![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
302 Cards in this Set
- Front
- Back
|
P wave |
Atrial Depol |
|
|
QRS Complex |
Ventricular Depol |
|
|
T [ECQ] |
Repolarisation |
|
|
Fluid Compartments in fluid homeostasis? |
Extra cellular fluid (plasma and interstitial fluid) and Intracellular fluid |
|
|
Fluid Movement in capillaries |
Hydostatic (BP) and Osmotic[oncotic] Pressures (proteins - notible albumin) |
|
|
Capillary pressure |
Difference in pressure across the interface between two immiscible fluids |
|
|
Oncotic Pressure |
(osmotic) pressure exerted by proteins [albumin] in a vessel plasma. Pulls water into the circulatory system |
|
|
Define Oedema |
Excessive accumulation of fluid, mainly water, in the tissue spaces of the body. Increase in BP or decrease in oncotic pressure |
|
|
Lymphatics |
Drains ISF from tissue into the venous system (abnormal function of this leads to oedema eg. localised obstruction of lymph flow) |
|
|
What conditions may cause oedema |
Renal problems, DM, Liver, type 1 hypersensitivity |
|
|
How can renal problems cause oedema |
Excessive loss of proteins in urine - decreased oncotic pressure = oedema |
|
|
How can hepatic problems cause oedema |
Reduced production of proteins - decreased oncotic pressure = oedema |
|
|
How can type 1 hypersensitivity cause oedema |
Increased capillary permeability |
|
|
Pitting oedema |
A disease of chronic health caused by raised arterial pressure. Occurs in dependant places - ankles and the scrotum |
|
|
Define: Systolic Pressure, Diastolic Pressure and Pulse Pressure |
S - Ventricular contraction D - Ventricular pressure P - difference between the two |
|
|
Describe short term regulation of blood pressure |
ANS - via reflex baroreceptors Low BP = increased sympathetic action leading to: Increased TPR, Cardiac stroke Volume and HR (acting at the SAN) High BP = the converse. |
|
|
Factors in blood pressure control |
CO, total peripheral resistance, circulatin blood volume, blood viscosity |
|
|
Long term Regulation of Blood Pressure factors |
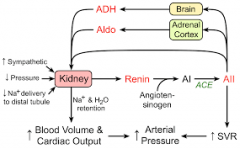
Renin angiotensin system Liver, kidney, lung, PG] Aldosterone from adrenal cortex ADH (AVP) |
|
|
Renin - angiotensin System |
|
|
|
From where is renin excreted |
Kidneys (nephron juxtaglomerular apparatus - monitors low BP) |
|
|
What does renin do? |
Stimulates/Influences angiotensin --> angiotensin I |
|
|
From where is ACE (angiotensin converting enzyme) excreted |
Pulmonary and renal |
|
|
What does ACE do? |
Converts angiotensin I--> angiotensin II |
|
|
What does Angiotensin II do? [also called AVP] |
Constricts vessels to increase arterial pressure and systemic vascular resistance. Stimulates Na reabsorption Stimulates the release of ADH (vasopressin) from pituitary. At adrenal cortex stims release of Aldosterone |
|
|
What does Vasopressin (ADH) do? |
From PG: Increases water retention, Increases peripheral resistance |
|
|
What does Aldosterone do |
From adrenal cortex: Reabsorption of Na, also increases the loss of potassium and H+ in urine. |
|
|
What is hypertension |
140/90mm/Hg sytolic over 140 when diastolic is less than 90mm/Hg. |
|
|
What can cause secondary hypertension |
Renal parenchymal disease, pregnancy, cushings. Drug induced - OCP |
|
|
Risk factors for HTN? |
Age, ethnicity, genetics, obesity, diet, pharmacology, stress, high salt diet, contraceptives, pharmacology e.g. cocaine, NSAIDs, corticosteroids. |
|
|
Non pharmacological management of HTN |
Lifestyle - diet - reduced salt, exercise, limit booze, stop smoking, Assess renal function Aim to lower cholesterol |
|
|
Pharmacological Interventions |
ACE inhibitors -opril Ca Channel Blockers Thiozide Diuretics |
|
|
Complications of HTN |
Cardiac, renal, retinal, cerebral |
|
|
What is Peripheral Artery Disease? |
Atherosclerosis of the larger arteries - stenosis/thrombus/impact of infarcts Symptoms - intermittent claudication, rest pain, critical ischaemia --> ulceration, pain, l.o.sensation, wet/dry gangrene |
|
|
What is AAA |
Abdominal Aortic Aneurysm - may rupture - life threatening |
|
|
What is RAS? |
Renal artery stenosis deminished blood flow to the kidneys = increased renin =HTN |
|
|
WHat is CAS? |
Carotid artery stenosis - atherosclerosis of the carotid arteries. this is a risk factor for TIA and Stroke. |
|
|
Describe briefly the pathogenesis of coronary heart disease |
build up of atherosclerotic plaques leading to narrowing of vessels and potential for infarct - Angina and MI |
|
|
Angina? and describe unstable and stable... |
May be stable or unstable. Stable - pain in chest when there is insufficient blood flow to meet the demands of the heart. - precipitated by exercise or stress Unstable - no precipitating stimulus |
|
|
Symptoms of angina? |
Pain, tightness in chest, heaviness - look for clenching of fist/ hand. Pain may radiate (l. arm/neck/mandible) or be localised |
|
|
Unstable Angina? |
High risk of MI - plaque fissuring and thrombogenic |
|
|
Management of ANGINA |
Drugs - nitrates, beta blockers [-olols], Potassium channel blockers [nicorandil] Surgery - revascularisation - angioplasty/ stents/ CABG |
|
|
Myocardial Infarction |
Same sequelae as angina - the consequence of the infarct depends on site and any cormorbid disease. |
|
|
Diagnosis of an MI |
ECG and troponins [cardiac enzymes] and symptoms |
|
|
Management of MI |
Analgesics - morphine Anti platelets - asp and hep B blockers - eg aterolol Nitrates ACE inhibs Thrombolysis - IV streptokinase |
|
|
Define Atrial Fibrillation |
Most commonly sustained arrythmia - chaotic, uncoordinated and ineffective depol of aorta |
|
|
Types of AF? |
Paroxysmal - transient less than 7 days Persistant - Greater than 7 days. can resolve Perminant - can be resolved/ greater than 1yr |
|
|
Risks of AF |
Most importan RF for stroke as indicated periods of stasis of the blood. |
|
|
Management of AF |
Anti-thrombotic therapy (reduce risk of stroke) - antiplatelets. Cardioversion - pharmacol/electrical |
|
|
Define Diabetes Mellitus |
Chronic raised blood glucose levels |
|
|
What role does the liver have in glucose control? |
The liver is a store of glycogen - which is a polysaccharide of glucose. These stores can be used to rapidly increase the bodies blood glucose levels |
|
|
What role does insulin have in the control of blood glucose? |
Insulin is secreted from the beta islet cells of the pancreas - it has an effect on muscle, EPO, and fat cells to absorb glucose from the blood |
|
|
What role does glucagon have in the control of blood glucose? |
Glucagon is secreted from the alpha cells of the pancreas and acts at many cells and the liver to increase the bodies blood glucose - release stored glucose/gluconeogenesis/ glycogenolysis |
|
|
How does the body raise blood glucose? |
At rest - glucagon At stress - cortisol Pancreas/ adrenal glands / PG - growth hormone |
|
|
What causes type 1 Diabetes? |
Caused by dimished insulin production by the B islet cells in the pancreas - this is usually an autoimmune process - inflammatory destruction |
|
|
What causes type 2 diabetes? |
Cells of the body become resistant to glucose -due to failures in intracellular signalling - this causes initial hyperglycaemia. Later as the B islet cells begin to fail the body stops producing insulin and this will then present as Hypoglycaemia. |
|
|
How might a person with DM1 present? |
Has a rapid clinical onset, reflects the rapidly diminishing B islet cells. Polyuria - Excess urine due to increased glucose in the blood - osmotic diuresis. Polydipsia Fatigue and blurred vision Wt loss Diabetic ketoacidosis |
|
|
Explain diabetic ketoacidosis |
Life threatening, shortage of glucose therefore the body switches burning fatty acids this leads to metabolic acidosis |
|
|
Symptoms of diabetic ketoacidosis |
V unwell, Dehydrations [polyd&polyu], wt loss and muscle wasting, peardrop breath, N&V, abdominal pain. |
|
|
Presentation of DM2 |
V insidious onset, symptoms over months/ years, wt gain, dehydration [polyd, polyu] |
|
|
Diagnosis of DM1 |
1. BG vvv high at first presentation 2. Ketones in urine - signs of DKA |
|
|
Diagnosis of DM2 |
1. random blood glucose - above 8 3. Fasting blood glucose >7mmol 2. Ketones in urine -ve 3. Glucose tolerance - pt fasts overnight then provocation with 75mg of glucose wait 2 hours and if greater than 11 then DM |
|
|
Impact of Chronic Diabetes (main three) |
Small vessel desease, large artery disease, neuropathy. |
|
|
Impact of Chronic diabetes? |
Vascular Disease - metabolic syndrome, Microvascular - CHD, Stroke HTN Heart disease - CHD, autonomic neuropathy and diabetic cardiomyopathy Renal Disease - ATS and HTN Eye Holes - retinopathy, cataracts Neuropathy - distal symmetrical, asymmetrical, pressure palsies, and autonomic Diabetic foot Wound healing - affects neutrophil function Sexual Dysfunction Pregnancy issues Oral - perio, wound healing, infections, sialosis, oral dysaethesia, cranial nerve abnormals, altered saliva quality, ADRs |
|
|
Management of Diabetes |
Education - nutrition, OH, exercise, limit illness or trauma (increases insulin requirements), self monitoring, looking after feets. 2' prevention - smoking cess, foot care, complications - dyslip, HTN, eyes, kidneys Type 1 - insulin needed to survive Type 2 - weight loss is pivotal, and monitoring of HbA1C. diet and exercise then metformin then insulin. Oral HypoG agents - Metformin |
|
|
Impact of Diabetes on orofacial disease |
Perio Altered Taste due to ADRS (metformin) Xerostomia (dehydration) - altered quality/ quantity Sialosis Oral infections - Fungal infections Delayed wound healing |
|
|
What is obesity |
BMI 30-34.9 Kg/M2 |
|
|
Other factors (other than diet and exercise) that may contribute to obesity. |
Genetics, smokers, meds - anticonvulsants, antidepressants, corticosteroids, PM. |
|
|
Consequences of Obesity |
Reduced life expectancy DM2 CHD HTN, HF, Stroke Dyspnoea Obstructive Sleep apnoea Asthma Psychosocial Osteoarthritis Reduced fertility in women GORD Cancers Hypercoaguable state - DVT, stroke Steatohepatitis - cirrhosis Excessive sweating |
|
|
Define Asthma |
Chronic inflammation of the airways, in susceptible individuals. Widespread reversible airway obstruction to a variety of triggers e.g exercise/dust. |
|
|
Define Asthma |
Chronic inflammation of the bronchi and oedema and increased mucous secretion and bronchial hypersensitivity causing sudden and reversible luminal narrowing. |
|
|
Symptoms of Asthma |
Wheezing [diffuse, polyphonic, bilateral and particularly expiratory], SOB, Cough, chest tightness |
|
|
Triggers to Asthma |
Exercise, viral. Iatro - Beta blockers, NSAIDs Environmental Worse at night. Occupational |
|
|
Prevention of Asthma |
1' - breast feeding, decreases the risk 2' avoid allergens, smoking and pollution [triggers] |
|
|
Management of Asthma |
Relievers [B2 agonists, antimuscarinics and theophylline] Controllers/preventors - [corticosteroids, theophylline, leukotriene receptor agonists] B2 Agonists - salbutamol/salmeterol Bronchodilation (relax smooth muscle) BLUE- MDI Antimuscarinics - Ipatropium bromide stimulates paraS to produce acetylcholine GREEN Corticosteroids - ORANGE/BROWN [candida] Cromoglycates - Anti-inflamm, mast cell stabilisation. |
|
|
Peak flow records |
An objective measure of asthma control, easily measured by the patient. |
|
|
Asthma and oral health |
If steroid inhaler - increased likelihood of candida infections. [rinse mouth after and denture hygiene] Risk of precipitating an attack! Prescribing - don't prescribe NSAIDs |
