![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
130 Cards in this Set
- Front
- Back
|
What distinguishes stroke from a TIA? |
TIA < 24h |
|
|
What causes death acutely after a stroke? |
Brain swelling and herniation |
|
|
What is the common origin of emboli from atheromatous plaques that cause strokes? |
Internal carotid artery |
|
|
Which artery of the brain is the commonest site for infarction? |
Middle cerebral or one of its branches
|
|
|
Describe the evolution of histological changes after an ischaemic stroke: |
1. Oedema
2. Neuronal eosinophilia, axonal swelling 3. Inflammatory reaction with neutrophil infiltration and microglial activation 4. Neovascularisation 5. Foamy macrophages (ingest products of degradation of neutrons and myelin), gliosis (glial scar formation) |
|
|
What three mechanisms are proposed to account for neuronal death in ischaemic stroke? |
1. Buildup of lactate from non-oxidative metabolism 2. Buildup of reactive oxygen species and free radicals 3. Excessive influx of Ca2+ (excitotoxicity) |
|
|
Which areas are mostly susceptible to infarction in hypoxia (i.e. drowning)? |
Watershed areas at junctions between arterial territories
|
|
|
What are lacunar infarcts? |
Small areas of infarction in deep areas of the brain (basal ganglia, thalamus, white matter) caused by occlusion of deep penetrating branches. Associated with hypertension and diabetes. Difficult to distinguish from dementia if numerous lacunar infarcts occur. |
|
|
What are the risk factors for venous infarction of the brain? |
Factors increasing blood clotting - dehydration, infection, thrombophilia |
|
|
What is the predominant risk factors for all causes of haemorrhagic stroke? |
Hypertension |
|
|
What is the most common site for haemorrhagic strokes? |
Deep brain matter - might be associated with Charcot-Bouchard aneurysms in relation to hypertension |
|
|
Common causes of cerebral haemorrhage: |
1. Berry aneurysms 2. AV malformations 3. Aβ amyloid depositions in vessel walls (associated with Alzheimer's) 4. Tumours 5. Bleeding disorders |
|
|
What is the most common cause of epidural haemorrhage? |
Trauma (esp fracture of the temporal bone with damage of the middle meningeal artery) |
|
|
What is the classic presentation of epidural haemorrhage? |
Lucid interval directly after trauma; then sudden collapse |
|
|
What is the common cause of subdural haemorrhage? |
1. Trauma 2. Chronic alcoholism (cerebral atrophy + bleeding from liver failure + propensity to minor trauma) 3. Old age 4. Bleeding disorder 5. Perinatal distress |
|
|
What two haemorrhagic events in the brain bear resemblance to rapidly progressing dementia in the elderly?
|
1. Lacunar infarcts 2. Subdural haemorrhage (have the tendency to organise and then re-bleed, mimicking neurodegeneration) |
|
|
What is the common cause of subarachnoid haemorrhage? |
1. Berry aneurysm 2. AV malformation 3. Trauma |
|
|
What is the clinical presentation of subarachnoid haemorrhage? |
Thunderclap headache, vomiting, confusion, signs of meningism |
|
|
What are the differences in terms of blood distribution between epidural, subdural and subarachnoid haemorrhage? |
Epidural - blood doesn't cross suture lines Subdural - blood doesn't cross dural lines (falx, tentorium) Subarachnoid - blood accumulates in sulci and ventricles |
|
|
Name three organisms commonly responsible for bacterial meningitis in the newborns: |
1. Enterobacteriae 2. Group B strep 3. Listeria |
|
|
Name three pathogens commonly responsible for bacterial meningitis in adults? |
Neisseria meningitides Strep pneumo Haemophilus influenzae |
|
|
In prescribing antibiotic therapy against bacterial meningitis in the elderly, you should consider prescribing two agents for added coverage against which organism? What antibiotic will you add? |
Listeria monocytogenes Ampicillin |
|
|
What is the classical triad of signs and symptoms of meningitis? |
1. Neck stiffness 2. Altered GCS 3. Fever |
|
|
Name signs and symptoms of meningitis: |
1. Neck stiffness 2. Altered GCS 3. Fever 4. Headache 5. Photophobia 6. Fits 7. Focal neurology 8. Rash |
|
|
Name two eponymous signs associated with meningitis: |
1. Brudzinsky - forced flexion of neck elicits reflex flexion of hips 2. Kernig - sitting down with thigh flexed at 90 degrees at the hip, subsequent extension of the knee is painful |
|
|
What is the danger of performing an LP in a patient with suspected bacterial meningitis? |
They might have raised ICP; performing an LP may lead to coning |
|
|
What findings would you expect on CSF analysis in a patient with bacterial meningitis?
