazole - vancomycin - azithromycin/claritromycin/ erythromycin
REDUCED dose - diazepam - barbituates
**PENICILLIN / AMOXICILLIN USUALLY SAFE |
|
|
Euthyroid |
Euthyroid - Normal thyroid hormone levels
Hyperthyroidism (thyrotoxicosis) - Increased production of thyroid hormone - Excessive formation and secretion
Hypothyroidism - primary = Decreased production of thyroid hormone - secondary = Decreased secretion due pituitary not secreting TSH |
|
|
Hyperthyroidism (thyrotoxicosis) |
Euthyroid - Normal thyroid hormone levels
Hyperthyroidism (thyrotoxicosis) - Increased production of thyroid hormone - Excessive formation and secretion
Hypothyroidism - primary = Decreased production of thyroid hormone - secondary = Decreased secretion due pituitary not secreting TSH |
|
|
Hypothyroidism |
Euthyroid - Normal thyroid hormone levels
Hyperthyroidism (thyrotoxicosis) - Increased production of thyroid hormone - Excessive formation and secretion
Hypothyroidism - primary = Decreased production of thyroid hormone - secondary = Decreased secretion due pituitary not secreting TSH |
|
|
Lab Findings and Medical Treatment in pt w/ HYPO-throidism |
- INCREASED TSH - DECREASED T3/T4 |
|
|
Lab Findings and Medical Treatment in pt w/ HYPER-throidism |
- DECREASED TSH - INCREASED T3/T4 |
|
|
Causes of Hypothyroidism |
***Autoimmune --> Hashimoto’s disease
- secondary to treatment for hyperthyroidism ----> Surgical removal of gland ---->Radioactive iodine thyroid gland ablation
- External irradiation - Drug-‐induced ---> Lithium, sulfonamides - Pituitary and hypothalamic disease |
|
|
Hypothyroidism |
- In utero-cretinism - Mental slowness, decreased concentration, dementia - constipation |
|
|
myxedema coma |
- Patient with poorly controlled hypothyroidism
Certain factors may suddenly trigger - Drugs - Par1cularly sedatives, narcotics, anesthesia, lithium (Eskalith, Lithobid), and amiodarone - Infections - Trauma - Heart failure - Gastrointestinal bleeding - Hypothermia/Cold - Failing to take thyroid medications as prescribed.
**LIFE-THREATENING EMERGENCY*** |
|
|
symptoms of severea myxedema coma |
- HYPOthermia - HYPOventilation - HYPOxia - HYPOtension
--> seek medical aid, cover to conserve heat, Hydrocortisone 100-300mg, CPR |
|
|
autoimune cause of HYPO-thyroidism |
hashimotos !!!!
autoimmune cause of HYPER-thyroidism is Graves disease |
|
|
autoimmune cause of HYPER-thyroidism |
Graves disease
autoimune cause of HYPO-thyroidism is hashimotos |
|
|
causes of HYPER-thyroidism |
***Autoimmune –Grave’s disease
- Adenoma - Multinodular goiter - Subacute thyroiditis - Iodine-induced hyperthroidism - Excessive pituitary thyroid stimulating hormone (TSH) |
|
|
most COMMON cause of hyperhyroidism |
Grave's disease |
|
|
Grave's disease |
- most frequent cause of hyperthyroidism - toxic diffuse goiter - exophthalmos --> protrusion of the globe of the eye, proptosis and restriction of eye movement |
|
|
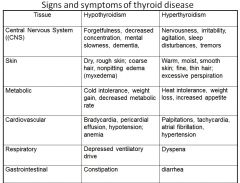
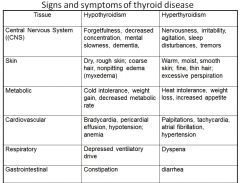
symptoms of HYPER-thyroidism |
- Acceleration of metabolic processes
|
|
|
thyroid storm (thyrotoxic crisis) |
- life- threatening - can be precipitated by ---> stress, infection, vigorous thyroid gland palpation
clinical signs: - elevated body temp; marked tachycardia; extreme restlessness; agitation - tremor; mental confusion - coma + death if not promptly treated |
|
|
clinical signs of thyroid storm |
- life- threatening - can be precipitated by ---> stress, infection, vigorous thyroid gland palpation
clinical signs: - elevated body temp; marked tachycardia; extreme restlessness; agitation - tremor; mental confusion - coma + death if not promptly treated |
|
|
how to treat a hyperthyroid crisis |
• Begins emergency therapy and get immediate medical assistance
|
|
|
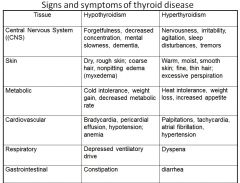
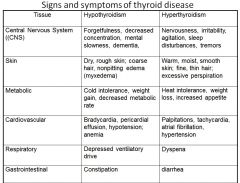
