Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
124 Cards in this Set
- Front
- Back
|
Movement is influnced by
|
muiltple systems: environmental influences, sensorimotor factors, musculokeletal factors, regularoty functions and behavioral/emotional goals
|
|
|
Carr and Shepard's Motor Relearning Program (MRP)
|
person is an active participant
postural adjustements and limb movements are linked sucessful task relearning occurs when activites are performed automatically and efficiently learning of skills doesn't follow developmental sequence practice of compensatory strategies limits fxnal recovery intervention not focused on learning specific movemtns, instead on learning general strategies for solving motor problems obstacles to efficient movement include loss of soft tissue extensibility, balance loss, fixation patterns due to postural insecuity and muscle weakness abnormal movemtn patterns are attributed to repeated practice of compensatory movement strategies that become overleanred |
|
|
Contemporary Task-Oriented Approach
|
occupational performance emerges from interaction of multiple systems (including personal and performance contexts)
personal and environmental systems are heterarchiacally organized individua's behavioral changes reflect his/her attemptst to compenstate and acheive fxnal goals must practice with varied strategies to find optimal solutions for motor problems and develop skill performance fxnal tasks help organize motor behavior OT must detemine control parameters or systems that have positive or negative influences on motor behavior proactice opportunities are provided and appropriate to person's stage of learning OT conducts eval using top-down approach eval focuses initially on role performance & tasks second step of eval is task analaysis to identify which subsystems of person and/or environmatal factors limiting fxn |
|
|
COntemporary Task-Oriented Approach intervention
|
help pts adjust ot role and task performance limits
create environment that utilizes common challenges of daily life practicing fxnal tasks or close simulations to find effective and efficient strategies for performance provide opportunities for practice outside of therapy time remediate client factor min inefficient of ineffective movement pattern adapting the environment using assistive techonology |
|
|
Contemporary Motor Learning approach
|
treat motor dysfunction by incorporating principles of motor learning during interventsion focused on remediatign motor conrol in persons with CNS dysfunction
Goal: acquisition of fxnal skills that can be generalized to multiople situations and environments |
|
|
Stages of motor learning
|
1. skill acquisition stage (cognitive stage) occurs during intital instruction and practice of a skill
2. skill retention stage (associated stage) involves carry-over as individuals are asked to demonstrate newly acquired skill after intital practice 3. skill transfers stage (autonomous stage) invovles indivdiual demonstrating the skill in a new context |
|
|
Random (or variable) Practice
|
involves practice of several tasks that are presented in a randome order encouraging reformation of the solution to the presented motor problem
|
|
|
blocked practice
|
repeated performance of the same motor skill
|
|
|
intrinsic feedback
|
info received by learner as a result of performing task
info is received from tactile, vestibular & visual systems during and after task |
|
|
Extrinsic feedback
|
provided from outside source
includes knowledge of performance, which is verbal feedback abou the process or perfromance itself includes knwledge of resutls, which is OT's provision of feedback about hte outcome or end product that results of motor action |
|
|
Factors to promote generalization of motor learning
|
capacity to generate intrinsic feedback
high feedback regarding knowledge of performance low extrinsic feedbsck regarding knoweldge of results practice conditons tha tare variable, random whoel task performance as opposed to breaking activites into contrived parts high contextual interfeence utilizes environmental conditions that increase the difficulty of learning such as noise distractions, crowded environments, and random practice pracice in naurralistic settings |
|
|
Motor learning tx sequence
|
1. initial task is first activity performed by pt
2. near transfer is an alternate form of the initial task 3. intermediate trasnfer ahs a mod number of changes in task parameters but still has some siiliarities to the initial task 4 far transfer introduces activity that is coneptually the same as but physcially different from the intitial task 5. very far transfer requires spontaneous use of new strategy in daily fxnal activities |
|
|
Motor learning Cognitive stage characteristics
|
learned devleops as understanding of task, cognitive mapping, assess abilities, task demands, identifies stimuli, contacts memory, selects resonse, perfoms intital approximations of task; sructures motor progem, modifies intitial responses
What to do decison |
|
|
Motor learning congnitive stage tranining strategies
|
highlight purpose of task in fxnally relevant terms
demonstrate ideal performance of tsk to establish a reference of correctness have pts verbalize task components and requirements direct attn to critical task elements select appropriate feeedback ask learner to eval performance, outcomes, identify problems, solutions use reinforcemtns (praise) for correct performance, continuing motivation organize feedback schedule organize initial praoctice assess, modify arousal levels as appropriate structure environment |
|
|
knowledge of performance feedback
|
focus on erros as they become consistent; don't cue on lg number of random erros
|
|
|
knowledge of results feedback
|
focus on successes of movment outcome
|
|
|
motor leaning associated stage characteristics
|
learned practices movements, refines motor programs (spatial and temporal organization) decreases erros, extraneous movemnts, dependence on visual feedback decreases, increases for use of proprioceptive feedback; congitive mointoring decreses
ho to do decision |
|
|
motor learning associated stage training strategies
|
select appropriate feedback
oraganize feed back schedule organize practice structure environmetn |
|
|
motor learning autonomous stage characteristics
|
learner practices movement, continues to refine motor responses, spatial and temopral highly organized, movements are largely error free, minimal level of cognitive monktoring
how to succeed decision |
|
|
motor learning autonomous stage training strategies
|
assesses need for conscious attn automoatcity of movements
select appropriate feedback organize practice structure environment focus on competetive aspects of skills as appropriate (i.e. wheelchair sports) |
