![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
Endodontic |
- Recognized in 1963 - Manages the prevention, diagnosis, and treatment of the dental pulp and the periradicular tissues that surround the root of the tooth - Also referred to as root canal therapy - Provides an effective means of saving a tooth that might otherwise have to be extracted *Removal of the dental pulp and filling of the canal with material - Additional 3 yrs of experience of clinical skill and research of pulp therapy |
|
|
Periradicular |
Refers to the area of the nerve, blood vessels and tissues that surrounds the root of a tooth |
|
|
Endodontic |
- Also referred to as root canal therapy - Provides an effective means of saving a tooth that might otherwise have to be extracted - *Removal of the dental pulp and filling of the canal with material |
|
|
Endodontist |
- A dentist who specializes in the prevention, diagnosis, and treatment of diseases of the dental pulp and the periradicular tissues - Training for a minimum of 3 yrs in clinical skills and research of pulp therapy |
|
|
Two Causes of Pulpal Damage |
Main sources of damage are physical irritation and trauma |
|
|
Physical Irritation |
- Can range from mild tooth sensitivity to complete nerve death of the tooth or even infection of the surrounding tissues - When bacteria rach the nerves and blood vessels, infection can result in an abscess, which is a localized area of pus |
|
|
Trauma |
- Blow to a tooth or jaw, can cause damage to surrounding tissues - Overtime, this damage can affect the nerve tissue and blood vessels of the pulp |
|
|
Abscess |
Localized area of pus orginating from an infection |
|
|
Pulpal Damage Symptoms |
- Sensitivity, discomfort and pain may be symptoms of pulpal nerve damage -Most common types of signs and symptoms: - Pain when occluding - Pain during mastication - Sensitivity to hot or cold beverages - Noticeable facial swelling - Fever - Tenderness of the surrounding gums - Cracked or discolored teeth |
|
|
Subjective Examination |
- Evaluation of symptoms or problems described by the patient, which include the following: - Chief complaint - Character and duration of pain - Painful stimuli - Sensitivity to biting and pressure |
|
|
Objective Examination |
- Conducted by the endodontist, who evaluates the status of the tooth and surrounding tissues - Extent of decay - Periodontal conditions - Presence of an extensive restoration - Tooth mobility - Swelling or discoloration - Pulp exposure |
|
|
Control Tooth |
Healthy tooth used as a standard to compare questinable teeth of similar and structure during pulp vitality testing |
|
|
Percussion |
- Examination technique that involves tapping on the incisal or occlusal surface of a tooth to assess vitality with the end of the mouth mirror handle, which is held parallel to the long axis of the tooth - Determine whether the inflammatory process has extended into the periapical tissues - Positive response to these test indicates that inflammation is present in the periodontal ligament and that endodontic treatment is most likely required |
|
|
Palpation |
- Touching or feeling for abnormalities within soft tissue - Applying firm pressue to the mucosa above the apex of the root and noting any sensitivity or swelling |
|
|
Thermal Sensitivity |
- Determines the status of the pulp - Never used on a metallic restoration or on gingival tissue |
|
|
Cold Test |
- DDS uses ice, dry ice, or carbon dioxide to evaluate the response of a tooth to cold - First, the control tooth and the suspect tooth are isolated and dried - Second, source of cold is applied first to the cervical area of the control tooth, then to the cervical area of the suspect tooth |
|
|
Necrotic Pulp |
Will not respond to cold |
|
|
Irreversible Pulpitis |
When the cold relieves the pain, however cold in teeth with this also can initiate severe, lingering pain |
|
|
Heat Test |
Least useful of the vitality test because a painful response to heat could indicate either reversible pulpitis or irreversible pulpitis |
|
|
Gutta-Percha |
- Plastic type of filling material used in endodontics - A small (pea-sized) piece of this isheated in a flame and then applied to the facial surface of the tooth - Another method is to heat the instrument and place on the tooth - Apply petroleum Jelly to tooth surface before testing to prevent material from sticking |
|
|
Electric Pulp Testing |
- Used in endodontic diagnosis to determine whether a pulp is vita or nonvital - Can produce a false-positive or a false-negative response - Therefore, test results must be supported by other diagnosis findings - Deliver a small electrical stimulus to the pulp |
|
|
Nonvital |
Not living, as in oral tissue and tooth structure |
|
|
Factors that influence the reliability of the pulp tester |
- Teeth with extensive restorations can vary in response - Teeth with more than one canal can have one vital canal and other nonvital canals - A failing pulp can produce a variety of responses - Control teeth may not respond as anticipated - Moisture on the tooth during testing may produce an inaccurate reading - The batteries in the tester may weaken over time |