HYPO vs HYPER thyrodism |
|
|
|
cold intolerance / heat intolerance |
|
|
|
respitory signs + symptoms of pts with HYPO vs HYPER thyroidism |
|
|
|
dental management of HYPO-thyroidism |
• Assessment of clinical status
Untreated/poorly treated
• Recognition of myxedema coma |
|
|
avoid for hypo-throidism pts |
• Assessment of clinical status
Untreated/poorly treated
• Recognition of myxedema coma |
|
|
avoid for HYPER-throidism pts |
• Underlying cause and stability
Untreated/poorly treated: Avoid --> Surgical procedures
• Recognition of thyrotoxic crisis |
|
|
adrenal medula produces |
- epinephrine - norepinephrine - dopamine |
|
|
what produces:
- epinephrine - norepinephrine - dopamine |
adrenal medula |
|
|
cortisol |
• Maintain blood pressure and cardiovascular function
|
|
|
commonly prescribed replacement steroid equivalents |
hydrocortisone is EQUAL in potency to cortisol
prednisone is 4x more potent !!!! |
|
|
prednisone vs. hydrocortisone |
hydrocortisone is EQUAL in potency to cortisol
prednisone is 4x more potent !!!! |
|
|
cortisol peaks |
Normal cortisol production
In an adult who is not experiencing stress
During stress
|
|
|
Disorders of Adrenal Cortex |
• Primary Adrenal Cortical Insufficiency
• Secondary Adrenal Insufficiency
• Adrenal Cortical Hyperactivity ----> Pituitary tumor causing chronic glucocorticoid excess – Cushing’s Syndrome ----> Chronic administration of corticosteroids to tx immunological and inflammatory disorders
|
|
|
cushing's syndrome vs disease |
– Cushing’s Disease ----> Pituitary tumor causing chronic glucocorticoid excess
– Cushing’s Syndrome ----> Chronic administration of corticosteroids to tx immunological and inflammatory disorders |
|
|
Addison's disease (primary adrenal insufficiency) |
• Deficiency of aldosterone and cortisol.
*** Higher risk of adrenal crisis if stressed
|
|
|
dental management of HYPER-thyroidism |
• Underlying cause and stability
Untreated/poorly treated: Avoid --> Surgical procedures
• Recognition of thyrotoxic crisis |
|
|
medical management of: Addison's disease (primary adrenal insufficiency) |
• Glucocorticoid replacement
• Mineralocorticoid replacement
|
|
|
secondary adrenal insufficiency |
• Most common from chronic corticosteroid administration
|
|
|
cushing's syndrome (HYPER-adrenalism) |
• A “Cushingoid” patient dislplays
|
|
|
– Weight gain
|
cushing's syndrome (HYPER-adrenalism) |
|
|
problems associated with adverse effects of chronic steroid use |
- immunosuppression - hypertension - osteoporosis - hypergylcemia - muscle weakness - GI ulcers |
|
|
Which patients are at risk for adrenal insufficiency? |
• Addison’s Disease (primary AI)
**(LOW risk for exogenous steroid use .. secondary) |
|
|
Adrenal Crisis |
• More common in primary adrenal insufficiency
• Evolves slowly over a few hours
|
|
|
Tx of Adrenal Crisis |
• STAT 100-‐mg hydrocortisone bolus—and intravenous fluid and electrolyte replacement to restore the blood pressure. • After the initial treatment
|
|
|
dental management for pts taking systemic corticosteroids |
• For diagnostic, all restorative, endodontic and periodontal and minor oral surgery procedures
· For major oral surgery (multiple extractions, impactions, jaw surgery) or sedation |
|
|
supplemental steroids for dental tx? |
NO routine, non-surgival dental procedures warrant supplemental steroids before/during/after the operative period
however... for minor oral surgery (few extractions... biopsy.. single tooth implant, minor perio surgery) --> 25mg of hydrocortisone (5-6mg prednisone) on the day of surgery
--> for moderate , target is 50mg hydrocortison (multiple extractions, bony impactions, mult implants) --> MAJOR (surgery > 1 hour... genanesthesia) = 50-100mg hydrocortisone + 1 day post-op |
|
|
surgery for a pt on steroids |
NO routine, non-surgival dental procedures warrant supplemental steroids before/during/after the operative period
