Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
147 Cards in this Set
- Front
- Back
|
What does the mnemonic FEGNOMASHIC stand for?
|
-Fibrous dysplasia
-Enchondroma and Eosinophilic granulmoma -Giant cell tumor -Nonossifying fibroma -Osteoblastoma -Metastatic diseases and myeloma -Aneurysmal bone cyst -Solitary bone cyst -Hyperparathyroidism (brown tumor) -Infection -Chondroblastoma and chondromyxoid |
|
|
What are the distinguishing characteristics of fibrous dysplasia?
|
No periosteal reaction
|
|
|
What are the distinguishing characteristics of enchondroma?
|
-Calcification present (except in phalanges)
-Painless (no periostitis) |
|
|
What are the distinguishing characteristics of eosinophilic granuloma?
|
Younger than age 30
|
|
|
What are the distinguishing characteristics of giant cell tumor?
|
-Epiphyses closed
-Abuts the articular surface (in long bones) -Well defined with a nonsclerotic margin (in long bones) -Eccentric |
|
|
What are the distinguishing characteristics of nonossifying fibroma?
|
-Younger than age 30
-Painless (no periostitis) -Cortically based |
|
|
What are the distinguishing characteristics of osteoblastoma?
|
Mentioned when aneurysmal bone cyst is mentioned (especially in the posterior elements of the spine)
|
|
|
What are the distinguishing characteristics of metastatic diseases and myeloma?
|
Older than age 40
|
|
|
What are the distinguishing characteristics of aneurysmal bone cyst?
|
-Expansile
-Younger than age 30 |
|
|
What are the distinguishing characteristics of solitary bone cyst?
|
-Central
-Younger than age 30 |
|
|
What are the distinguishing characteristics of hyperparathyroidism?
|
Must have other evidence of hyperparathyroidism
|
|
|
What are the distinguishing characteristics of infection?
|
Always mention
|
|
|
What are the distinguishing characteristics of chondroblastoma?
|
-Younger than age 30
-Epiphyseal |
|
|
What are the distinguishing characteristics of chondromyxoid?
|
No calcified matrix
|
|
|
What is fibrous dysplasia?
|
Benign congenital process that can be seen in a patient of any age and can look like almost anything on imaging.
|
|
|
What does fibrous dysplasia look like on imaging?
|
-There’s no periosteal reaction (big distinguisher)
-It can be wild looking, discretely lucent, patchy, sclerotic, expansile, multiple, etc. |
|
|
Does fibrous dysplasia undergo malignant degeneration?
|
Almost never
|
|
|
Does fibrous dysplasia cause pain?
|
Not unless there’s a fracture
|
|
|
Do fractures occur with fibrous dysplasia?
|
They can in long bones that bear weight, otherwise, no.
|
|
|
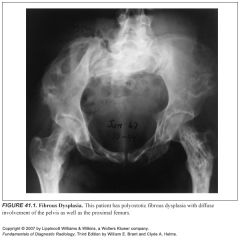
Is fibrous dysplasia monostotic or polyostotic?
|
It can be either, but is more commonly monostotic
|
|
|
Where in the body does fibrous dysplasia tend to occur?
|
Pelvis, proximal femur, ribs, skull
|
|
|
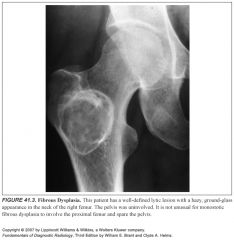
If fibrous dysplasia is in the pelvis, where else should you always see it?
|
The ipsilateral proximal femur
|
|
|
What does fibrous dysplasia look like in the ribs?
|
It typically has an expansile, lytic appearance in the posterior ribs and a sclerotic appearance in the anterior ribs.
|
|
|
Is fibrous dysplasia lytic or blastic?
|
-You can see both BUT
-It is often purely lytic and becomes hazy or takes on ground-glass look as the matrix calcifies -It can go on to calcify significantly, and then it presents as a sclerotic lesion |
|
|
What is an adamantinoma?
|
A malignant tumor that radiographically and histologically resembles fibrous dysplasia
|
|
|
Where does adamantinoma occur?
|
-Almost exclusively in the tibia and the jaw (it’s unknown why)