|
|
Initial Radiograph |
PA is taken during diagnostic stages before treatment |
|
|
Working Length Image |
- PA is taken once the pulp has been opened - Used to determine the length of the canal - Easier to detect canal length with the file remaining in the tooth |
|
|
Final Instrumentation Image |
PA is taken with the final size files in all canals receiving treatment |
|
|
Root Canal Completion Image |
Final PA is taken of the completed canal filled after the tooth has been temporized and the dental dam is removed |
|
|
Recall Image |
PA images is taken at posttreatment evaluations |
|
|
Requirements of Rad Images |
- Show 4 - 5 mm beyond the apex of the tooth and the surrounding bone or pathologic conditions - Present an accurate image of the tooth without elongation or foreshortening - Exhibit good contrast so that all pertinent structures are readily idenfiable |
|
|
Normal Pulp |
- No subjective symptoms or objective signs - Tooth responds normally to sensory stimuli and the healthy layer of dentin surrounds the pulp |
|
|
Pulpitis |
- Pulpal tissues have become inflamed - Can be describe clinically as: - Reversible Pulpitis - Irreversible Pulpitis |
|
|
Pulpitis |
Inflammation of the dental pulp |
|
|
Reversible Pulpitis |
- Form of pulpal inflammation in which the pulp may be salvageable - Occurs when the pulp is irritated and the patient is experiencing pain to thermal stimuli - Eliminating the irritant and placing a sedative material may save the pulp |
|
|
Irreversible Pulpitis |
- Infectious condition in which the pulp is incapable of healing, which would then require root canal therapy - Display symptoms of lingering pain - Pulp is incapable of healing and will indicate root canal therapy or extraction as the only treatment options |
|
|
Periradicular Abscess |
Inflammatory reaction the pulpal infection |
|
|
Chronic |
Pertaining to diease symptoms that persist over a long time |
|
|
Chronic Periradicular Abscess |
- Presence of a draining sinus tract - Lesion is asymptomatic, with little or no discomfort, and an intermittent discarhge iof pus may be noticed |
|
|
Acute |
Pertaining to a traumatic pathologic, or physiologic occurrence of process that has a short and relatively sever course |
|
|
Acute Periradicular Abscess |
An inflammatory response with pain, tenderness of the tooth to pressure, pus formation, and swelling of the tissue resulting from necrosis |
|
|
Periodontal Abscess |
- Inflammatory reaction to bacteria trapped in the periodontal sulcus - Patient will experience rapid onset, pain, tenderness of the tooth to pressure, pus formation and swelling |
|
|
Periradicular Cyst |
- Cyst that develops ar or near the root of a necrotic tooth - Develop as an inflammatory response to pulpal infection and necrosis of the pulp |
|
|
Pulp Fibrosis |
- Decrease of living cells within the pulp, causing fibrous tissue to take over the pulpal canal - Seen in older patients, as well as in patients with traumatic injury to a tooth |
|
|
Necrosis |
- Also referred to as necrotic or nonvital, used to describe a tooth that does not respond to sensory stimulus - Although tooth may be considered "nonvital" tooth continues to be attached to the alveolus by way of the cementum and periodontal ligaments, which are still vital tissues |
|
|
Pulpal Therapy |
- An attempt to stimulate pulpal regenration and save the pulp - When it is not effective, the endodontist will move to more extreme measures, which can include root canal therapy or surgery |
|
|
Pulp Capping |
An attempt to save the pulp, a covering of calcium hydroxide is placed over an exposed or nearly exposed pulp to encourage the formation of new dentin at the site of injury |
|
|
Indirect Pulp Cap |
- Placement of a medicament over a partially exposed pulp - Temporary procedure where most of the carious dentin in a deep cavity is not removed - Liner and a temporary restoration are placed and the cavity is reopened after a period of time; the remaining carious dentin is then excavated - Goal: to give the pulp a chance to form more dentin beneath the carious dentin, so that pulp exposure can be avoided Aims of Treatment: 1. Promote puppal healing by removing most of the decay 2. Stimulate the production of reparative dentin through placement of calcium hydroxide |
|
|
Direct Pulp Cap |
- Application of dental material with an exposed or nearly exposed dental pulp - Procedure that is indicated when the pulp has been partially exposed - Tooth is still vital - Calcium hydroxide or an adhesive resin that is naturally compatible with pulpal tissue is placed to allow healing - Periodic monitoring is necessary |
|
|
Pulpotomy |
- Removal of the coronal portion of a vital pulp from a tooth - Involves removal of the coronal portion of an exposed vital pulp - Procedure is completed to preserve the vitality of the remaining portion of the pulp within the root of the tooth - Indicated for vital primary teeth, teeth with deep carious lesions, and emergency situations |
|
|
Pulpectomy |
- Complete removal of vital pulp from a tooth - Also referred to as root canal therapy, involves complete removal of the dental pulp |
|