|
|
worris COPD? |
Airflow obstruction that is typically irreversible, progressive and doesn't change markedly. Closely linked with smoking. Airflow obstruction of reduced FEV1 less than 80% of predicted. Caused by damaged airways - inflammation and fibrosis/narrowing or damaged lung parenchyma. inflammation causes alveolar destruction which means the area for gas exchange is reduced |
|
|
Alpha-1 antitrypsin deficiency |
deficiency of A1A - this is a protease inhibitor and protects against enzymes associated with inflammatory cells. deficiency can cause COPD or liver cirrhosis. |
|
|
Diagnosis of COPD - signs and symptoms |
patients older than 35, exertional breathlessness, chronic cough, regular sputum, wheezem ankle oedema, cachexia, depression/anxiety |
|
|
Management of COPD |
1. Limit Complications - smoking and vaccines 2. Control symptoms - medicines [bronchodilators, mucolytics, corticosteroids.] Oxygen, surgery. Oxygen - ambulatory or longterm |
|
|
Pharmacological Management of COPD |
1. Inhaled Bronchodilators [anticholinergic] 2. ChomboBronchodilators [ duovent - ipatropium and feratol or Combivent - ipatropoum and salmeterol 3. Mucolytics |
|
|
Define Seizure |
temporary abnormal activity in brain cells that may involve other parts of the brain. Clinical features include involuntary changes in function, movement, behaviour and awareness. Seizures last for seconds to minutes and are usually self-terminating. |
|
|
Epilepsy |
A group of disorders with different causes characterised by recurring unprovoked seizures. |
|
|
Dermatitis |
Inflammation of skin. 2 types - endogenous (from within) and exogenous (from without). |
|
|
Angina |
A severe pain in the chest that often spreads to the shoulder, arm, neck and mandible, due to an inadequate blood supply to meet the oxygen requirements of the heart (caused by a narrowed lumen of coronary arteries due to atherosclerotic plaque or fissured plaque) |
|
|
Diabetes Mellitus |
A group of disorders with different causes, characterised by a persistently raised blood glucose measurement. |
|
|
Multiple Sclerosis |
Inflammatory demyelinating disease of CNS (brain and spinal cord) that is disseminated in time (occur different points in time) and space (lesions occur at different sites). |
|
|
Anaemia |
A reduction in haemoglobin concentration in the blood. Haemoglobin level below the normal for the age, gender and ethnic background of the individual. (normal range Hb- Men : 13.5- 18.0 g/dl, Women: 110.5-15.5 g/dl). |
|
|
Stroke |
A sudden onset of focal neurological symptoms of presumed vascular aetiology lasting for longer than 24 hours. 80% are due to cerebral infarction and ~20% to cerebral haemorrhage. |
|
|
TIA |
A sudden onset of focal neurological symptoms of presumed vascular etiology lasting for less than 24 hours. |
|
|
Crohn's |
A chronic relapsing inflammatory bowel diseases characterised by periods of active inflammation and clinical symptoms interspersed with periods of relative quiescence and relative health. It most commonly affects the colon, but can affect any anatomical site between the lips and anus. |
|
|
Obesity |
The WHO defines obesity as having a BMI of >30 kg/m2. BMI – weight in kg, divided by height in meters, squared. Waist Circumference – central obesity. |
|
|
Parkinson's Disease |
A common neurodegenerative disorder characterised by the degeneration of dopamine producing cells in the substantia nigra in the midbrain, which results in bradykinesia, rigidity, a resting tremor and other clinical features. |
|
|
Maladaptive Behaviour |
An exaggeration of a normal behaviour e.g. consumption of alcohol / dieting and over-eating. Maladaptive causes the individual to suffer. Typically place the individual at a biological disadvantage. |
|
|
Lichen Planus |
Common mucocutaneous disease of unknown cause Peak incidence 30-60 years old Can occur at any age, including childhood. thought to be autoimmune with an initial trigger. |
|
|
Rheumatoid Arthritis |
It is a common autoimmune disease – 1% of population / F > M 3:1 / Clinical symptoms presents mostly in 4th and 5th decades. Complex and poorly understood – genetic predisposition / environmental factors. In which the immune system activated inappropriately resulting in inflammation of synovium – inappropriate proliferation of synovium / joint destruction. Articular and extraarticular manifestations. |
|
|
Coeliac Disease |
“Gluten – sensitive enteropathy”. An inappropriate T-cell-mediated immune response against gluten in a genetically predisposed individuals.1%. Test Ig specigic, bloods, stools, biopsy. |
|
|
COPD |
Chronic obstructive pulmonary disease (COPD) is characterised by airflow obstruction, which typically is progressive, not fully reversible and does not change markedly over several months. Old terms include Chronic Bronchitis and Emphysema. FEV1 70% of expected. |
|
|
Leukaemia |
Two Forms – Acute Leukaemia and Chronic Leukaemia - both may be further subdivided. Result of accumulation of early myeloid or lymphoid precursors in the bone marrow, blood and other tissues. Probably occurs by somatic mutation in a single cell within a population of early progenitor cells May arise de novo or be the terminal event of a pre-existing blood disorder. |
|
|
Atrial Fibrillation |
Is the most common sustained arrhythmia. Is characterised by chaotic, uncoordinated and ineffectual depolarisation of the atria. paroxysmal, persistent, permanent. |
|
|
Ventricular Fibrillation |
An abnormally irregular heart rhythm caused by rapid, uncoordinated fluttering contractions of the ventricles. Ventricular Fibrillation is rapidly fatal – ‘cardiac arrest’ |
|
|
Bisphosphonates |
Bisphosphonates are drugs that reduce bone resorption |
|
|
BRONJ [MRONJ] |
BRONJ is defined as exposed, necrotic bone in the maxilla or mandible that has persisted for more than eight weeks in patients taking bisphosphonates and where there has been no history of radiation therapy to the jaw. |
|
|
Symptoms of BRONJ |
Symptoms include delayed healing following a dental extraction or other oral surgery, pain, soft tissue infection and swelling, numbness, paraesthesia or exposed bone. |
|
|
Melanoma |
Malignancy arising from cutaneous melanocytes |
|
|
Basal Cell Carcinoma |
Also known as a ‘rodent ulcer’ – ‘gnaws away’. Believed to arise from undifferentiated basal keratinocytes. Locally destructive/invasive (slow-growing) – Metastasis is extremely rare |
|
|
Asthma |
Asthma is a chronic condition characterised by: Chronic inflammation of the bronchi with oedema and increased mucus secretion; Bronchial hyper-responsiveness leading to sudden, but reversible luminal narrowing and airways obstruction during an asthma attack. |
|
|
Osteomyeletis |
An infective disease of bone, which results in necrosis of an area of the affected bone |
|
|
Osteoradionecrosis |
Necrosis of bone primarily due to tissue damage caused by irradiation |
|
|
Osteoporosis |
is a systemic skeletal disease characterised by: – - Low bone mass; – Abnormalities of bone architecture: |
|
|
Sjogren's Syndrome |
A chronic autoimmune condition characterised by degeneration of the salivary and lachrymal glands, causing dryness of the mouth and eyes |
|
|
Infective Endocardititis |
Is infection of the endocardium (inner lining of the heart) by bacteria with inflammation that leads to tissue damage and decreased cardiac function particular related to heart valve damage and the physical effects of related infected vegetations. |
|
|
Trigeminal Neuralgia |
A chronic pain condition that affects the trigeminal nerve, which carries sensation from your face to your brain. If you have trigeminal neuralgia, even mild stimulation of your face — such as from brushing your teeth or putting on makeup — may trigger a jolt of excruciating pain. Associated with atherosclerosis - micro compression - local demyelination [sup cerebellar A]/neoplasms/MS. |
|
|
Types of Melanoma |
Malignancy arising from cutaneous melanocytesSuperficial spreading Nodular melanoma Lentigo maligna melanoma Acral lentiginous melanoma |
|
|
Types of BCC |
Nodular BCC Superficial BCC Morpheaform BCC |
|
|
Types of Atrial Fibrillation |
Paroxysmal - Transient episode of AF that self-corrects with reversion to sinus rhythm in <7 days. Persistent - AF lasts >7 days, but treatment can restore sinus rhythm. Permanent - • Sinus rhythm cannot be restored; or • AF has persisted for >1 year if no attempts made to correct to sinus rhythm. |
|
|
Crohn's +oral features and general features. |
A chronic relapsing inflammatory bowel diseases characterised by periods of active inflammation and clinical symptoms interspersed with periods of relative quiescence and relative health. It most commonly affects the colon, but can affect any anatomical site between the lips and anus. Oral features: Long standing lip swelling- sometimes with lip fissures, Ulceration (aphthous or linear), Cobblestone buccal mucosa, Gingival enlargement, Mucosal tags. Features: Abdominal pain, Diarrhoea, Passing blood/slime per rectum, Weight loss, Fever, Tenesmus, Fistulas (abnormal passaged between two hollow organs), Features of malabsorption’s (e.g. Iron –ferritin- Vitamin B12 or Folate). |
|
|
Parkinson's Disease + oral and general features |
A common neurodegenerative disorder characterised by the degeneration of dopamine producing cells in the substantia nigra in the midbrain, which results in bradykinesia, rigidity, a resting tremor and other clinical features. Oral sialorrhoea, burning mouth, antimuscarinics - xerostomia. General bradykinesia, tremor, rigidity -> loss of postural reflect - falling, facial expressions, speech, altered posture, difficulty initiating voluntary movements, freezing when a movement has stopped, micrographia, dementia, depression, psychosis. |
|
|
Maladaptive Behaviour + features of dependency and Oral signs of alcohol abuse |
An exaggeration of a normal behaviour e.g. consumption of alcohol / dieting and over-eating. Maladaptive causes the individual to suffer. Typically place the individual at a biological disadvantage. Features of Dependancy Subjective awareness of a compulsion to use the substance in question e.g. alcohol Increased tolerance, Symptoms of withdrawal Oral signs of OH abuse Angular Cheilitis, Oral candidiasis, Mucosal ulceration, Glossitis with lose of filiform papillae (smooth tongue) Increased risk of oral cancer (especially if tobacco smoker), Dental erosion if vomiting frequently, Abnormal oral sensation, Sialosis – painful enlargement of major salivary glands (usually bilateral parotid). whiskey nose, gin blossom |
|
|
Lichen Planus and Cancer |
Give accurate information - cancer developing in oral lichen planus is rare. If any new oral lesions develop or existing lesions are worsening (in symptoms or appearances) then the patient should seek early professional advice. 2% of erosive lesions turn into cancer in 15yrs. |
|
|
Symptomatic Management of LP |
Avoid Triggers - curry, tomatoes, SLS toothpaste Analgesics - Difflam [benzydiamine HCL-topical anaesthetic and NSAID] Coating Agents - orabase and gelclair Corticosteroids Orbase [contains triamcinolone] Betnesol, Hydrocortisone succinate, MDI Antimicrobials - chlorhex and polyenes/azoles Systemic Corticostedz |
|
|
Functions of the Liver |
1. Processing and storage of nutrients in the gut 2. Bile synthesis and excretion 3. Synthesis of coagulation factors and other proteins (vitamin K dependent coagulation factors and albumin) 4. Infection and immunity (macrophage lineage kupffer cells) 5. Hormone metabolism 6. Vitamin D metabolism 7. Drug metabolism |