|
1. Raised opening pressure 2. Cloudy appearance 3. Elevated protein level 4. Low glucose (<50% BG) |
|
|
How are the numbers of RBCs and WBCs in CSF related? Why? |
Sometimes during an LP a blood vessel is burst. To avoid over interpretation of elevated WCC, CSF analysis assumes that for every 500 RBCs there can be 1 WBC (assuming it also comes from the burst vessel). |
|
|
What antibiotic would you use in a suspected case of bacterial meningitis in a 21 year old? |
IV Ceftriaxone |
|
|
What antibiotic would you use in a suspected case of bacterial meningitis in a 67 year old? |
IV Celftriaxone + IV Ampicillin (to cover for Listeria) |
|
|
What adjuvant therapy would you consider administering before the first dose of antibiotics in a patient with bacterial meningitis? |
Steroids; a lot of the damage associated with bacterial meningitis is due to overwhelming host response. There is some evidence for protective role of steroids in prevention of meningitis complications such as deafness. |
|
|
What diseases can be caused by Listeria monocotygenes? |
Febrile gastroenteritis Meningitis Encephalitis |
|
|
Name some possible causes of aseptic meningitis: |
1. Fastidious organism (i.e. TB) 2. Viral meningitis 3. Fungal meningitis 4. Drug-induced meningitis (trimethoprim, NSAIDs) 5. Syphillis 6. Lime disease 7. Partially treated bacterial meningitis (recent antibiotics) |
|
|
Name some of the common pathogens that cause viral meningitis: |
1. Enteroviruses 2. HSV 3. HIV (early presentation) 4. HHV6 5. VZV 6. EBV 7 CMV |
|
|
How would you diagnose viral meningitis? |
CSF PCR |
|
|
How would you treat viral meningitis? |
Supportive treatment |
|
|
What distunguishes meningitis from encephalitis? |
Encephalitis - neurological symptoms, focal neurology, odd behaviour, confusion, abnormal speech |
|
|
What is the common aetiology of encephalitis? |
Viral infection |
|
|
What investigations would you carry out to diagnose viral encephalitis? |
1. CSF PCR 2. Imaging (involvement of temporal lobes suggests HSV) |
|
|
How would you treat a patient with encephalitis? |
Depending on the viral pathogen: - HSV - acyclovir - CMV - gencyclovir - St Louis virus - interferon - HIV - HAART |
|
|
What is the prognosis in viral encephalitis? |
Poor - 40% don't have a favourable outcome |
|
|
What fungi cause meningitis? What is the association? |
Cryptococcus - usually in AIDS |
|
|
How would you distinguish brain abscess of haematogenous and contiguous aetiology? |
Contiguous - usually single lesions Haematogenous - usually multiple lesions |
|
|
What infections can give rise to brain abscesses by contiguous spread? |
Otitis media, mastoiditis, sinusitis, dental infection |
|
|
Symptoms of brain abscess: |
1. Headache - especially in the morning
2. Seizures 3. Focal neurology 4. False localising signs (i.e. 6th nerve palsy - susceptible to stretch) |
|
|
What is the radiological sign of a brain abscess? |
Ring-enhancing lesion |
|
|
What is the differential diagnosis of a ring-enhancing lesion? |
1. Brain abscess 2. Metastasis 3. Glioma 4. Resolving contusion or infarction |
|
|
What is a characteristic sign of TB meningitis on CT? |
Basal meningeal enhancement |
|
|
What is the definition of hydrocephalus? |
Increased volume (and usually pressure) of CSF associated with dilatation of CSF spaces due to congenital or acquired CSF flow obstruction, CSF overproduction or defective CSF absorption |
|
|
What is the usual congenital cause of hydrocephalus? |
Cerebral aqueduct stenosis |
|
|
What acquired conditions may lead to CSF flow obstruction and consequently hydrocephalus? |
1. Tumours and space-occupying lesions 2. Infections 3. Haemorrhage |
|
|
What acquired conditions may lead to CSF overproduction and consequently hydrocephalus? |
Choroid plexus papilloma |
|
|
What is the pathophysiology of 'ex vacuo' hydrocephalus? |
Apparent increase in CSF volume due to brain atrophy and expansion of CSF spaces - raised volume but not pressure |
|
|
Symptoms of hydrocephalus: |
1. Headache - worse in the mornings 2. Lethargy 3. Blurred vision 4. Drop attacks (if sudden change of pressure) |