Endodontic Explorer |
Endodontic Explorer - Double-ended, long and straight - Working ends are positioned at an angle to the handle that is unique to this instrument, which helps in locating canal openings |
|

|
Endodontic Spoon Excavator Double ended, very long shank which allows it to reach deep into the canal to remove coronal pulp tissue, decay, and temporary cements |
|

|
Spreaders - Used in the obturation of the canal - Condsense and adapt the gutta-percha points into the canal - Look similar but differ at the tip - Have a pointed tip, similar to that of an explorer |
|
|
Pluggers - Have a flat tip that of a condenser - Condenses the gutta percha |
|
|
Obturation |
Process of filling a root canal |
|

|
Glick Number 1 - Paddle shaped end designed for placement of temporary restorations, and the rod-shaped plugger at the opposite end is ideal for removal of excess gutta-percha - Plugger is graduated at 5mm increments and can be heated for placement or removal of gutta-percha |
|
|
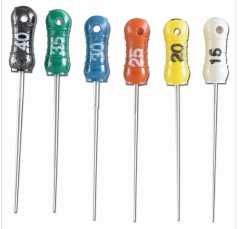
Hand-Operated Files |
- Used for cleaning and shaping pulp canal - Each file designed for a specific function once placed in the canal - FIles are color-coded according to size |
|

|
Ni-Ti files Advantages 1. Extreme flexibility, which enables them to better follow the contour of the canal 2. Good strength, which is an important safety factory in keeping the instrument from breaking while in the canal 3. Longer working life |
|

|
K-type File - Twisted design and is used to clean out of the canal and during later stages of shaping and contouring the canal - Conventional has a "stiff" feel that is very effective for straight canals - Narrow canals and curved canals, some DDS prefer flexible K-type File |
|

|
Hedstrom File - Greater cutting efficiency because of its design - Used for final enlargement of the canal when pulling outwards - Has its spiral edges arranged so that cutting occurs only on the pulling stroke, making the dental walls smooth and easier to fill |
|

|
Reamer File - Similar in design to the K-type file, but its cutting edges are farther apart - To remove dentin structure and to smooth and increase size of the canal |
|
|
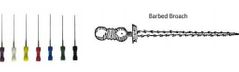
Broaches - Thin, flexible, tapered metal - Have tiny fishhook-like projections along the shaft that are used to remove vital, inflamed hemorrhagic pulp tissue from the canal - Not as frequently used as other files - Used to remove objects such as cotton pellets and paper joints - Should be discarded after a single use because of their fragile makeup |
|
|
Rotary-Operated Files and Burs |
- Similar to hand files but are latch-type placed in a high-torque, low-rpm handpiece designed for Ni-Ti rotary instrument - Popular because of their makeup, ease of use, and efficiency |
|
|
Gray Handle Color |
Diameter: 08 |
|
|
Purple Handle Color |
Diameter: 10 |
|
|
White Handle Color |
Diameter: 15-45-90 |
|
|
Yellow Handle Color |
Diameter: 20-50-100 |
|
|
Red Handle Color |
Diameter: 25-55-110 |
|
|
Blue Handle Color |
30-60-120 |
|
|
Green Handle Color |
Diameter: 35-70-130 |
|
|
Black Handle Color |
Diameter: 40-80-140 |
|