|
|
Congenital liver Probs |
hereditary heamochromatosis - Inappropriate deposititon of iron in tissues Wilsons (alpha1 antitrypsin) - copd and cirrhosis |
|
|
Acquired Pathology of the Liver - Biliary Tree |
[Any pathology of the parenchyma will cause 2' damage to the bile ducts and vice versa] Gallstones - jaundice and pain PBC - chronic progressive destruction of the small biliary ducts in the liver - 2' cirrhosis [70% have sjogren's] PSC - Progressive fibrosing inflammation of the bile ducts - cirrhosis [linked with UC] |
|
|
Acquired Pathology of the Liver - parenchyma |
[Any pathology of the parenchyma will cause 2' damage to the bile ducts and vice versa] Hepatitis - acute/chronic - infections, drugs, AI, Errors of metabolism, cryptogenic, cancer Cirrhosis - Diffuse abnormalities of the liver - inapprop fibrosis with abrnormal nodules. Liver Cancer |
|
|
Acquired Pathology of the Liver - Vasculature |
Portal HTN - raised venous pressure in liver caused impaired blood flow through parenchyma - cirrhosis. Right heart failure, portal vein thrombosis, hypercoag state, malignancy. Gastro-oesophogeal Varices - due to HTN. [abnormal dilation/enlargement of vein]. May haemorrhage (slow or fast) Splenomegaly - venous connection between spleen and liver + HTN = enlarged spleen - hypersplenism [destruction of RBCs and platelets through thrombocytopaenia - increased thrombotic state] |
|
|
Chronic Signs that the Liver is knackered? |
Jaundice, Prolonged Bleeding, Hepatorenal problems, Malnutrition, Fluid overload, Ascites, Nails, Palmar erythema, Spider naevi, Hepatic encephalopathy, Altered steroid metabolism. |
|
|
Functions of the Kidneys |
1. blood filtration - 20-30% through glomeruli 2. fluid balance - reabsorb sodium and water. (recovery of ions). also facilitated by ADH (vasopressin) (secreted from pituitary). excretion of H and K ions. 3. excretion of waste products - urea and creatinine. 4. acid base balance - hydrogen and bicarbonate ions 5. Endocrine - erythropoietin and renin and Vitamin D (renal osteodystophy) |
|
|
Signs that the Kidneys are knackered? |
CV disease - CHD/Angina/HFAnaemia, Abnormalities of coagulation, Renal bone disease (renal osteodystrophy), Malnutrition, Tissue Oedema, Immune system, Malignancy, Sexual dysfunction and pregnancy, Mental health, Childhood development |
|
|
Congenital Kidney Issues |
ADPKD- autosomnal domninant polycystic kidney disease Alports |
|
|
Acquired Renal Issues |
Diabetic Nephropathy - common in DM2 HTN Neuropathy Renovascular disease (ATS) - atherosclerosis of renal arteries SLE Infections such as HIV Cancers Nephrotoxic Drugs |
|
|
Define Pharmacokinetics |
Active drugs and/or their active metabolites will accumulate with potentially adverse effects, if in health the liver/kidney contributes to their excretion; and The activity of some drugs is influenced by their degree of protein binding, which can be changed in hepatic/renal impairment. |
|
|
Define Pharmacodynamics |
The sensitivity of the target tissues to specific drugs may be either increased or decreased with potentially adverse effects. |
|
|
Management of Liver Disease |
1. BarriersPatient availability, interns of time and finance. OH might not be a priority. The dentist can improve the patient’s QOL by maintenance of oral healthcare to minimise likelihood of problems. 2. Orofacial Manifestationsdeficiencies in vitb12 and ferritin - anaemia - angular cheilitis, depapillation of the tongue, erythema and pain, oral ulcerations (apthous), candida, burning/abnormal taste, pallor, plummer vinson - dysphag due to oesophageal webs 3. Diet and Oral Health/ smoking and drinking - stop drinking advice. linked to poor control of blood glucose therefore may have to snack frequently - cares risk? Dry mouth? 4. Side effects of therapeutic interventions - e.g. immunosupression and cyclosporin - gingival enlargement 5. Prescribing - effects on metabolism and clearance. hepatotoxins 6. Family - impact on fam - may be carers etc. |
|
|
What is HBa1c |
Haemoglobin becomes glycosylated in presence of glucose; HbA1C gives a measure of glycosylated haemoglobin. This is a good indicator of glycaemic control over last 8- 12 weeks: Health – 20-41mmol/mol / Diabetes good control <59mmol/mol |
|
|
Pathogensis of type I DM |
1. Results in diminished insulin production. Caused by the destruction of β-islet cells in pancreas 2. Usually auto-immune process - Infiltration of lymphocytes. Disease typically manifests once ~90% of β-islet cells destroyed. 3. T-lymphocytes infiltrate β- islet cells;Inflammatory destruction.Auto-antibodies present in most. |
|
|
Obesity and DM? |
Studies suggest that abdominal fat causes fat cells to releases ‘pro-inflammatory’ chemicals, which can make the body less sensitive to the insulin it produces by disrupting the function of insulin responsive cells and their ability to respond to insulin. This is known as insulin resistance - a major trigger for type 2 diabetes. Having excess abdominal fat (i.e. a large waistline) is known as central or abdominal obesity, a particularly high-risk form of obesity The links between obesity and type 2 diabetes are firmly established - without the intervention of a healthy diet and appropriate exercise, obesity can lead to type 2 diabetes over a relatively short period of time. The good news is that reducing your body weight, by even a small amount, can help improve your body's insulin sensitivity and lower your risk of developing cardiovascular and metabolic conditions such as type 2 diabetes, heart disease and types of cancer. According to the NHS, a 5% reduction in body weight followed up by regular moderate intensity |
|
|
What is the difference (histologically) between pemphigus and pemphigoid? |
Pemphigus - intraepidermal blistering disease [type 2- immune destruction of desmosomes] Pemphigoid - sub epidermal blistering disease [type 2] |
|
|
Clinical Features of a Seizure? |
involuntary changes in function, movement, behaviour and awareness.Seizures last for seconds to minutes and are usually self-terminating. |
|
|
Causes of Epilepsy? |
66% unknown causes Genetic/congenital predisposition Acquired illness - Cerebrovascular disease, - Cerebral neoplasm - Alcohol related brain damage - Post traumatic brain damage |
|
|
Classifications of Eplilepsy |
Partial Epileptic Seizure - Temporal PES, Occipital PES Generalised Epileptic Seizure - Grand Mal (tonic-clonic) |
|
|
How may epilepsy impact day to day living |
Can't drive for 1 yr after diagnosis Can't drive larger vehicles (HGVs, buses etc.) for 10yrs Can't work in certain jobs May effect earning and employment - may therefore have an impact on the individuals psychological wellbeing etc. |
|
|
How may Drugs used for Epilepsy impact the oral environment? |
Phenytoin/ sodium valproate- gingival hyperplasia |
|
|
What are the two main pathological mechanisms that result in dermatitis? |
Abnormal epithelial barrier: Abnormal immune response to allergens |
|
|
Why are members of the oral health team prone to developing dermatitis? |
1. Primary irritant dermatitis 2. Acute/chronic exposure to irritants - e.g. soaps/detergents [remove protective oils and cause dry skin] 3. Type 4 reaction to allergen - Ni, glue plasters, wool, benzoates, topical drugs etc. |
|
|
What are the typical signs and symptoms associated with dermatitis? |
Primary irritant dermatitis o Itch o Hot red skin o Oedema (in acute phase) o Oozing/ weeping o Crusting ( in acute phase) o Fissuring and scaling in chronic phase o Excoriation (due to scratching. There may be secondary thickening andlichenfication) o Secondary infection o Impairment of thermoregulation (increased blood flow to the skin Nickel, triggers dermatitis, rare in mouth... (jeans button, jewellery, glasses frame Colophony , pine tree resin, glue plasters (Elastoplast) Others: fragrances, benzoates, wool, topical drugs. |
|
|
What can be done by healthcare workers to limit dermatitis? |
To avoid contact with sensitizing metals: Pierce ears with surgical steel posts Coat jewelry and clothing buttons causing reactions with clear non-sensitizing polish. Make keys of aluminum or other non-sensitizing metals. Test objects with dimethylglyoxime If perspiring, change shoes and socks often Wear cotton gloves under leather work gloves Avoid direct contact with cement and construction materials by using face masks and protective clothing. Moisturize hands often GOOD Hand hygiene important Wearing gloves throughout working day |
|
|
Define Angina |
A severe pain the chest that often spreads to the shoulder, arm, neck and mandible, due to an inadequate blood supply to meet the oxygen requirements of the heart (caused by a narrowed lumen of coronary arteries due to atherosclerotic plaque or fissured plaque) |
|
|
Pathology of Angina - Stable and unstable |
Stable - atherosclerotic plaque deposits result in the lumen becoming narrower. This results in inadequate blood for to meet increased oxygen requirements of the myocardium. (predictable) Unstable - Cracks and fissures develop in atherosclerotic plaques. These fissures are thrombogenic. o Thrombus start to form (some luminal narrowing that may lead to symptoms of angina) o Emboli shed from thrombi (critical narrowing) o Fissured plaque may heal (critical narrowing that my cause angina/ MI) |
|
|
List other diseases that a patient is at increased risk of developing if the have angina |
Dyslipidaemia Hypertension Diabetes ?smoking and lung cancer |
|
|
Invasive interventions to manage Angina |
Coronary artery bypass grafting (CABG) - saphenous vein graft from leg bypassing the constriction of the arty. Coronary revascularization (Percutaneous coronary intervention) Coronary artery angioplasty- vascular access via groin. Balloon catheter placed innarrowed artery and dilated. Coronary artery stent (+angioplasty) - deploys stent in artery. Reduces change orrestenosis. |
|
|
Prevalence of Diabetes |
In the UK prevalance is 3-4% of the population - due to western lifestyle. Has a rising prevalence and is expected to continue rising [obesity etc.] |
|
|
Management of Diabetes and why |
Neither injections nor tablets - Certain types of diabetes [II] may be controlled by diet. In some patients a controlled diet and weight loss can decrease HbA1c. Tablets but no Injections - In type 2 diabetes oral hypoglycaemic agents (OHAs) may be used to augment insulin secretion or utilise endogenous insulin (e.g. sulphonylureas, glitazones and meglitinides) [metformin] Tablets initially then injections - As HbA1c rises with time, Oral hypoglycaemic agents (OHAs) become insufficient for control. (Insulin is used in combination with OHA such as metformin- a biguanide). Injections and no tablets - Some patients have no or very little insulin (e.g. type 1 DM) therefore they take exogenous insulin as subcutaneous injection (exogenous insulin cannot be taken as an oral suspension) |
|
|
How may chronic liver disease with hepatic impairment impact on the delivery of oral healthcare? |