-So if you see fibrous dysplasia in the tibia or jaw, bring up the possibility of adamantinoma (but it’s super rare) |
|
|
Describe McCune-Albright syndrome:
|
-Polyostotic fibrous dysplasia with café-au-lait spos and precocious puberty
-Fibrous dysplasias tend to occur unilaterally—along one half of the body |
|
|
Describe cherubism:
|
-Multiple fibrous dysplasia lesions in the jaw
-These lesions regress in adulthood |
|
|
Where do enchondromas occur?
|
In any bone formed from cartilage
|
|
|
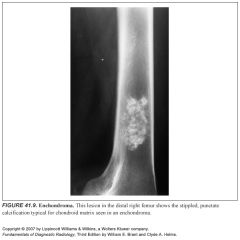
What do enchondromas look like on imaging?
|
-They may be central, eccentric, expansile, or nonexpansile
-They invariably contain calcified chondroid matrix, except when in the phalanges |
|
|
What is the most common benign cystic lesion in the phalanges?
|
An enchondroma is the most common benign cystic lesion in the phalanges
|
|
|
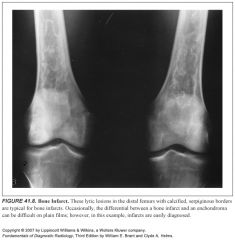
What can enchondroma look like?
|
A bony infarct
|
|
|
How can you tell the difference between an enchondroma and a bony infarct?
|
-An infarct usually has a well-defined, densely sclerotic, serpiginous border. An enchondroma doesn’t.
-An enchondroma often causes endosteal scalloping; infarcts don’t. |
|
|
How can you tell an enchondroma from a chondrosarcoma?
|
-It is almost impossible, even on pathology
-Pain in an apparent enchondroma should be suspicious -Periostitis should not be seen in an enchondroma either |
|
|
What is the condition of multiple enchondromas called?
|
Ollier’s disease
|
|
|
Describe Ollier’s disease:
|
-Multiple enchondromas
-It is not hereditary -There is no increased rate of malignant degeneration of the enchondromas |
|
|
What if there’s multiple enchondromas and soft tissue hemangiomas?
|
It’s called Mafucci syndrome
|
|
|
Describe Mafucci syndrome:
|
-Multiple enchondromas and soft tissue hemangiomas
-It is not hereditary -There is an increased incidence of malignant degeneration of the enchondromas |
|
|
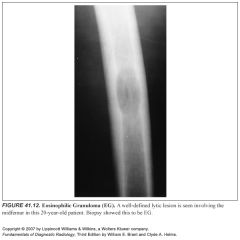
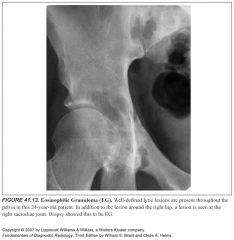
What is an eosinophilic granuloma?
|
It is a form of histiocytosis X
|
|
|
What are the other forms of histiocytosis X besides eosinophilic granuloma?
|
-Letterer-Siwe disease and Hand-Schuller-Christian disease
-The bony manifestations of all forms are similar, so they’re called eosinophilic granuloma |
|
|
What does eosinophilic granuloma look like on imaging?
|
-It can be lytic or sclerotic, well defined or ill defined.
-It might or might not have a sclerotic border. -It may or may not ellicit periosteal reaction -If present, the periostitis is typically benign in appearance (thick, uniform, wavy), but can be lamellated or amorphous -EG can mimic Ewing sarcoma and it may be permeative (multiple small holes) -It is most often monostotic, but can be polyostotic |
|
|
What malignancy can EG mimic?
|
Ewing sarcoma
|
|
|
What should you always mention when describing bony lesions?
|
Always mention associated soft tissue mass when describing bony lesions, but know that this does not narrow the differential.
|
|
|
How can you distinguish EG from anything else?
|
-It is difficult to exclude it from any differential
-It occurs almost exclusively in patients under 30 years old (usually <20 years old). -You can add it to the differential without even looking at the image! |
|
|
Is EG normally monostotic or polyostotic?
|
It’s most often monostotic, but you still have to include it in the differential for multiple lesions in a young patient
|
|
|
What entities can have a bony sequestrum?
|
-EG
-Osteomyelitis -Lymphoma -Fibrosarcoma -Don’t forget that an osteoid osteoma can have the appearance of a sequestrum when the nidus is partially calcified |