Gates-Glidden Burs |
- Also known as Gates-Glidden drills - Football-shaped working end with a very long shank - Burs designed to have the cutting edge on the sides, not on the end, to enlarge the walls of the pulp chamber - Used in handpiece with a latch-type attachment and are operated in a clockwise direction |
|

Pesso Files |
- Also known as Pesso Reamers - Work in the same manner as Gates Glidden burs, but are shaped slightly different to have their blades long and parallel with the noncutting ends - Used when tooth requires a port preperation for placement of the final restoration |
|
|
Rubber Stops |
- Ancillary Instrument - A stop is a small, color-coded, round piece of rubber, silicone, or plastic that is slid onto hand-operated files to prevent perforation of the apex of the tooth during instrumentation - Lengths of the files are carefully measured on a rad and the stop is placed precisely at the predetermined working length of the canal |
|
|
Perforation |
Making a hole, as in breaking through and extending beyond the apex of the root |
|
|
Paper Points |
- Ancillary Instruments - Sterile absorbent pieces of paper rolled into long, narrow points - Held with locking pliers and is insterted into the canal to absorb the irrigating solution and to dry the canal - Procedure is repeated with a fresh point until a paper point is completely dry when removed from the canal - Sterile paper is available in a variety of sizes ranging from fine to coarse |
|
|
Microscopic Endodontics |
- Move efficient, effective, and patient-friendly endodontic procedure - Beneficial from diagnosis, to the location of canals or missed canals, for cleaning and shapin the canal, and to the filling of the canal - Can be completed in less time because of the greater visibility of the root canal anatomy with the final product having reduced procedural errors |
|
|
Operating Microscope Accomplishes 3 Objectives |
Magnification - Acts like binoculars, allowing the endoddontist to view the pulpal canal in a magnification mode Illumination - light from a 100 - watt halogen bulb illuminates the canal, with the light intensity controlled by a rheostat and cooled by a fan Addition of accesories - LCD monitor and a video camera for visualization and documentation |
|
|
Irrigation Solutions |
- Irrigating the canal facilitates the removal of materials from the canal and provides tissue dissolution, bleaching, deodorizing, and hemorrhage control - The following solutions are used: - Sodium Hypochlorite - Hydrogen Peroxide - Parachlorophenol (PCP |
|
|
Sodium Hypochlorite |
- Commonlu known as household bleach, diluted with equal parts of sterile water for use as an irrigation solution - A 5- to 6-ml disposable plastic syringe with a special 27-gauge needle is used - Antimicrobial agent that has a solvent action on necrotic pulp tissue and organic debris - Must be used with caution because a bleach solution causes skin irritation, and drips or splashes can ruin the patient's clothing |
|
|
Hydrogen Peroxide |
Clear, colorless liquid with disinfectant and bleaching properties for endodontics |
|
|
Parachlorophenol (PCP) |
Coroless, crytalline toxic phenol compound that is used as an antimicrobial agent for disinfection of the pulp canal |
|
|
Root Canal Filling Materials |
- Gutta-percha points are made from a rubber material taken from the Palaquium gutta true - Organic subs that is solid at room temperature and becomes soft and pliable when heated - Used to obturate the pulpal canal after treatment has been completed - Radiopaque and supplied in various size and used with a sealer (color coded with file size) - Made to flow in the pulpal canal with the use of heat or solvent - Melts when heated above 140 degree can be condensed with the use of an electronic heated spreader |
|
|
Root Canal Sealers |
- Cement-type material that seals out the unfilled voids during the obturation process - Several cements can be used as a sealer for root canal therapy, including calcium hydroxide, zinc oxide eugenol and glass ionomers - These materials undergo very little shrinkage - Must be easy to place, radiopaque, nonstaining to the teeth, bacteriostatic, gentle on the periapical that surround them, and able to resist moisture |
|
|
Types of Root Canal Sealers: Calcium Hydroxide Sealers |
- Sealapex - CRCS - Apexit |
|
|
Types of Root Canal Sealers: Resin Composite Sealer |
- Epipheny - Endorez |
|
|
Types of Root Canal Sealers: Glass Ionomer Cement |
Ketac Endo |
|
|
Formocresol |