|
|
When does headache associated with hydrocephalus commonly get worse? |
In the mornings |
|
|
Signs of hydrocephalus: |
1. Increased head circumference 2. Papilloedema 3. Brain herniation |
|
|
What is the most dangerous type of brain herniation? |
Trans-foraminal |
|
|
What medical treatment can be used to alleviate raised ICP? |
Dexamethasone Osmotherapy (mannitol) |
|
|
What is the precursor lesion to glioblastoma? |
Astrocytoma |
|
|
What is the appearance of glioblastoma on MRI? What could it be confused with? |
Ring-enhancing lesion Dx: brain abscess, metastases, cryptococcus |
|
|
What is the typical time scale for presentation of primary glioblastoma? |
Days-weeks |
|
|
Aetiology of glioblastomas: |
1. Primary 2. Progression from low-grade astrocytoma |
|
|
Which genetic conditions predispose to glioblastomas? |
1. Li-Fraumeni syndrome 2. Von Hippel-Lindau syndrome 3. Neurofibromatosis |
|
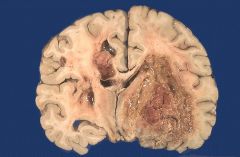
Identify this lesion |
Glioblastoma multiforme (grade IV) |
|
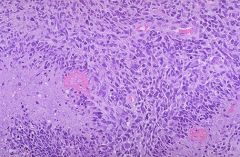
This is a histological slide of a glioblastoma. Describe the characteristic features: |
1. Area of necrosis surrounded by palisading neoplastic astrocytes 2. Glomeruloid vascular proliferation |
|
|
Is glioblastoma amenable to surgical treatment? |
No; combined radio- and chemotherapy is used but usually with poor outcomes |
|
|
Where in the cortex are metastases from other sites likely to appear? |
On the border between grey and white matter in the distribution of middle cerebral artery (MCA) - receives most of the blood flow |
|
|
What is the typical appearance of meningiomas on MRI? |
Enhancing, well-circumscribed, dural lesions |
|
|
What is a common histological appearance of a meningioma? |
Meningothelial cells are arranged in concentric whorls. When calcified, these are called psamomma bodies. |
|
|
What is a psamomma body? |
A concentric area of calcification - common histological feature of a meningioma |
|
|
What is the treatment of choice of a meningioma? |
Surgical resection - can be curative as these are most commonly benign lesions |
|
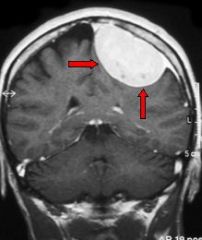
Identify this lesion |
Meningioma |
|
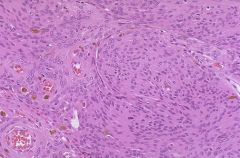
This is a microscopic slide of a meningioma. Identify the characteristic histological features present. |
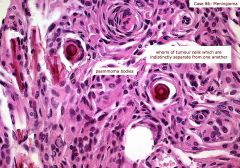
Whorls of meningothelial cells - when calcified, these become known as 'psamomma bodies' |
|

When does this tumour typically present? What is it derived from? |
This is a medulloblastoma - presents in infancy and childhood - derives from neuroectodermal tissue - precursors of cerebellar granule layer cells |
|
|
What is the mode of inheritance of neurofibromatosis? |
Autosomal dominant |
|
|
Which type of neurofibromatosis is more common? |
Type 1 |
|
|
What is the gene product of the defective gene in neurofibromatosis type 1? |
Neurofibromin |
|
|
What is the gene product of the defective gene in neurofibromatosis type 1? |
Merlin |
|
|
Manifestations of neurofibromatosis type 1: |
1. Lisch nodules (iris hamartoma) - brownish-red spots on the iris 2. Neurofibromas (benign skin nodules) 3. Cafe-au-lait spots 4. Optic nerve astrocytomas 5. Pheochromocytomas |
|
|
Lisch spots are associated with ... |
neurofibromatosis type 1 |
|
|
Manifestations of neurofibromatosis type 2: |
1. Bilateral vestibular schwannomas 2. Multiple peripheral schwannomas 3. Meningiomas 4. Ependymomas (tumours arising from the ependymal lining cells of the cerebral ventricles) |
|
|
Is Schwannoma a benign or a malignant neoplasm? |
Benign |
|
|
What are the immediate causes of neuronal death in neurodegenerative disorders? |
1. Excitotoxicity 2. Oxygen free radicals 3. Apoptotic or non-apoptotic cell death |
|
|
How might glial cells perpetuate neurodegeneration? |
By secreting toxic cytokines |
|
|
What is the microscopic pathology of Parkinson's disease? |
Accumulation of alpha-synuclein in Lewy bodies - synucleinopathy. Seen as intracellular eosinophilic inclusions.