o Barrier to OH care: Patient availability, in terms of time and finance. OH might not be a priority. The dentist can improve the patient’s QOL by maintenance of oral healthcare to minimize likelihood of problems. o Orofacial manifestations: low levels of Vit B12 or ferritin (anaemia) o Increased tendency to infections – e.g. candida o PBC and secondary Sjogren’s syndrome o Careful dental prescribing- diminished drug metabolism and clearance. Potential forhepatotoxicity (e.g. Paracetemol or aspirin drug interactions) o Increased bleeding post extraction/ perio etc. - low levels of clotting factors o Adverse reactions from prescribed drugs eg. if had a liver transplant may be prescribed ciclosporin and be immunosuppressed - predispo to infections and neoplasia. and gingival hyperplasia. |
|
|
Define Multiple Sclerosis |
Inflammatory demyelinating disease of CNS (brain and spinal cord) that is disseminated in time (occur different points in time) and space (lesions occur at different sites). |
|
|
How can MS present via oral symptoms |
Trigem neuralgia, trigeminal sensory neuropathy and facial palsy Several types of oral lesions can be observed in patients with multiple sclerosis such as stomatitis, oral ulcers, glossitis, cheilitis, gingivitis, gingival hyperplasia (phenytoin), xerostomia, candidiasis, herpes, opportunistic infections, hemorrhagic changes and even certain forms of cancer (lymphoma, squamous cell carcinoma) in some patients who have been on long-term immunosuppressant treatment |
|
|
Describe the natural history of MS |
1. Illness initially acute attacks (1/2 a yr) and subsequent remission 2. Years pass... Recovery from acute attacks incomplete -> permanent impairment + disability(lower limb weakness, cerebellar dysfunction, wheelchair, urinary incompetence) 3. 10% pts -> primary progressive MS = lack of remissions + rapid progression of impairment+ disability OR benign MS lack of impairment after 10 years of diagnosis75% pts are alive after 35 yrs. Suicide x2-7 |
|
|
Common presenting clinical features of MS. |
1) Weakness 2) Optic neuritis (painful eye movement) 3) Paraesthesia (numbness +tingling) 4) Diplopia (double vision) 5) Micturition (passing urine) 6) Vertigo 7) Neuropathic pain – trigeminal neuralgia 8) Spasticity e.g. cramps, limb stiffness 9) Fatigue 10) Mood disturbance |
|
|
MS and barriers to oral healthcare |
Management: A side effect of antidepressants is xerostomia Loss of dexterity and poor oral hygiene Patients less likely attend (mood disturbance and fatigue) Oral health is not a priority (patient may be in pain) Patient comfort Physical access Xerostomia - denture adhesion/ prone to infections and trauma |
|
|
Describe the 3 Clinical Stages of HIV Infection. |
1. Primary infection: glandular fever/flu- like illness (fever, sore throat, body rash and other symptoms) 2. Post-sero conversion- may be asymptomatic and can last years. Virus continues to spread and damage immune system. 3. Acquired immunodeficiency syndrome- immune system very week. CD4 t cell count is <200 |
|
|
List 7 Oro-facial features associated with HIV infection |
Kaposi sarcoma (HHV8) Hairy leukoplakia (EBV) Non-Hodgkin’s lymphoma Periodontal disease (NUG, NUP, linear gingival erythema) Lymphadenopathy HPV warts Sialosis Cancers Candida |
|
|
HAART |
Highly Active anti-retroviral therapy |
|
|
Define Anaemia |
A reduction in haemoglobin concentration in the blood. Haemoglobin level below the normal for the age, gender and ethnic background of the individual. (normal range Hb- Men : 13.5- 18.0 g/dl, Women: 110.5-15.5 g/dl). |
|
|
Iron Deficiency Anaemia - blood film characteristics |
Iron deficiency anaemia Blood film: Small pale RBC. Blood count: low mean cell volume (MCV) and mean cell haemoglobin (MCH) |
|
|
Conditions associated with anaemia |
Blood loss: peptic ulcers, Gastrointestinal cancer, menorrhagia (heavy periods). The commonest cause of blood loss worldwide is hookworm. Pregnancy- due to increased requirements. Malabsorption- coeliac disease and Crohn’s disease. Dietary- rare in western countries. |
|
|
Oral Signs and Symptoms of Chronic Anaemia |
Angular cheilitis Depapilation of the dorsum of the tongue (glossitis) Erythema Oral ulceration (aphthous or other) Oral candidiasis Altered oral sensations (oral dysathesias e.g. Burning mouth syndrome) Mucosal pallor in extreme cases Plummer-vinson syndrome (dysphagia) |
|
|
List 4 focal neurological symptoms of a stroke/ TIA |
Loss (change) of speech Loss of movement Loss of sensation Loss of vision |
|
|
Describe the use of Apirin in relation to stroke |
Prevention - low dose aspirin to prevent stroke Acute - my reduce stroke symptoms/ long term consequences of stroke if given during acute phase [if cerebral infarct, will worsen if due to cerebral hemorrhage] |
|
|
How may the long-term consequences of a stroke impact oral health care |
Disability issues and access to the dental surgery Gaining informed consent ( + understanding) as there may be some cognitive impairment Loss of manual dexterity (effects maintaining oral hygiene) Pain and patient comfort Change in face shape + dentures may not fit anymore Medication: warfarin and clopidogrel (prolonged bleeding) Loss of protective gag reflex (no swallowing therefore good suction is needed) The dentist should be ready for a medical emergency incase this occurs. |
|
|
List oral signs and symptoms of Diabetes Mellitus |
Periodontal disease / Oral Infections / altered saliva quality and quantity / SialosisOral dysaesthesias / cranial nerve abnormalities / Delayed wound healing / adverse drug reactions |
|
|
List chronic illnesses associated with DM |
Vascular Disease Metabolic Syndrome Hypertension Heart Disease – CHD, Autonomic Neuropathy, Diabetic Cardiomyopathy Renal DiseaseEye Disease / Retinopathy Neuropathy / Diabetic Foot Sexual Dysfunction Pregnancy Wound healing |
|
|
How may parkinson's affect the delivery of oral healthcare |
Loss of manual dexterity - tooth brushing Difficulties with communication - dementia - problems with capacity Oral healthcare might not be a priority - depression etc. The impact of the disease on the patient’s physical function, physical comfort andmental wellbeing may affect the provision of OH care tremors may make provision of treatment a problem burning mouth Excess saliva Xerostomia from antimuscarinic drugs - trauma and lack of denture adhesion Lack of muscular control for denture wear. |
|
|
List the 3 features of a dependancy |
Subjective awareness of a compulsion to use the substance in question e.g. alcohol Increased tolerance Symptoms of withdrawal |
|
|
List Orofacial features of alcoholismm |
Angular Cheilitis Oral candidiasis Mucosal ulceration Glossitis with lose of filiform papillae (smooth tongue) Increased risk of oral cancer (especially if tobacco smoker) Dental erosion if vomiting frequently Abnormal oral sensation Sialosis – painful enlargement of major salivary glands (usually bilateral parotid) |
|
|
General Signs of alcohol abuse |
Distress / agitation (CNS depressant) Hand tremorSweatingGI disturbancesIllusions and hallucinations Fits |
|
|
Name mental illnesses associated with alcoholics |
Depression Amnesia Dementia Personality deterioration |
|
|
What investigations would you conduct to confirm a suspected diagnosis of a mandibular fracture - in a dental surgery and in a hospital |
In a dental surgery - Radiographs at 2 views [90º] generally OPT and PA variable In a hospital Lateral obliques (right and left) CT scans for fracture condyles |
|
|
List signs of a mandibular fracture |
Pain / Swelling / Paraesthesia/anaesthesia of ID nerve / Tenderness over region of TMJ / Loose teeth/missing teeth / limited opening of mouth / Deformity / deranged occlusion / haematoma (sublingual) |
|
|
How would you treat a mandibular fracture |
Undisplaced – conservative management Displaced – Ideally treated within 8h under nasotracheal intubation (GA) Special Circumstances – Fractured condyles Intermaxillary fixation (IMF)– 6 weeks Mini plates – 2mm plates / passive plate positioning / 2 screws either side of fracture Analgesia – NSAIDs/Opioids Temporary stabilisation – bridal wire to immobilise fracture IV Fluids and antibiotics Open reduction internal fixation (ORIF) – miniplates and osteosynthesis / temporary IMF Post-Operative immobilisation – transalveolar screws / buttons / elastics |
|
|
List clinical signs and symptoms of anaphylaxis |
Neck and/or tongue swelling with upper airways obstruction / Increasing respiratory distress with noisy breathing / increasing pulse rate and decreasing blood preasure / decreasing level of consciousness / red rash / Flushing / Urticaria / urticarial (‘hives’) rash / angioedema / abdominal pain or vomiting / runny nose and/or tearing eyes / sense of impending doom |
|
|
How and where is adrenaline administered? |
Adrenaline Auto-Injector – EpiPen – Adrenaline 0.30mg over 6 years old / 0.15g 6 months to 6 years Jab EpiPen firmly in to the mid point of the antero-lateral thigh – needle enters at 90O to the skin / hold in place for 10 seconds |
|
|
Explain the mechanism of action of adrenaline works |
Epinephrine is a direct-acting sympathomimetic drug that acts as an agonist at alpha and beta- adrenergic receptors. It produces vasoconstriction to counteract the vasodilation and resulting hypotension associated with anaphylaxis. The bronchodilatory effects of epinephrine and its ability to reduce mucosal oedema relieve bronchoconstriction and improve respiratory effort. |
|
|
How would you explain to a patient how to use Betnesol? |
Betamethasone soluble tablets – 500mcg - Dissolve one tablet in 10ml of WARM water Hold in mouth ensuring affected parts of the mouth are covered for up to 4 minutes Spit out – do NOT swallow Use up to four times a day with the frequency of use titrated against benefit |
|
|
List potential triggers of a lichenoid reaction |
Dental materials e.g. Amalgam, gold, composites / Drugs / Hepatitis C Graft-versus-host-disease Others (uncommon) – Hep B Vaccination, chewing gum, HIV |
|
|
6 Functions of the Kidneys in Health |
1. Excrete toxic metabolytes 2. Vit d metabolism 3. Drug metabolism 4. Hormone Metabolism - control of blood pressure 5. Reabsorption of proteins and water (dons answer) Kidneys receive around 20% of cardiac output – blood is filtered through ~2 million glomeruli to form glomerular filtrate, then extensively modified as it passes through renal tubules to form urine that passes along ureters to bladder Fluid Balance – maintenance of water and electrolyte balance; recovery of ions is essential, water reabsorption, facilitated by secretion of vasopressin from the pituitary gland, some ions e.g. Hydrogen and Potassium excreted into the nephron essential for correct maintenance of body’s electrolyte composition Excretion of Waste Products – Urea, main nitrogenous product and Creatinine, by-product of normal muscle metabolism Acid-Base Balance and pH – Hydrogen ions generated primarily by metabolism of sulphur-containing amino acids, kidney maints correct acid-base balance via secretion of hydrogen ions and bicarbonate reabsorption Endocrine Functions – produces erythropoietin – upregulates production of RBCs- Produces Renin for renin-angiotensin-aldosterone pathway, i.e. stimulation release of angiotensin I which is converted to angiotensin IIKidney is essential for normal vitamin D metabolism and maintenance of normal bone turnover – Vit. D undergoes hydroxylation in kidney, promotes Calcium absorption from intestine. Calcium and Phosphate closely linked – Calcium levels fall, Phosphate increases. Reduced Vit. D = Reduced Calcium and raised levels of phosphate, increased PTH to correct low calcium levels. Chronic disruption of calcium can results in renal bone disease |
|
|
What are the commonest causes of acquired renal impairment in the UK? |
HTN and diabetes mellitus. |