- Mixture of formaldehyde and cresol in a water-glycerin base - Type of solution was used as an intracanal medicament for the pulpotomy of primary teeth - Bc concerns about its toxic effects, it is not recommended for use |
|
|
Anesthesia and Pain Control |
- For endodontic treatment they use infiltration for maxillary teeth and nerve block for mand teeth - Local anesthetic agent is administered any time vitality remains in the tooth to be treated - If tooth is nonvital, local anesthetic is not necessary - Tissue should not be inflammed when administering anesthetic because it would be harder to get to the pulp |
|
|
Isolation and Disinfection |
- Endodontic treatment requires the use of a dental dam - Once dental dam is placed, it is necessary to disinfect the tooth, dental clamp and surrounding dental dam material with the use of iodine solution or a sodium hypochlorite solution |
|
|
Problems that result from inaccurate measurement of length: |
1. Perforation of the apex 2. Overinstrumentation or underinstrumentation of canal length 3. Overfilling of underfilling of the canal 4. Posoperative pain |
|
|
Estimated Working Length |
- Bc the exact apex locations vary and because these variation are not always visible on radiographs, the working length is assessed - Determine by selecting a reference point on the tooth, usually the highest point on the incisal or occlusal surface |
|
|
Electronic Apex Locator |
- Supplemental technique that can be used to facilitate identification in the apex of the root canal - Aid to endodontic therapy can reduce the number of diagnostic radiographs required for working length determination - Determine working length, location of the apical forament is identified more accurately than when radiographs are used alone |
|
|
Debridement and Shaping of the Canal |
- To remove or clean out the pulpal canal Purposes: 1. Remove bacteria, necrotic tissue and organic debris from the root canal 2. Smooth and shape the canal so that the filling material can be completely adapted to the walls of the canal |
|
|
Obturation |
- When the canal is now ready for obstruration or to be filled by the endodontist - The objective is to place a fluid-tight seal in the canal from apical tip to the coronal surface, to prevent the reentry of micro-organisms - If the tooth has more than one canal, each canal is filled individually, with each canal requiring a properly fitted and sealed gutta-percha point |
|
|
Surgical Endodontics |
- Successful approx. 90-95% - Exceptional situations, however is must be used to save a tooth from extraction - Indications for surgical intervention include: 1. Endodontic Failure 2. Exploratory Surgery 3. Biopsy |
|
|
Endodontic Failure |
Failure of nonsurgical endodontics may be caused by persistent infection, severely curved roots, perforation of the canal, fractured roots, extensive root resorption, pulp stones, or accessory canals that cannot be treated |
|
|
Exploratory Surgery |
- Surgery may be necessary to determine why healing has not occurred after root canal therapy - Canal medications that extend beyond the apex and into the periapical tissues may be the cause |
|
|
Biopsy |
A tissie sample may be required |
|
|
Apicoectomy |
- Surgical removal of the apical portion of the tooth through a surgical opening made in the overlying bone and gingival tissues - Surgical removal of the apical portion of the root with the use of a tapered fissure bur in a high-speed handpiece Dentist can examine the apex for signs of: 1. Inadequate sealing of the canal 2. Accessory (additional) canals 3. Fractures of the root |
|
|
Apical Curettage |
- Surgical removal of infectious material surrounding the apex of a root - Once the endodontist has entered the apical area of a tooth, this may be required to remove the pathologic soft tissue around the root apex - Curretage means the removal of diseased tissue by scraping with a curette |
|
|
Retrograde Restoration |
- Small restoration placed at the apex of a root - Also referred to as root end filling - Completed when the apical seal is not adequate - Small preparation is made at the apex and is sealed with filling materials such as gutta-percha, amalgam, or composite |
|
|
Root Amputation |
- Removal of one or more roots without removal of the crown of the tooth - Amputation occurs at the point at which the root joins the crown - Most often performed on maxillary molars |
|
|
Hemisection |
- Surgical seperation of a multirooted tooth through the furcation area - Procedure in which the root and the crown are cut lenghwise and removed - Often performed on mand molars |