however... for minor oral surgery (few extractions... biopsy.. single tooth implant, minor perio surgery) --> 25mg of hydrocortisone (5-6mg prednisone) on the day of surgery
--> for moderate , target is 50mg hydrocortison (multiple extractions, bony impactions, mult implants) --> MAJOR (surgery > 1 hour... genanesthesia) = 50-100mg hydrocortisone + 1 day post-op |
|
|
major surgery for pt on steroids |
NO routine, non-surgival dental procedures warrant supplemental steroids before/during/after the operative period
however... for minor oral surgery (few extractions... biopsy.. single tooth implant, minor perio surgery) --> 25mg of hydrocortisone (5-6mg prednisone) on the day of surgery
--> for moderate , target is 50mg hydrocortison (multiple extractions, bony impactions, mult implants) --> MAJOR (surgery > 1 hour... genanesthesia) = 50-100mg hydrocortisone + 1 day post-op |
|
|
moderate surgery for pt on steroids |
NO routine, non-surgival dental procedures warrant supplemental steroids before/during/after the operative period
however... for minor oral surgery (few extractions... biopsy.. single tooth implant, minor perio surgery) --> 25mg of hydrocortisone (5-6mg prednisone) on the day of surgery
--> for moderate , target is 50mg hydrocortison (multiple extractions, bony impactions, mult implants) --> MAJOR (surgery > 1 hour... genanesthesia) = 50-100mg hydrocortisone + 1 day post-op |
|
|
acute adrenal crisis |
- position patient semi-reclining with legs elevated - call 911 -administer oxygen and monitor blood pressure - administer 100mg SoluCortef (hydrocortisone) - transport to medical facility |
|
|
mortality rate in individuals with diabetes |
mortality rate is DOUBLED in individuals with diabetes ---> increased risk of cardiovascular mortality |
|
|
why is muscle unable to use glucose in type 1 diabetes? |
type 1 --> muscle unable to use glucose due to low insulin
type 2 --> muscle unable to use glucose due to insulin resistance |
|
|
why is muscle unable to use glucose in type 2 diabetes? |
type 1 --> muscle unable to use glucose due to low insulin
type 2 --> muscle unable to use glucose due to insulin resistance |
|
|
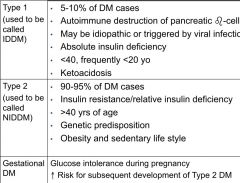
type 1 vs type 2 diabetes |
|
|
|
normal fasting plasma glucose |
normal = < 100 pre-diabetes = between 100 & 125 diabetes = >126 |
|
|
diabetes fasting blood glucose |
normal = < 100 pre-diabetes = between 100 & 125 diabetes = >126 |
|
|
2 hour plasma glucose challenge |
normal: < 126 impaired: betw 140-200 diabetes: > 200 |
|
|
basic levels of glycoslated hemoglobin |
used to determine how well controleld pt is
<6 --> very excellent 9 --> fair >12 --> very poor |
|
|
what does Metformin do? |
it is a biguanide --> enhances liver and muscle insulin sensitivity |
|
|
symptoms of HYEPR-glycemia |
- going to bathroom a lot - very thirsty - feeling tired - feeling weak - blurry vision - feeling hungry (even after a meal) |
|
|
symptoms of HYPO-gylcemia |
- shakiness - dizziness - nervousness - sweating a lot*** - hunger - headache - pale face - clumsiness - confusion - trouble paying attention - tingling around the mouth - passing out (fainting) |
|
|
what drugs does a pt take that could most commonly cause HYPO-glycemia? |
- MOST likely with insulin - more likely with sulfonyureas - uncommon with other meds... esp metformin |
|
|
good glycemic control |
FBS: < 110mg/dl HbA1c: <7% |
|
|
moderate glycemic control |
FBS: < 2000mg/dl HbA1c: 7-8.5% |
|
|
poor glycemic control |
FBS: >200mg/dl HbA1c >8.5% |
|
|
dental management for diabetic pt |
- confirm pt has taken usual insulin dosage or oral hypoglycemic AND eaten normal meal (less critical with metformin)
- avoid scheduling during meal time |
|
|
when might signs of HYPO-glycemis become blunted/absent? |
if a pt is taking beta-blockers !!!