|
|
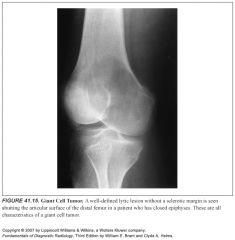
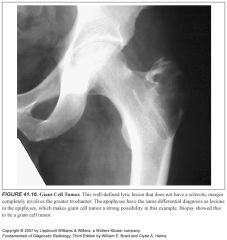
Is a giant cell tumor malignant or benign?
|
-You can’t tell, neither can pathologists
-Surgeons will curettage them and consider them benign unless they recur. -About 15% are thought to be malignant |
|
|
Where do giant cell tumors metastasize to?
|
The lungs (infrequently)
|
|
|
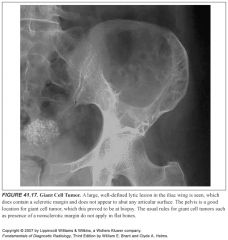
What are the four rules of giant cell tumors?
|
-They only occur in patients with closed epiphyses
-They are epiphyseal and abut the articular cartilage (the metaphysis also frequently has some the tumor in it because they are generally very large) This rule doesn’t apply in flat bones like the pelvis or in the apophyses -They are eccentrically located in the bone, not centrally placed in the medullary cavity -They must have sharply defined zone of transition (border), that is not sclerotic. This does not apply to flat bones or the calcaneus |
|
|
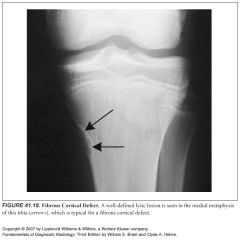
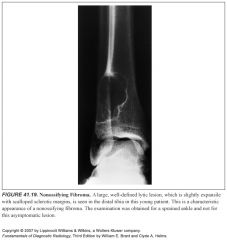
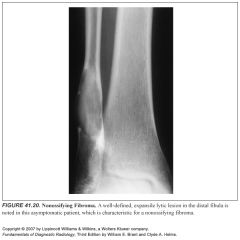
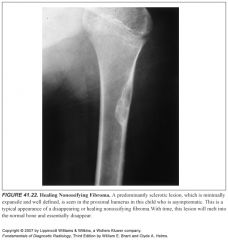
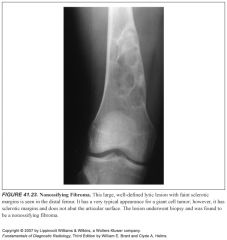
What is a nonossifying fibroma?
|
-Benign, asymptomatic lesions that typically occur in the metaphysis of a long bone, emanating from the cortex.
-They classically have a thin, sclerotic border that is scalloped and slightly expansile |
|
|
How many kids have a nonossifying fibroma?
|
Up to 20%
|
|
|
What is a nonossifying fibroma also called?
|
A fibrous cortical defect (some people call fibrous cortical defects lesions that are smaller than 2 cm in size, while NOF’s are larger than 2 cm)
|
|
|
So, what if you see an interruption of the cortex of an NOF on CT or MR?
|
This is merely cortical replacement by benign fibrous tissue, and should not warrant further investigation. This is NOT cortical destruction.
|
|
|
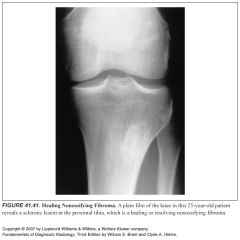
What do NOF’s look like on imaging (including nucs) while they’re healing?
When does this usually happen? |
-They develop sclerosis and eventually disappear
-This usually happens around ages 20-30 years -During this healing period, they can appear hot on radionuclide bone scan because there is osteoblastic activity |
|
|
Is there periostitis in NOF’s?
|
No, unless there is a history of trauma.
|
|
|
What if an NOF increases in size?
|
It shouldn’t alter the diagnosis, because these lesions can get quite large, grow, and change in size
|
|
|
Where do NOF’s usually occur?
|
Typically around the knee, occassionally multiple NOF’s can be around the knee.
|
|
|
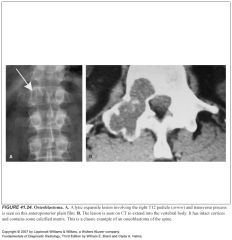
What do osteoblastomas look like on imaging?
|
Two types:
1:They look like large osteoid osteomas, often called giant osteoid osteomas 2:They look like aneurysmal bone cysts. If an ABC is being considered, so should an osteoblastoma. |
|
|
Where do osteoblastoma classically occur?
|
In the posterior elements of the vertebral bodies
|
|
|
What is the differential of an expansile lytic lesion of the posterior elements of the spine?
|
-Osteoblastoma
-Aneurysmal bone cyst -Tuberculosis |
|
|
When should you think about metastatic disease in bone lesions?
|
In ANY bone lesion, add this to the differential in any patient over 40
|
|
|
What do metastatic lesions look like?
|
Anything, they can appear perfectly benign
|
|
|
How does multiple myeloma usually present?
|
As diffuse permeative process in the skeleton
|
|
|
What is a plasmacytoma?
|
-Bubbly, lytic bone lesions of myeloma