|
|
|
Symptoms of Parkinson's disease: |
1. Akinesia/bradykinesia 2. Tremor 3. Postural instability 4. Rigidity 5. Postural hypotension 6. Sleep disturbances |
|
|
What is the classical triad of symptoms in Huntington's disease? |
1. Chorea (dyskinesia) 2. Dementia 3. Psychiatric changes |
|
|
Describe the genetic changes that result in Huntington's disease. |
CAG triple repeat on chromosome 4; exhibits anticipation (number of repeats increases with each subsequent generation; correlates with early manifestation and severity of symptoms) Autosomal dominant mode of inheritance. |
|
|
What is the pathogenesis of Huntington's disease with respect to brain changes? |
Genetic defects lead to toxic gain of function by huntingtin protein, leading to accumulation in the nuclei and neurites of neurons. This leads to atrophy of cortico-striatal loop (head of caudate and cerebral cortex) with net loss of basal ganglia inhibition of thalami-cortical excitation. |
|
|
Describe the molecular pathogenesis of Alzheimer's disease: |
1. Tau is a structural protein which stabilises microtubules - neuronal scaffolding important for transport of nutrients and molecules from the cell body down the elongated axon. In Alzheimer's, misfolded tau becomes insoluble and accumulates in clumps. When this happens, the microtubules disintegrate, collapsing the neurones transport system. 2. Extracellular deposition of beta-A4 peptides results in beta-amyloid plaques deposited in the cortex and blood vessels. |
|
|
What are the initial sites of atrophy in Alzheimer's disease? |
Hippocampus and medial temporal lobe; followed by neocortex. |
|
|
What are some risk factors for Alzheimer's disease? |
1. Old age 2. Down's syndrome 3. ApoE polymorphisms 4. APP ( amyloid precursor protein) mutations - very rare |
|
|
What are the known causes of PrPc → PrPsc transition in prion disease? |
Transition from PrPc (cellular) to PrPsc (scrapie) can be: - idiopathic (sporadic) - facilitated by coding mutation - triggered by exposure to exogenous PrPsc |
|
|
What is the molecular basis of prion disease? |
Misfolded PrPsc is β-pleated sheath rich, protease resistant protein. It accumulates in synaptic and extracellular spaces. This produces neuronal loss, gliosis and characteristic spongiform change. |
|
|
What variants of prion disease are there? |
1. CJD (sporadic) 2. vCJD (variant) 3. Fatal familial insomnia 4. Kuru |
|
|
What are the presenting symptoms of CJD? |
Rapidly progressive dementia - memory loss, personality changes, hallucinations, psychosis |
|
|
Which gene is associated with prion disease? |
PRPN - mutations can cause inherited prion disease; certain polymorphisms increase the risk of sporadic form |
|
|
Which geographical areas show greater prevalence and incidence of MS? |
Colder climates (further from the equator) |
|
|
What is the characteristic finding on CSF analysis in MS? |
Oligoclonal IgG bands |
|
|
How is the diagnosis of MS made in practice? |
Clinical symptoms + neuroimaging backup |
|
|
What findings would you expect to find on MRI in a patient with MS? |
Periventricular plaques (areas of oligodendrocyte loss and reactive gliosis with destruction of axons). |
|
|
What is the pathology of MS? |
Sharply defined, often multiple foci of demyelination with relative preservation of axons, accompanied by inflammation. In later phases, astrocytic gliosis occurs as an attempt to repair the lesion, producing sclerosis. Lesions often separated in space and time. |
|
|
Which sites in the CNS are commonly affected by MS? |
Periventricular white matter Spinal cord Optic nerve |
|
|
What treatments are available to patients with MS? |
No cure; disease-modifying therapies include β-interferon, natalizumab |
|
|
What is a hazardous side effect associated with natalizumab therapy? |