|
|
Given example of interventions to manage patients with end stage renal failure |
1. Dialysis - haemodialysis or peritoneal 2.Tranplant |
|
|
Describe the main differences between the two kinds of (rrt) renal replacement therapies |
Dialysis may be started before end stage renal failure has developed; Once end stage renal failure has developed, then RRT is required to maintain life – it may be used for many years. Dialysis – Haemodialysis – undertaken in hospital setting – i.e.patient travels to the dialysis unit, required three times a week – each session may last several hours / need vascular access / dialysis machine / heparin used to prevent clotting caused by dialysis machine Peritoneal Dialysis – alternative to haemodialysis, may take place at home / catheter inserted into peritoneal cavity and dialysis fluid inserted / peritoneum acts as dialysis membrane / done over 4 occasions during 24 hour period Transplant –Preferred option for end-stage renal failure / Donor kidneys may come from deceased or living donors /tissue matching to reduce but not eliminate graft rejection / placed extraperitoneally in the iliac fossa / need for immunosuppression to avoid rejection needed in nearly all cases |
|
|
Define Rheumatoid Arthritis |
An autoimmune disease characterised by inflammation of the synovium leading to inappropriate proliferation of the synovium giving joint dysfunction - pain and dysfunction of the joints. Has articular and extra-articular involvements. |
|
|
What are the aims of management of rheumatoid arthritis? |
Aims are to manage symptoms and prevent complications. Weigh up benefits of drugs against side effects. Limit organ and tissue damage Pharmacalogical interventions |
|
|
List the features of rheumatoid arthritis that may impact on the patients oral health and the provision of oral healthcare |
1. dexterity - patient may not have the dexterity to brush teeth or look after a denture -therefore oral hygiene may be poor 2. barriers - in terms of access - patient may struggle to physically attend 3. patient may be uncomfortable in chair. 4. patient may also suffer with sjogren's disease therefore may suffer with xerostomia - oral health, trauma, bad breath, denture adhesion. 5. Oral health may be a low priotity to the patient. 6. Patient may suffer with depression - motivation 7. ADRs - immune modulating drugs may predispose to oral infections. |
|
|
Define Anylosing Spondylitis |
Spiral arthritis tends to affect young males - its an autoimmune disease leads to ankylosis of vertebral and sacroileac joints. This is characterised as symptomatic sacrolitis (inflammation of the sacroiliac joints) where there is persistence pain and stiffness for >3months where the stiffness predominates in the mornings and is improved on exercise and worsening when at rest. Although it is primarily a spinal disorder it can affect other joints. In Caucasian people it affects approximately 1% of men and 0.5% of women. It is progressive disease that presents in young adults and is associated with disability in later life. It has a multifactorial aetiology with a recognised genetic factor with mutations in the HLA-B27 |
|
|
Describe 3 complications of Ankylosing Spondylitis |
Lower back pain, muscular spasm, reduced mobility - bamboo spine entheriopathy - pathological change where tendons and ligs insert bone. Other tissues - IBD - crohn's and UC, Psoriasis, Iritis, Osteoporosis, Fatigue. Plantar fasciitis o Pain in heel and arch of foot Costochronditis o Inflammation of the cartilage that connects the inner end of each rib with thesternum which causes chest pain Achilles tendonitis o Pain at the insertion of the Achilles tendon into the heel. |
|
|
Ankylosing spondylitits primarily affects the vertebrae and sacroileac joints. List other tissues, organs and conditions that may be involved. |
Inflammatory bowel disease o Crohns o Ulcerative colitis Skin o Psoriasis Eye o Iritis Bone o Osteoporosis Fatigue |
|
|
List pharmacological interventions in the management of Ankylosing Spondylitis |
NSAIDs Bisphosphonates Disease modifying anti-rheumatic drugs (DMARDs) o Methotrexate o Gold Anti-TNFα antibody drugs o Infliximab |
|
|
List the non-pharmacological management of Ankylosing spondylitis |
Physiotherapy - regular excercises and stretching/ rest/ diet and weight control/ Relieve pain Reduce inflammation Maintain good posture and function Regular exercise Stop smoking Aids |
|
|
Define the term coeliac disease |
Gluten sensitive enteropathy |
|
|
Describe the pathological events in Coeliac disease |
Caused by an inappropriate T-cell response to the protein [gluten] This leads to inflammation and destruction of the villi in the gastro-oesophageal tract. This leads to maladsorption, bloating, pain, fatigue etc. An inappropriate T-cell-mediated immune response against gluten in a genetically predisposed individual Present in approximately 1% UK / Common in West Ireland Gluten –Protein fraction of wheat |
|
|
How is coeliac's diagnosed? |
Blood tests - anamia and deficiency states Colon/endoscopy - biopsy Blood tests - autoantigen Stool examination - steatorrhoea Specific antibody tests - Immunoglobulin A (IgA) anti-tissue transglutaminase antibody is the single preferred test for detection of coeliac disease. If abnormally elevated levels of IgA endomysial and anti-tissue transglutaminase antibodies are found, a person almost certainly has celiac disease. Small intestinal biopsy - People who test positive for celiac disease antibodies, or who have a high probability of celiac disease regardless of the results of the blood tests, should have a small intestinal biopsy to confirm the diagnosis. A pathologist evaluates the tissue samples for loss of villi and other characteristics of celiac disease, such as an increased number of lymphocytes. Stool examination for malabsorption - Stool from patients with celiac disease often contains many globules of fat -- a condition called steatorrhoea -- that can be viewed under a microscope using a dye to make them visible. To conclusively diagnose steatorrhoea, however, stool is collected over a 72-hour period, and the fat in the stool is chemically measured and quantified.Blood tests for malabsorption and vitamin deficiencies - Malabsorption reduces the absorption of protein and causes a reduction in blood protein levels. This can be seen commonly as a reduced blood level of albumin, the most concentrated protein in blood. Intestinal malabsorption can lead to deficiencies and low blood levels of iron,calcium, vitamin B12, folate, and the fat- soluble vitamins (A, D, E, and K). Iron deficiency anemia, abnormally prolonged PT (delayed clotting) may result, however these also occur in other diseases not just coeliac and are not the most reliable. |
|
|
Give example of how undiagnosed coeliac disaese may have a negative impact on a patients general health |
1. Malabsorbtion - B12 deficiency (uncommon) 2. Steatorrhoea - fat malabsorption/anaemia - iron and folate malabsorbtion/ osteoporosis - vit D 3. Weight loss – amenorrhoea 4. Dermatitis herpetiformis - itchy, blistering rash on extensor surfaces of limbs (almost always associated with coeliac diseases but not vice versa) |
|
|
What is the main intrevention used to control coeliac disease? |
Avoid gluten |
|
|
List oral features of coeliac disease |
Enamel defects / delayed eruption / recurrent aphthous ulcers / cheilosis / oral lichen planus / atrophic Glossitis |
|
|
Describe features of COPD that distinguish it from asthma |
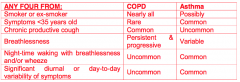
1. COPD is not completely reversible 2. COPD not worse at any particular time of day 3. COPD not generally found in younger people 4. COPD is primarily found in smokers |
|
|
COPD - define |
A chronic progressive, not completely reversible inflammatory obstruction of the lungs - SOB, etc. Does not change markedly over severl months |
|
|
List risk factors of smoking that impact oral health |
Oral Cancer / Chronic Periodontitis / NUG / Potential to lose teeth due to gum disease |
|
|
In a patient who wears an upper partial acrylic denture - describe the potential adverse effects on the oral cavity of interventions used to manage COPD. |
Corticosteroids – e.g. 2 week course of Prednisolone Inhaled – Patient should rinse mouth with water after use to reduce the likelihood of oral candidiasis and denture stomatitis Good denture hygiene is needed - Microorganisms can be aspirated off the denture plaque biofilm into the lower respiratory tract and could reduce the patient's immunity and cause pneumonia. Systemic – Morbidity associated with systemic steroids - cushings/ adrenal crisis[steroid cover] COPD Exacerbation –Delivery of oral healthcare dependent on –What treatment is required / severity of the exacerbation / morbidity of the exacerbation / stage in the evolution of the exacerbation If patient is smoking – smoking cessation advice will improve control of any oral diseaseDry mouth can be related to oxygen use (via a mask) – sip fluids / rinse / use artificial saliva products / dry mouth can lead to dental caries / suck sugar free lollies or chew gum / regularly clean both teeth and dentures to reduce bacteria build-up / have regular dental check-ups |
|
|
Describe the three cardinal features of addiction |
1. Withdrawal symptoms 2. Subjective compulsion 3. Tolerance |
|
|
Define the term leukaemia |
Two Forms – Acute Leukaemia and Chronic Leukaemia - both may be further subdivided. Result of accumulation of early myeloid or lymphoid precursors in the bone marrow, blood and other tissues Probably occurs by somatic mutation in a single cell within a population of early progenitor cells. May arise de novo or be the terminal event of a pre-existing blood disorder |
|
|
Give a simple classification of Leukaemia |
Acute Leukaemia – Acute Myeloid Leukaemia / Acute Lymphoblastic LeukaemiaAML – with recurrent genetic abnormalities / with multilineage dysplasia – includes secondary AML (MDS, therapy related) / AML not otherwise categorised Chronic Leukaemia – Chronic Lymphocytic Leukaemia / Chronic Myeloid Leukaemia / Other Chronic Lymphoproliferative Disorders |
|
|
List 5 oral clinical features of untreated leukaemia |
1. Lymphadenophy 2. ulcerations 3. bleeding/ bruising Gingival bleeding / petechiae / ecchymosis / gingival enlargement / gingival ulceration / oral infection e.g. candidiasis, herpes simplex virus infection, periodontal bone loss / necrotic lesions / |
|
|
List modalities of treatments used to treat leukaemia |
Induction chemotherapy to obtain remission / Consolidation treatment with further courses of combination chemotherapy / prophylaxis of meningeal leukaemia with intrathecal methrotrexate and cranial irradiation / maintenance chemotherapy / bone marrow transplantation in ‘bad-risk’ patients |
|
|
Describe of Oral Complications common to chemo and radiotherapy |