--> diaphoresis (sweating) actually increases |
|
|
best and worse case scenarios of dental management of a diabetic |
BEST = pt took meds and ate... (blood sugar should be close to normal)
WORST = took meds but did NOT eat (blood sugar may drop a LOT)
OK --> pt ate but did NOT take meds
SO-SO --> didnt take meds OR eat |
|
|
if a pt starts experiencing symptoms of hypoglycemia |
- administer 15gms sugar source EVEN IF YOU ARE NOT SURE IT SI HYPOGLYCEMIA !!!!
NEVER GIVE A PT INSULIN !!!!!!!!!!!!!! |
|
|
diabetes and periodontal disease |
periodontal disease is THE MOST PREVALENT oral complication of diabetics |
|
|
how does poor glycemic control affect salivary flow and crevcular fluid? |
DECREASES salivary flow and INCREASES glucose concentration in crevicular fluid |
|
|
diabetes and caries |
- poorly controlled have increased glucose in salivary secretion --> INCREASED root caries
well-controlled have lower intake of carbs --> may have diminished caries rate |
|
|
diabetes and dental pulp |
- GREATER prevalence of periapical lesions in diabetics than in nondiabetics - b/c the dental pulp has limited or NO collateral circulation, it is more prone to infection
in pts with good glycemic control.. --> periapical and other lesions heal as readily as in non-diabetics |
|
|
diabetes and xerostomia |
- 80% of poorly controlled diabetics - decreased parotid flow rates - INCREASE in candidiasis --> especially with dentures --> use azole antifungals with care in pts on TZDs - INCREASED oral burning and taste disturbances |
|
|
what is the most common cause of renal disease? |
DIABETES !!!!
diabetes --> hypertension --> renal failure |
|
|
most common causes of chronic renal failure |
- diabetic nephropathy - nephrosclerosis secondary to HTN |
|
|
co-morbitities of patients with renal disease |
- 100% have HTN - 75 % have diabetes - 60% have coronary arery disease 34% have ischemic heart disease - 25% have congestive heart failure |
|
|
symptoms of renal failure |
ASYMPTOMATIC until about 50% of the nephrons are lost --> then the compensatory mechanisms are overwhelmed |
|
|
symptoms of renal insufficiency |
- headaches - decreased ability to concentrate urine - polyuria --> oliguria - INCREASED BUN and serum creatinine - edema - mild anemia - INCREASED BP - weakness + fatigue - GFR progressively decreases from 90 to 30 ml/min |
|
|
symptoms of end stage renal failure |
- neurological weakness/fatigue & confusion - increased BP - pitting edema; periorbital edema, pericarditis - SOB, depressed cough, thick sputum - ammonia odor to breath; metallic taste, anorexia - withdrawn; depression - anemia; bleeding tendencies - dry flaky skin; pruritis, ecchymosis; purpura |
|
|
laboratory findings in renal disease |
- HYPER-kalemia - acidosis - HYPO-calcemia - HYPER-phosphatemia - HYPER + HYPO - natremia - moderately severe normochromic-normocytic anemia - leukocyte and platelet destruction - coagulopathies |
|
|
what kind of anemia would a pt with renal disease have |
- HYPER-kalemia - acidosis - HYPO-calcemia - HYPER-phosphatemia - HYPER + HYPO - natremia - moderately severe normochromic-normocytic anemia - leukocyte and platelet destruction - coagulopathies |
|
|
azotemia |
- buildup of blood urea nitrogen compounds (mainly urea) - acids accumulate --> metabolic acidosis - ammonia retention |
|
|
normal GFR |
normal = 90-120 mL/min CKD 2 = 60-90 CKD 3 = 30-60 CKD 4 = 15-30 CKD 5 = <15 |
|
|
uremia leads to: |
- HTN - anemia - bleeding problems - electrolyte and fluid imbalance - malnutrition and diarrhea - mental slowness, psychosis, convulsions - altered drug metabolism |
|
|
complications of renal failure |
- DECREASED glomerular perfusion --> activates renin-angiotension system --> increases BP
fluid shifts related to sodium/water shifts - fluid volume overload - mild edema to life-threatening pulmonary edema --> secondary hypertension and CHF |
|
|
oral findings in pts with renal disease |
- pallor of oral mucosa - bad taste/halitosis --> b/c urea in saliva - petechiae and exxhymosis - mucosal / gingival hemorrhang - xerostomia / candidiasis - parotid inflammation and enlargement - NUG and periodontitis - radiographic triad of: loss of lamina dura; ground glass appearance of bone; RL lesions |
|
|
dental findings in pts with renal disease |
tooth erosion --> secondary to vomitting
decreased occlusal/interproximal caries --> increased urea
increased cervical caries --> fluid restrictions and xerostomia |