PML - progressive multifocal leukoencephalopathy (opportunistic infection) |
|
|
How do axons get damaged in MS? |
Hypothesis: demyelination leads to redistribution of sodium channels from nodes of Ranvier to the whole surface area of the axon. This increases risk of overwhelming calcium entry and toxicity. |
|
|
What are some of the characteristic symptoms of MS? |
Optic neuritis (sudden loss of vision) Internuclear opthalmoplegia Nystagmus Hemiparesis Intention tremor Scanning speech Bladder/bowel incontinence |
|
|
What pharmaceutical agent can be used to treat acute flare-ups of MS? |
Steroids - reduce duration of a flare-up but do not improve later disability |
|
|
What is a cerebral contusion? |
A bruise in the brain tissue - multiple microhaemorrhages, usually caused by trauma. |
|
|
Where is the lesion localised in a: a) coup b) contre-coup injury? |
a) coup - injury localised on the same side as the area of impact b) contre-coup - injury on the opposite side of the impact |
|
|
What is the life-threatening complication of a cerebral contusion? |
Rise in ICP and herniation |
|
|
What is the typical macroscopic appearance of old cerebral contusions? |
Yellow-golden discolouration (due to residual haemosiderin) with varying degree of cavitation |
|
|
What is the difference between cerebral contusion and laceration? |
Contusion - blunt force, i.e. blow to the head/acceleration/deceleration. Pia-arachnoid membranes not torn. Laceration - tissue of the brain is mechanically cut or torn with pie-arachnoid membranes torn over the site of injury |
|
|
How can you classify brain damage associated with traumatic injury? |
Primary - focal (contusions, lacerations) - diffuse (diffuse axonal injury) Secondary - intracranial haemorrhage - brain swelling - herniation - infection - infarction |
|
|
What is the usual cause of diffuse axonal injury? |
Traumatic brain injury |
|
|
What is the pathogenesis of diffuse axonal injury? |
Traumatic shearing forces that occur when head is rapidly accelerated or decelerated cause disruption of axons as tissue slides over other tissue. |
|
|
What are the histological characteristics of diffuse axonal injury? |
Swollen axons Axonal retraction bulbs |
|
|
What is the characteristic macroscopic feature of diffuse axonal injury? |
Petechial haemorrhages in certain locations (i.e. corpus callosum) |
|
|
What is the difference between Parkinson's and Lewy body dementia? |
Lewy body dementia: - onset of dementia sooner after onset of parkinsonism - less tremor - more cognitive symptoms: hallucinations, fluctuating cognitive impairment |
|
|
What is the clinical presentation of Guillain-Barre disease? |
Rapid progressive limb weakness that ascends following GI/upper resp infection. |
|
|
What is the most dangerous complication of Guillain-Barre syndrome? |
Paralysis of respiratory muscles |
|
|
What genetic condition is associated with predisposition to development of meningiomas? |
Neurofibromatosis type 2 |
|
|
What cells are meningiomas thought to arise from? |
Arachnoid cap cells of the arachnoid villi |
|
|
What are the site-independent presentations of meningioma? |
Headache Seizures |
|
|
What are the most common sources or brain mets? |
1. Lungs 2. Breasts 3. GI 4. Skin (melanoma) 5. Kidney |
|
|
What do you call a glioblastoma that has spread across the midline of corpus callosum? |
Butterfly glioma
|
|
|
Which chemotherapy agent is used in treatment of glioblastoma? |
Temozolamide |
|
|
What is Duret's haemorrhage? |
Tearing of small parenchymal blood vessels associated with transtentorial herniation, resulting in a bleed into the brainstem. |
|
|
What syndrome is associated with development of bilateral acoustic neuromas (Shwannomas)? |
Neurofibromatosis type 2 |
|
|
What are the common presenting symptoms of vestibular schwannoma? |
Hearing loss and tinnitus on the side of the tumour |