Oral complications common to both chemotherapy and radiation Oral mucositis: inflammation and ulceration of the mucous membranes; can increase therisk for pain, oral and systemic infection, and nutritional compromise. Infection: viral, bacterial, and fungal; results from myelosuppression, xerostomia, and/ordamage to the mucosa from chemotherapy or radiotherapy. Xerostomia/salivary gland dysfunction: dryness of the mouth due to thickened, reduced, orabsent salivary flow; increases the risk of infection and compromises speaking, chewing, and swallowing. Medications other than chemotherapy can also cause salivary gland dysfunction. Persistent dry mouth increases the risk for dental caries. Functional disabilities: impaired ability to eat, taste, swallow, and speak because of mucositis, dry mouth, trismus, and infection. Taste alterations: changes in taste perception of foods, ranging from unpleasant to tasteless. Nutritional compromise: poor nutrition from eating difficulties caused by mucositis, dry mouth, dysphagia, and loss of taste. Abnormal dental development: altered tooth development, craniofacial growth, or skeletal development in children secondary to radiotherapy and/or high doses of chemotherapy before age 9. Other complications of chemotherapy Neurotoxicity: persistent, deep aching and burning pain that mimics a toothache, but forwhich no dental or mucosal source can be found. This complication is a side effect ofcertain classes of drugs, such as the vinca alkaloids. Bleeding: oral bleeding from the decreased platelets and clotting factors associated withthe effects of therapy on bone marrow. Other complications of radiation therapy Radiation caries: lifelong risk of rampant dental decay that may begin within 3 months ofcompleting radiation treatment if changes in either the quality or quantity of saliva persist. Trismus/tissue fibrosis: loss of elasticity of masticatory muscles that restricts normalability to open the mouth. Osteonecrosis: blood vessel compromise and necrosis of bone exposed to high-doseradiation therapy; results in decreased ability to heal if traumatized. |
|
|
Define Atrial Fibrillation and Ventricular Fibrillation |
AF - Most commonly sustained chaotic, uncoordinated and ineffective depolarisation of the atria - insufficient contraction of the atria VF - an abnormally irregular heart rhythm caused by rapid, uncoordinated fluttering contractions of the ventriclesVentricular Fibrillation is rapidly fatal – ‘cardiac arrest’ |
|
|
Explain the Management of AF and VF |
Atrial Fibrillation: Three broad areas of intervention: • Anti-thrombotic therapy; • Cardioversion - correction from AF to sinus rhythm:– Pharmacological / Electrical • Pharmacological rate control Ventricular Fibrillation:Implantable cardioverter-defibrillator: – Placed when risk of ventricular fibrillation |
|
|
What are the consequences of untreated Atrial Fibrillation |
Stroke can occur because the top chamber of the heart is in a very chaotic and rapid rhythm. When this occurs, the top chambers are not able to squeeze and pump the blood as it is designed to do. By nature, when the blood flow slows, it has the tendency to form a clot. Congestive heart failure may also be caused by atrial fibrillation, a condition called "tachycardia induced cardiomyopathy." When the main chamber of the heart has been pumping for a long time at such a rapid heart rate induced by the atrial fibrillation, the heart muscle can become very weak and cause congestive heart failure. |
|
|
List the 3 commonly related malabsorption conditions related to coeliac disease and the consequences of each. |
Steatorrhoea – Fat malabsorption / Anaemia – Iron and folate malabsorption / Osteoporosis – Vit D malabsorption / B12 deficiency uncommonWeight loss – amenorrhoea |
|
|
Name and describe a common condition (not a malabsorption condition) almost always associated with coeliac disease |
Dermatitis herpetiformisItchy, blistering rash on extensor surface of limbs Almost always associated with coeliac disease (but not vice versa) |
|
|
Name complications of not sticking to a coeliac diet |
• Osteoporosis • InfertilityIncreased risk of some cancers Complicated / refractory coeliac disease – Jejunal ulceration – Lymphoma |
|
|
Describe the relationship between bisphosphonates and osteonecrosis of the jaw |
Bishphonates reduce the action of osteoclasts. They also affect the vasculature of bone Remodelling [resporption/formation] is imperative for healing. Following an extraction a person on bisphophonates will not heal as well and the extraction socket will become necrotic and will appear as exposed bone. |
|
|
Bisphosphonates are used for: |
1. Osteoporosis 2. Paget's 3. Bone cancers osteogenesis imperfecta / fibrous dysplasia / primary hyperparathyroidism / cystic fibrosis / multiple myeloma / breast cancer / prostate cancer / bony metastatic lesions / hypercalcaemia of malignancy |
|
|
Describe the clinical features of BRONJ |
Exposed, necrotic bone in the maxilla or mandible that has persisted for more than eight weeks in patients taking bisphosphonates and where there has been no history of radiation therapy to the jaw. Symptoms include delayed healing following a dental extraction or other oral surgery, pain, soft tissue infection and swelling, numbness, paraesthesia or exposed bone. |
|
|
Describe the mode of action of bisphosphonates |
Hndering the formation, recruitment and function of osteoclasts. |
|
|
Describe the current guideline r.e dental procedures and osteonecrosis. |
If at all possible, extraction of teeth should be avoided If extractions, or other procedures which may disrupt the mucosal covering of bone areunavoidable, the surgery must be ‘covered’ with a short course of an antibiotic such asamoxicillin, penicillin V or erythromycin. Patients should not have ANY dental procedures in the 24h following an IV infusion of abisphosphonate If a patient experiences slow healing of a site following dental extraction they should be referred to an Oral and Maxillofacial Surgeon for diagnosis and management |
|
|
Describe the ABCDE of pigmented skin lesions |
A - Asymmetry B - border [irreg] C - Colour [2 or more/change] D - diameter - >6mm E -evolutionary changes |
|
|
Define the term melanoma and discuss the prevalence of malignant melanoma. |
A melanoma is a malignancy arising from cutaneous melanocytes. Prevalence is rising - due to increased UV rayz. - more people go on holiday now and use the sunbeds. |
|
|
List risk factors in the formation of a melanoma |
1. Being fair skinned - blonde and blue eyes 2. Having loads of moles 3. UV sun exposure 4. Poor UV protection practice - tees, sunscreen, hats, avoiding the hottest sun. UV light exposure is the main risk factor: – Sunlight – sunbathing – Sunbeds • Risk factors for melanoma include: – Skin that does not tan or that burns easily – Red or blond hair – Pale coloured eyes People should be considered to have higher risk (approximately 10-fold) of malignant melanoma if they have: – >100 normal naevi or 5 atypical naevi – Atypical moles: • Changing shape or colour– Two or more cases of melanoma in 1st degree relatives |
|
|
List types of recognised melanoma |
Acral lentiginous, superficial spreading, nodular, lentigo maligna. |
|
|
Discuss the management of a melanoma |
Biopsy, - excisional [cure] Removal Monitoring Radiot/chemo depends on staging - TNM |
|
|
Discuss the primary prevention of melanoma |
Regular check up/ good monitoring of moles/new moles. UV protection - sunscreen over 15, covering up, wearing hats, avoiding the hottest sun. avoid the beds babe. |
|
|
list symptoms of Xerostomia |
1. Dryness of the mouth 2. Burning mouth 3. troubles eating [dysphagia] 4. Difficulties articulating • Altered quality of saliva (thick, ropey) • Dry mouth • Oral discomfort– May include burning sensations • Difficulty chewing & swallowing (dysphagia)– Difficulty eating certain foods (e.g. dry foods) • Altered taste sensation • Halitosis • Difficulty speaking (articulation) • Symptoms associated with – Periodontal disease – Caries – Infections (fungal and bacterial) • Difficulty in wearing dentures (retention) • Depression in some |
|
|
Define xerosotomia |
Percieved/actual dryness of the mouth |
|
|
List signs of xerostomia |
1. Dryness of the mouth - dry and glazed mucosa, sticky erythmatous mucosa, lobulatied, depapilated fissured tongue. 2. frothing of saliva at lines of contact/ no pooling 3. trauma 4. ulcerations. 5. heapsa caries 6. Candida and angular (merckel) cheilitis 7. Perio 8. Ascending bacterial sialadenitis |
|
|
Describe the iatrogenic causes of xerostomia |
1. Medications such as antimuscarinics - may cause xerostomia as an adverse drug reaction Act via different mechanisms to suppress saliva production / a large number of different prescribed drugs can cause xerostomia / some recreational drugs cause profound dryness 2. If the parotid gland was to be removed - this would cause xerostomia 3. Radiotherapy - Irradiation to the head & neck / Serous cells more susceptible to damage than mucus cells / Reparative fibrosis replaces the glandular tissue / Saliva production drops and the saliva has a thick, tenacious quality with altered biochemistry and properties. 4. GvHD Reduced saliva: – Radiotherapy & drugs may contribute./ Generalised mucosal inflammation; / Lichenoid lesions: – Often erosive / Infections: – Especially Candida / Hairy Leukoplakia: – A manifestation of EBV infection. |
|
|
Describe 2 non iatrogenic causes of xerostomia |
1. Sjogrens - an autoimmune disease of the exoc rine glands causing xerostomia and decreased lacrimation 2. Mumps can cause swelling of the parotid glands and also a reduced amount of salivary flow 3. Diabetes mellitus can cause altered quality and quantity of saliva 4. Dehydration 5. Sarcoidosis Sympathetic outflow • Transient dryness – e.g. when nervous./ Dehydration • Fluid restriction; • Excess fluid loss: – Hot weather, diabetes, excess alcohol / Salivary gland disease • Sjögren’s Syndrome; • Sarcoidosis / Infection • Transient: – Mumps. – HIV; – Hepatitis C (any xerostomia is usually mild) / Diabetes Mellitus • Especially when poorly controlled (dehydration); • Also an element of salivary gland/nerve dysfunction |
|
|
Discuss the management of Xerostomia |
• Remove the cause if possible:– Usually relates to drugs (liaise with doctors).• Minimize exacerbating factors:– Avoid smoking, spirits and low humidity;– Avoid irritants such as mouthwashes;– Avoid dry & spicy foods: • Add extra sauces & gravy, blend food...– Correct mouth-breathing;– Treat candidiasis.• Restorative – Regular need to see / excellent denture and oral hygiene / regular OH therapy / dietary advice to reduce carbohydrate exposures / fluoride (toothpaste, mouthwashes...)• Symptomatic relief - frequent sips of water / room air humidifiers / artificial salivas and related products / chewing gum |
|
|
List five functions of the liver in health |
Processing and storage of nutrients in the gut Bile synthesis and excretion Synthesis of coagulation factors and other proteins (vitamin K dependent coagulationfactors and albumin) Infection and immunity (macrophage lineage Kupffer cells) Hormone metabolism Vitamin D metabolism Drug metabolism |
|
|
Describe how hepatic impairment can have a profound effect on a drug i) PK ii) PD |
Pharmacokinetics, e.g.:Active drugs and/or their active metabolites will accumulate with potentially adverse effects, if inhealth the liver contributes to their excretion; The activity of some drugs is influenced by their degree of protein binding, which can bechanged in hepatic impairment. Pharmacodynamics, e.g.: The sensitivity of the target tissues to specific drugs may be either increased or decreased with potentially adverse effects. |
|
|
Discuss the management of liver failure |
o Control symptoms related to liver impairment (e.g. the physical discomfort associated with massive ascites or the pruritus of jaundice) o Limit any further liver damage; and where possible o Improve liver function (e.g. by reducing hepatic venous congestion); o Undertake organ transplantation at the appropriate time in those close to end stage liver failure. |