-They occur in slightly younger patients (older than 35) -They can precede clinical or hematologic evidence of myeloma by 3 to 5 years |
|
|
What metastatic lesions tend to be lytic and expansile?
|
Thyroid and renal cell cancers
|
|
|
What do aneurysmal bone cysts look like on imaging?
|
-Aneurysmal or expansile
-On CT or MR, these lesions often have fluid-fluid levels (many other lesions have fluid-fluid levels too) |
|
|
What age group gets aneurysmal bone cysts?
|
Patients younger than age 30
|
|
|
Where in the skeleton can ABCs occur?
|
-Anywhere
-They often occur in posterior elements of the spine |
|
|
How do ABCs present?
|
Usually because of pain
|
|
|
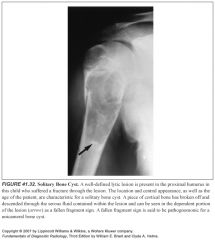
What are solitary bone cysts also called?
|
Simple bone cysts or unicameral bone cysts, although the are not necessarily unicameral (one compartment).
|
|
|
What is distinctive about unicameral bone cysts?
|
-They are one of the few lesions that do not occur most commonly around the knees
-They are the only lesion that is always central in location |
|
|
Where do UBCs tend to occur?
|
Two-thirds to three-fourths occur in the proximal humerus and proximal femur
|
|
|
How do UBCs tend to present?
|
-They are usually asymptomatic unless they fracture, which is frequently
-Even when they fracture, they rarely form periostitis |
|
|
What is a classic radiographic finding in UBCs?
|
-The fallen fragment sign
-This occurs when a piece of cortex breaks off after a fracture in a UBC and the piece of cortical bone sinks to the gravity-dependent portion of the lesion. -This indicates a fluid-filled cystic lesions, rather than a lesion filled with matrix |
|
|
Who gets UBCs?
|
Young patients (under 30)
|
|
|
Where do UBCs most commonly occur?
|
-Long bones, but they have been described in almost every bone in the body
-A fairly common location is in the calcaneus, where they have a characteristic location adjacent to the inferior surface of the calcaneus. |
|
|
How do UBCs evolve?
|
They begin at the physeal plate in long bones and grow into the shaft of the bone. They are not epiphyseal lesions.
|
|
|
What do brown tumors of hyperparathyroidism (HPT) look like?
|
They can have almost any appearance from a purely lytic, to a sclerotic process.
|
|
|
What do these tumors look like once a patient’s HPT gets treated?
|
They undergo sclerosis and will eventually disappear.
|
|
|
What do you need if you’re going to include HPT in the differential diagnosis?
|
Other radiographic findings of HPT should be seen.
|
|
|
What is pathognomonic for HPT?
|
Subperiosteal resorption. It should be searched for in the phalanges (particularly in the radial aspect of the middle phalanges), distal clavicles, medial aspect of the proximal tibias, and sacroiliac joints.
|
|
|
What do the physes look like in HPT?
|
If they’re open, they should have a frayed, ragged appearance, like rickets
|
|
|
What if you see osteoporosis or osteosclerosis in addition to findings of HPT?
|
-It is probably renal osteodystrophy with secondary HPT
-Subperiosteal resorption must be present, or HPT is not in the differential |
|
|
How do you rule out osteomyelitis?
|
You can’t
|
|
|
What is associated with osteomyelitis located near a joint?
|
A joint effusion, cartilage loss, or both
|
|
|
What imaging is routinely recommended when osteomyelitis is considered?
|
CT—to look for a sequestrum
|
|
|
Why is finding a sequestrum important in osteomyelitis?
|
Because it changes management, making surgery necessary
|
|
|
What are the big distinguishers for chondroblastoma?
|
-Only in the epiphyses
-In patients younger than 30 years old |
|
|
What is the differential for a lytic lesion in the epiphysis of a pt under 30 years old?