|
|
Describe the importance of management when planning and delivering orofacial healthcare to a patient with liver impairment |
o Barrier to OH care: Patient availability, in terms of time and finance. OH might not be a priority. The dentist can improve the patient’s QOL by maintenance of oral healthcare to minimise likelihood of problems. o Orofacial manifestations: low levels of Vit B12 or ferritin (anaemia) o Increased tendency to infections – e.g. candida o PBC and secondary Sjogren’s syndrome o Dietary habits and oral hygiene: Impaired liver function may be associated with poor control of blood glucose levels; Some patients need to snack on carbohydrates through the day to avoid hypoglycaemia which may impact upon: The number of sugar exposures in a day and an increased risk of caries or periodontal disease; and The planning of long dental procedures. o The side effects of therapeutic interventions such as: Immunosuppressants or immune modulating drugs, for example followingliver transplant (e.g. ciclosporin and gingival overgrowth). o Drug prescription where there is liver impairment (and possibly associated renal impairment)with reference to: Diminished drug metabolism and clearance; The potential risk of hepatotoxicity (e.g. paracetamol or aspirin); Drug interactions. o The disease and its management may also have a significant impact on other family memberssuch as spouses, with associated barriers to the family members accessing oral healthcare. |
|
|
Give a brief description of the changes of the airway in an asthma attack |
Asthma is a chronic condition characterised by: Chronic inflammation of the bronchi with oedema and increased mucus secretion; Bronchial hyper-responsiveness leading to sudden, but reversible luminal narrowing and airways obstruction during an asthma attack. |
|
|
List risk factors for acute life threatening asthma attack |
Exercise / Viral infections / Iatrogenic – NSAIDs/Beta-blockers / Occupational e.g. Painters, Bakers, Chemical workers / Environmental – Dust/Pollens/Animal fur or feathers / Smoke e.g. Tobacco / family history of asthma / history of atopic disease e.g. childhood eczema and hayfever |
|
|
What type of drug is salbutamol and what is its pharmacological action? |
β2-Agonist DrugAct at β2-adrenoreceptors to improve respiratory function: Main action – direct on smooth muscle Bronchodilatation – reduced small airways resistance Dilatation of associated lung blood vessels |
|
|
Why may a spacer used for the inhalation of salbutamol |
Spacer improves metered dose inhaler delivery to the lungs Increases amount reaching lungs Increases flow dynamics compared to if a spacer is not used |
|
|
Explain the meaning of HbA1c and how it is used |
Haemoglobin becomes glycosylated in presence of glucose; • HbA1C gives a measure of glycosylated haemoglobin. – Good indicator of glycaemic control over last 8- 12 weeks: Health – 20-41mmol/mol / Diabetes good control <59mmol/mol |
|
|
List 4 symptoms of diabetes that can be seen in the mouth |
Oral infections / altered saliva quality and quantity / sialosis / oral Dysaesthesias / delayed wound healing / adverse drug reactions / xerostomia / metallic taste – metformin / candidiasis / cranial nerve abnormalities |
|
|
List normal functions of the kidneys in health |
1. Excretion of waste products 2. Maintenance of acid base balance 3. drug metabolism 4. Hormone metabolism - renin and angiotenisn and sex hormones 5. filtration of blood 6. fluid balance 7. Maintenance of normal bone turnover |
|
|
List chronic consequences of renal impairment and for each one outline an adverse impact of oral health |
1. Adversed drug reactions from medications 2. GvHD is a recipient of a kidney transplant - oral ulcerations 3. CVD complications - warfarin meds and prolonged bleeding 4. Cardiovascular Disease – CHD – Orofacial pain / Angina – acute attacks and induction by local anaesthetic vasoconstriction / xerostomia from medication / caries from xerostomia / Heart Failure – patient positioning / access to OHC / priority of OHC / invasive IE with prosthetic heart valves Anaemia – Pallor of the mucosa / Glossitis / angular stomatitis Abnormalities of Coagulation – prolonged bleeding / drug interactions with antiplatelet/anticoagulant drugs / warfarin interactions Renal Bone Disease (Renal Osteodystrophy – As kidney function declines, calcitriol production and phosphorus excretion decrease, which results in phosphorus retention and contributes to the development of hyperparathyroidism. Malnutrition – caries / periodontal disease / oral cancer / bleeding gums / Glossitis / angular cheilosis / mucosal petechiae / enamel defects / muscles of mastication malformation/dystrophy/cramps Tissue Oedema – Uraemic stomatitis is now a rare condition in the United Kingdom, but may occur in patients with very high urea levels and is characterized by: Unpleasant taste and breath that smells of ammonia / A thick grey pseudomembrane overlying areas of oral mucosa that may be ulcerated. Impairment of the Immune System – e.g. oral candidiasis or delayed soft tissue wound healing / increased propensity for infections Malignancy – Alcohol, tobacco or recreational drugs – risk of oral cancer partially due to impairments of parts of immune system that fight early cancers Sexual Dysfunction and Pregnancy – Minimise drug use / drug interactions / LA use during pregnancy / periodontal problems / pyogenic granulomas / hypogonadism treatment by buccal tablets can lead to transient gum irritation and a bitter taste are the chief adverse effects associated with this route. Gum irritation tends to resolve within the first week. Other adverse effects include dry mouth, toothache, and stomatitis Mental Health Problems – depression / anxiety leading to non-attendance / phobias/psychotic states leading to avoidance of the dentist and decrease in OH and increase in most dental problems / effect of drugs on OH such as xerostomia Childhood Development – chronic renal failure resulting in risk of dental abnormalities such as enamel defects / impaired haemostasis i.e. care with any drug prescription / treatment only happens on non-dialysis days / if patient has transplant – effects of immunosuppressant drugs / orthodontic treatment if needed before transplantation due to immunosuppressant drugs and overgrowth/gingival hyperplasia |
|
|
Descibe the impact of renal impairment on drug pharmacokinetics and dynamics |
Pharmacokinetics - e.g.: potentially adverse effects, if in health the kidney is normally responsible for their excretion (e.g. NSAIDs); The activity of some drugs is influenced by their degree of protein binding, which can be changed in renal impairment. Pharmacodynamics The sensitivity of the target tissues to specific drugs may be either increased or decreased with potentially adverse effects. |
|
|
Define Dysphagia and Odynophagia |
Dysphagia - difficulty or discomfort in swallowing, as a symptom of disease. Odynophagia – painful swallowing [painful swallowing, in the mouth (oropharynx) or oesophagus. It can occur with or without dysphagia. Odynophagia often results in inadvertent weight loss] |
|
|
What questions would you ask a patient with a history of dysphagia |
What happens when you try to swallow? Is it water and food? Oropharyngeal or oesophogeal? Difficulty initiating the swallow? does the food stay in your mouth or throat? does it stick.. where? |
|
|
List oropharyngeal causes of dysphagia |
• Neuromuscular – Stroke – Parkinson’s – MND – Muscular dystrophies • Obstruction – Pharyngeal pouch – Goitre • Decreased saliva • Radiation • Sjögren’s • Drugs– Alzheimer’s |
|
|
What is a peptic ulcer and describe their aetiology |
Larger breaks in the gastro-intestinal mucosa caused by the caustic effect of acid and pepsin Peptic ulcers occur when acid in the digestive tract eats away at the inner surface of the esophagus, stomach or small intestine. The acid can create a painful open sore that may bleed. Helicobacter pylori bacteria commonly live in the mucous layer that covers and protects tissues that line the stomach and small intestine. Often, H. pylori causes no problems, but it can cause inflammation of the stomach's inner layer, producing an ulcer. Regular use of certain pain relievers – e.g. aspirin, ibuprofen, naproxen, ketoprofen and others |
|
|
List complications of peptic ulcers |
• Bleeding – Acute – haematemesis, melaena Chronic – iron deficiency anaemia • Perforation • Outlet obstruction – Vomiting– Fullness – Wt loss |
|
|
How are peptic ulcers treated |
“Test & Treat“ – Detect and treat H. pylori Stop NSAID’s Stop smoking Acid suppression – Proton pump inhibitors (eg. omeprazole, lansoprazole) – H2 receptor antagonists (ranitidine, cimetidine) |
|
|
Define Ostemyelitis, ORN, and Osteoporosis |
OM - An infective disease of bone, which results in necrosis of an area of the affected bone ORN - necrosis of bone primarily due to radiation therapy Osteoporosis - A systemic skeletal disease characterised by decreased bone mass density and abnormal bone architecture. |
|
|
List iatrogenic factors that increase bone resorption |
Glucocorticoids Thyroxine Heparin Diuretics (frusemide) Cytotoxic drugs |
|
|
List lifestyle factors that increase bone resorption |
Alcohol Tobacco Bed rest |
|
|
If a patient with osteoporosis was to fall and injure themselves, what injuries are they likely to sustain? |
Wrist, hip fractures Colles’ Fracture • Fracture of the lower end of the radius with displacement of the distal fragment dorsally • Typically sustained during a fall: – Hand is outstretched to break the fall. |
|
|
Describe the effect of osteoporisis on posture |
• Kyphosis:Forwards curvature of the spine; • Loss of height • Hunched posture • Abdominal protrusion |
|
|
Discuss the dental management on a patient with osteoporosis |
Bisphosphonate therapy treatment of osteolytic bone disease e.g. osteoporosis – Usually ORAL Recently a relationship between bisphosphonate therapy and osteonecrotic lesions in the jaws has been demonstrated. Extractions almost always precede development of an osteolytic lesion. Patients with this condition develop exposed bone in the jaw. The overlying tooth often is lost and a non- healing, often-painful lesion remains. If at all possible, extraction of teeth should be avoided If extractions, or other procedures, which may disrupt the mucosal covering of bone are unavoidable, the surgery must be ‘covered’ with a short course of an antibiotic such as amoxicillin, penicillin V or erythromycin. Patients should not have ANY dental procedures in the 24h following an IV infusion of a bisphosphonate If a patient experiences slow healing of a site following dental extraction they should be referred to an Oral and Maxillofacial Surgeon for diagnosis and management |
|
|
Define Abscess and Cellulitis |
Abscess - infection - localised collection of pus Cellulitis is an spreading infection not characterised by the accumulation of pus |
|
|
Discuss the local and regional factors associated with an abscess |
Local - swelling, pus, bad taste, dodgy tooth, inflammation - redness, pain, swelling heat Regional - trismus - MoM Dysphagia Induration |
|
|
Discuss the systemic factors associated with an abscess |
Raised Temperature (>37°C) Raised pulse & respiratory rate Lymphadenopathy Neutrophil leukocytosis Malaise |
|
|
Describe the action of penicillin |
Inhibition of cross-linking (murein, peptidoglycan) •Target - transpeptidase •Activation of hydrolases •Bactericidal effect |
|
|
Describe how patients develop a penicillin resisitance
|
Bacteria that can destroy penicillin do so by secreting enzymes called beta-lactamases. These enzymes cleave the beta-lactam ring of penicillin so that the drug becomes inactive. |
|
|
Describe the mechanism of hypersensitivity to penicillin |
Type I hypersensitivity (or immediate hypersensitivity) is an allergic reaction provoked by reexposure to penicillin is presented to CD4+ Th2 cells specific to the antigen that stimulate B-cell production of IgE antibodies also specific to the antigen. IgE instead of IgA, IgG, or IgM is secreted making it differ to normal immune response. The principal effects of these products are vasodilation and smooth-muscle contraction. |
|
|
Define DM |
A group of disorders characterised by persistently raised blood glucose. - has different causes most linked with the a reduction in the production of insulin |
|
|
Why can obesity result in type 2 DM and how can losing weight treat type 2 diabetes |
•Studies suggest that abdominal fat causes fat cells to releases ‘pro-inflammatory’ chemicals, which can make the body less sensitive to the insulin it produces by disrupting the function of insulin responsive cells and their ability to respond to insulin. •This is known as insulin resistance - a major trigger for type 2 diabetes. •Having excess abdominal fat (i.e. a large waistline) is known as central or abdominal obesity, a particularly high-risk form of obesity •The links between obesity and type 2 diabetes are firmly established - without the intervention of a healthy diet and appropriate exercise, obesity can lead to type 2 diabetes over a relatively short period of time. •The good news is that reducing your body weight, by even a small amount, can help improve your body's insulin sensitivity and lower your risk of developing cardiovascular and metabolic conditions such as type 2 diabetes, heart disease and types of cancer. •According to the NHS, a 5% reduction in body weight followed up by regular moderate intensity |
|
|
List chronic complications of diabetes |
•Polyuria •Polydipsia •Polyphagia •Unexplained weight loss •Blurred vision •Fatigue •ketoacidosis |
|
|
What is the relationship between NSAIDs and diabetes |
People with type 2 diabetes should avoid NSAIDs where possible. Reduced renal function and albuminuria are both risk factors for micro and macrovascular complications that have increased prevalence in people with diabetes. Preservation of renal function to prevent the development of CKD and to reduce cardiovascular risk is an essential part of the management of patients with type 2 diabetes. |
|
|
What is gestational Diabetes |
Gestational diabetes is a type of diabetes that affects women during pregnancy. Normally, the amount of glucose in the blood is controlled by a hormone called insulin.However, during pregnancy, some women develop higher than normal levels of glucose in their blood, which insulin can't bring under control.Gestational diabetes usually develops in the third trimester (after 28 weeks) and usually disappears after the baby is born. However, women who develop gestational diabetes are more likely to develop type 2 diabetes later in life. |
|
|
List the oral features of diabetes |
Periodontal disease, oral infection, altered saliva quality and quantity, sialosis (enlarged asymptomatic gland), oral dysaesthesias, CN abnormalities, delayed wound healing, adverse drug reaction, xerostomia due to microvascular disease and dehydration, candida, altered taste due to metformin. |
|
|
Discuss the epidemiology of Oral Cancer |
Common - smoking and alcohol consumption Rising - increased surveilance |
|
|
List 2 main risk factors for oral cancer |
Smoking and alcohol |
|
|
Other than smoking and alcohol list other risk factors for oral cancer |
Infections - HPV, HIV, HHV8 - kaposi's GvHD Immunodeficient states Less than 11 teeth in the mouth betel nut and areca nut [paan] occupation pre-cancer lesions UV Previous oral cancer Dietary genetics |
|
|
During the clinical examination discuss the clinical changes associated with oral cancer |
wt loss/ unexplained pain/ enlarged lymph nodes/ bleeding / new lesiosn/ changes to lesions/ persistent lesions [3weeks]/ erythroplakia/ mixed red white lesions/ white lesions/ trismus/ movement of teeth/ fixation/ exophytosis - mass, lump, growth / necrosis/ neuropathy |
|
|
Describe the information necessary to include when referring a patient for suspected oral cancer |
Relevant information: Size and site of lesion Appearance Duration Any ‘hard’ signs, e.g. neuropathy, otalgia PMH Risk factors Psychosocial issues |
|
|
Discuss the process that occurs when the patient is referred |
History and examination Flexible nasendoscopy Incisional biopsy OPT MRI Head and Neck CT Thorax MDT then treatment 31/62 day targets |
|
|
Tumour sizings Tx, T0, Tis, T1, T2, T3 |
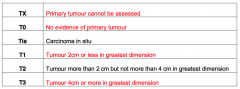
|
|
|
Define the term cyst |
A pathological cavity filled with liquid, semi liquid or gas may or may not be epithelial lined - not caused by the accumulation of pus. |
|
|
Lisst 4 clinical features of a cyst |
|
|
|
List 4 radiographic features of a cyst |
1. well corticated - slow growing 2. radiolucent 3. resporption of adjent teeth (maybe) 4. Displacement of adjacent structures - neurovasucalar bundle or teeth. |
|
|
Define enuclation and give advantages and disadvantages |
Surgical removal of the whole cyst and it’s lining The whole specimen is sent for pathologyIt is the default treatment for smaller cysts Advantages: •It is a one-stage treatment so avoids repeated procedures Disadvantages: •It may risk damage to adjacent structures •Risk of infection and wound-breakdown higher for very large cysts |
|
|
Define Marsupialisation and give advantages and disadvantages |
Removal of a window of mucosa/bone overlying the cystOpening of the cyst cavity in the mouth possibly eliminates the hydrostatic forces which cause cyst expansion.Cyst shrinks over time, enucleation can then be performed Advantages •Much simpler, can even be done with LA •Protects adjacent structures •Enables some unerupted teeth to be preserved Disadvantages •Wound needs to be packed / a bung placed in the hole •Patient compliance has to be excellent to maintain a clean cavity •Infill of cyst cavity is slow (prolonged treatment (up to 2y)) •Second procedure is required for enucleation |
|
|
List 3 causes of non-recurrent oral ulceration |
Infections e.g. HSV, HIV, TB, Syphilis etc Physical trauma Iatrogenic e.g. Medications nicorandil Recreational drugs / Chemical burn e.g. aspirin placed against oral mucosa Malignancy |
|
|
Define Sjogren's syndrome |
A chronic autoimmune condition characterized by degeneration of the salivary and lachrymal glands, causing dryness of the mouth and eyes |
|
|
Discuss the pathogenesis of Sjogren's |
• Multifactorial - contributory factors include: – Glandular destruction & lymphocyte infiltration; – Lymphadenopathy; – Production of abnormal saliva; – Lymphoma in a minority. • Swelling can be acute or chronic:– Depending upon the cause. |
|
|
Differentiate between primary and secondary Sjogren's |
Primary – xerostomia / keratoconjuctivitis sicca (KCS) Secondary - xerostomia / keratoconjuctivitis sicca (KCS) / chronic inflammatory connective tissue disease e.g. RA, SLE, PBC |
|
|
Patients with sjogrens are at an increased risk of developing what life threatening disease? |
Non –Hodgkin’s Lymphoma |
|
|
List 4 non-exocrine symptoms of sjogren's |
• Generalised fatigue;– This can be severe & extremely debilitating. • Inflammatory vascular disease:– Skin, muscle, joints, serosa, CNS/PNS. • Raynaud’s phenomenon; • Thyroiditis; • Anaemia; • Features of other associated autoimmune diseases in secondary Sjögren’s Syndrome |
|
|
Define Infective endocarditis
|
Infection of endocardium (the inner lining of the heart) by: – Bacteria (including some found in the mouth); or – More rarely other micro-organisms. With Inflammation • That leads to tissue damage and decreased cardiac function: – Particularly related to heart valve damage; and – Physical effects of related infected vegetations. |
|
|
List systemic features of infective endocarditis |
Fever Infective emboli transfer infective foci to distant sites Immune complex-mediated disease. |
|
|
Name factors in a patients MH that put the patient at increased risk of infective endocarditis |
– A past history of infective endocarditis – Prosthetic heart valves – Selected heart diseases as defined in current guidelines - Infective endocarditis may occur in the absence of any recognised predisposing cardiac lesions |
|
|
Describe the role and rationale that denstistry plays in infective endocarditis |
Surgical wounds and oral bacteria (viridans group streptococci) Oral bacteria in the bloodstream Oral bacteria infect compromised epithelium Infective endocarditis |
|
|
Discuss the guidelines surrounding IE prophylaxis and dentistry |
Guidelines reflect: – Analyses of the available information: • Quality clinical evidence unavailable; • Required clinical trials cannot be undertaken. – Expert opinion – less so than in the past. • Guidelines vary around the world:– Increasing consensus. • Guidelines change with time:– Guidelines first formulated >50 years ago. • Guidelines take consideration of: – Different predisposing lesions; – Previous antibiotic exposure; – Procedures to be undertaken. • U.K. guidelines were clarified in 2008:– NICE review Don't give Antibiotic prophylaxis - more likely to have anaphylaxis from the antibiotics. |
|
|
Define the term trigeminal neuralgia |
Chronic pain associated with the trigeminal nerve - even stimulus that would usually not be noxious can provide excruciating pain. Assoc. with microcompression, demyelination, neoplasms and athersclerosis. |
|
|
List 4 characteristics that pain assoc. with TN must inhibit to be considered TN. |
Distribution – one or more divisions of trigeminal nerve Sudden, intense, sharp, superficial, stabbing or burning quality Pain intensity severe Precipitation from trigger areas or by certain daily activities (eating, talking, brushing teeth...) Between paroxysms the patient is entirely asymptomatic |
|
|
Discuss the aetiology of TN |
Microcompression - local demyelination and altered neuronal processing of the trigeminal nerve root as it enters the pons; –Superior cerebellar artery is the commonest cause; –Neoplasms ~ uncommon but occur. •Demyelinating diseases: –Multiple sclerosis. |
|
|
Consideration must be given to what medical condition if an adult under the age of 40 has classical TN? |
Multiple sclerosis |
|
|
How is a diagnosis of TN made? |
Pain will go away when LA administered Does not fit any other conditions - e.g pains of dental origin MRI scan for trigem nerve root compression and associated artery/ neoplasm for MS CT - for base of skull neoplasm |
|
|
Discuss the medical management of TN |
• Primarily anti-convulsants – e.g. Carbamazepine • Support Groups - Liked by some patients –Trigeminal Neuralgia Association Alternate drugs e.g. Oxcarbazepine / Lamotrigine / Baclofen / Phenytoin / Sodium Valproate •T.N. relapses and remits, so the patient may be able to enjoy ‘drug holidays’ •If pain free for 3 months–The dose can be slowly tapered down •But most have to restart medication when the symptoms return–May need higher dose than before |
|
|
List 2 surgical methods of management of TN |
–Microvascular decompression of the nerve root –Nerve destruction. |