|
-Infection (most common)
-Chondroblastoma -Giant cell tumor -Always consider a subchondral cyst or geode if joint pathology is present |
|
|
Which four disease processes have subchondral cysts or geodes?
|
-Degenerative joint disease (must have joint space narrowing, sclerosis, and osteophytes)
-Rheumatoid arthritis -Pseudogout -Avascular necrosis |
|
|
What’s a differential for lytic lesions in the apophyses?
|
-Infection (most common)
-Chondroblastoma -Giant cell tumor |
|
|
Give a differential for lytic lesions near the carpal bones, the tarsal bones, and the patella:
|
-Infection (most common)
-Chondroblastoma -Giant cell tumor -Always consider a subchondral cyst or geode if joint pathology is present |
|
|
What do chondromyxoid fibromas look like?
|
-They look like NOF’s, but they can occur in any age
-They do not contain calcified cartilage matrix |
|
|
How are chondromyxoid fibromas NOT like NOF’s?
|
-They often extend into the epiphyses, while NOF’s rarely do
-They often present with pain, which doesn’t happen with an NOF |
|
|
Okay, name all the benign cystic bony lesions seen in patients younger than 30 years old:
|
-Eosinophilic granuloma
-Aneurysmal bone cyst -Nonossifying fibroma -Chondroblastoma -Solitary bone cyst |
|
|
Name the “automatics,” benign cystic bony lesions that get added to all differentials for patients younger than age 30:
|
-Infection
-Eosinophilic granuloma |
|
|
Name the “automatics,” benign cystic bony lesions that get added to all differentials for patients older than age 40:
|
-Infection
-Metastatic disease and myeloma |
|
|
Name benign cystic bony lesions that have no pain or periostitis:
|
-Fibrous dysplasia
-Enchondroma -Nonossifying fibroma -Solitary bone cyst |
|
|
Name the benign cystic bony lesions in the epiphyses:
|
-Infection
-Giant cell tumor -Chondroblastoma -Geode -And if the patient is over 40 years old, add metastatic disease and myeloma, then remove chondroblastoma |
|
|
What is the difference between an epiphysis and an apophysis?
|
-The epiphysis contributes to bone length
-Apophyses serve as ligamentous attachments |
|
|
What is the differential for benign cystic bony lesions in the ribs?
|
“FAME”
-Fibrous dysplasia -Aneurysmal bone cyst -Metastatic disease and Myeloma -Enchondroma and Eosinophilic granuloma |
|
|
Which lesions must demonstrate calcified matrix?
|
Enchondroma (except in the phalanges)
|
|
|
What findings do not narrow the differential?
|
Presence or absence of:
-A soft tissue mass -Expansion of bone (except that it has to be present for an ABC) -Sclerotic or nonsclerotic border (except that it must be nonsclerotic in giant cell tumor) -Bony struts -Compartments within the lesion -Size of the lesion |
|
|
What is the differential for multiple benign cystic bony lesions?
|
“FEEMHI”
-Fibrous dysplasia -Eosinophilic granuloma -Enchondroma -Metastatic disease and myeloma -Hyperparathyroidism (brown tumors) -Infection |
|
|
Which lesions should be considered for a sclerotic focus in a 20-40 year old, especially if it’s an asymptomatic, incidental finding?
|
-NOF
-EG -Aneurysmal bone cyst -Solitary bone cyst -Chondroblastoma -Fibrous dysplasia -Osteoid osteoma -Infection -Brown tumor (Healing) -Giant bone island |
|
|
1
|
|

|
2
|
|
|
3
|
|

|
4
|
|

|
5
|
|

|
6
|
|

|
7
|
|
|
8
|
|
|
9
|
|

|
10
|
|

|
11
|
|
|
12
|
|
|
13
|
|

|
14
|
|
|
15
|
|
|
16
|
|
|
17
|
|
|
18
|
|
|
19
|
|
|
20
|
|

|
21
|
|
|
22
|
|
|
23
|
|
|
24
|
|

|
25
|
|

|
26
|
|

|
27
|
|

|
28
|
|

|
29
|
|

|
30
|
|

|
31
|
|
|
32
|
|

|
33
|
|

|
34
|
|

|
35
|
|
|
36
|
|

|
37
|
|
|
38
|
|
|
39
|
|
|
40
|
|
|
41
|
|

|
42
|