|
|
closed tasks
|
activities in which the environment is stable and predictable and methods of performance are consistent over time
|
|
|
variable motinless tasks
|
invovle interacting with a stable and predictable environmetn, but specific features of environment are likely to vary between performance trials
|
|
|
consistent motion tasks
|
reqire an individual to deal with environmental conditions that are in motion during activity performance; the motion is consitent and predictable between trials
|
|
|
open tasks
|
require peopel to make adaptive decison about unpredictable events because objects within the environment are in random motion during tak performance
|
|
|
Neurophysiologic (traditional) FOR
|
neurodevelopmental tx approach (NDT), proprioceptive neuromuscular facilitation (PNF), Brunnstrom's apporach, Margaret Rood's approach
|
|
|
Neurophysiologic FOR assumptions
|
controlled movemetn ois preceded by stereotyp0ic reflex responses
sensory input regulates motor output and sensation is necessary for movement to take place normal movements are governed by heirarchial centralized motor programs that determine muscle activiation patterns damange to higher control centers release lower level or primitive reflexes and movement patters from inhibition when basic movements and postures are normalized skilled movement woudl occur atutomatically integration of lower level spinal and brainstem reflexes occurs by eliciting higher level righting and equilibrium respones controlled sensory input applied by OT can influence motor responses use of faciliation and inhibition techniques can improve motor performance |
|
|
tx strategies used by Rood approach
|
1. sensory stimulation used to evoke a motor response (uses direct applicaiton of sensory stimuli to muscles and joints)
2. refelexive movment used as a precursor for volitional movement (reflexive movement acheived initially through the application of sensory stimuli) 3. tx directed toward influenciing muscle tone (sensory stimuli used to inhibit or facilitate tone) 4. developmetnal patterns/sequences used for the developmetn of motor skills (ontogenic motor patterns used to develop motor skills) |
|
|
tx strategies used by Brunnstrom approach (movement therapy)
|
1. sensory stimulation used to evoke a motor response (movement occurs in response to sensory stimuli)
2. refelxive movement used as a precursor for volitional movment (move pt along a continuum of reflexive to volitional movement patterns) 3. tx directed twoard invluencing muscle tone (postures, sensory stimuli used to inhibit or facilitate tone) 4. developmental patterns/sequences used for the developmetn of motor skills (flexion and extension synergies; proximal to distal return) 5. conscous attn is directed toward movement |
|
|
tx strategies for proprioceptive neuromuscular approach
|
1. sensory stimulation used to evoke a motor response (tactille, auditory, visual sensory stimuli promote motor responses)
2. reflexive movement used as a precursor for volitional movement (volitional movements can be assisted by reflexive supported postures) 3. tx directed toward influencing muscle tone (movement patterns used to normalize tone) 4. developmental patterns/sequences used for the development of motor skills (patterns used to facilitate proximal to distal motor control) 5. conscious attention is directed toward movement |
|
|
tx strategies of neurodevelopmental tx
|
1. sensory stimulation used to evoke a motor response (abnormal muscle tone occurs, in part, because of abnormal sensory experiences)
2. tx directed toward influencing muscle tone (handling techniques and postures can inhibit or facilitate muscle tone) 3. developmental patterns/sequences used for the developmetn of motor skills 4. conscious attention is driected tward movement 5. tx directly emphasizes development of skilled movements for task performance |
|
|
Neurodevelopmental treatment (NDT)/Bobath Technique
|
normalization of postural and limb tone is prerequisite to normal movement
avoidance of movements that increase tone inhibition of primitive refelxes and abnormal postural and limb movments development of normal patterns of posture and movement improvement of the quality of movement and peformance of the invovled side associated reactions postural reaqctions considered basis for control of movement loss of postural control results in overuse of sound side and limits fxnal movements stereotypical patterns of trunk & limbs observed in persons with CNS dysfunction are viewed as abnormal patterns of motor corrdination focus on improving quality of movement |
|
|
NDT/Bobath eval prcedures
|
observe malalignmetns in trunk & limbs in various positions
eval abnormal tonal patterns in trunk & limbs during PROM eval person's placing response or ability to hold a posture/position as OT releases support of limb/trunk assesses for presence of associated reactions and situations tha evoke them eval psotural control, person's ability to automatcially activiate msucles to maintain control of body for posture and movement (righting rxns, equilibirium rxns, protective responses, wtshifting activites) eval abnromal coordination patters of limbs eval both automatic postural rxns and volitional movements of the trunk & limb |
|
|
NDT/Bobath intervention
|
handling to utilize movement
wtbearing trunk rotation scapula mobilization pelvic alignment and wtshifts slow & controlled movements proper positioning retrain integration of bilateral activities during ADLs bilateral movement patterns |
|
|
Proprioceptive Neuromuscular Facilitation
|
response of neuromsucular mechanixms can be hastened through stimulation of the proprioceptors
techniques are superimposed on patterns of movement and posture, focusing on sensory stimulation form manual contacts, visual cues, and verbal commands normal motor devvelopmetn proceeds in a cervicocaudal and porximodistal direction early motor behavior dominated by reflex activity early motor bheavior is characterized by spontaneous movement, which oscillates between extremes of flexion and extension developing motor behavior expressed in aorderly sequence ot total patterns of movement and posture shifts between flexor and extensor dominance in development normal motor development has an orderly sequence of total patterns of movemtn and posutres locomotion depends on reciprocal contraction of flexors and extensors maintenace of posture requires continual adjustment for nuances of imbalance frequency of stimulation and repetitive activity aqre used to promote and retain motor learning, and to develop strenght and endurance goal driected activites couple with techniques of facilitatio are used to hasten learning of total patterns of walking and sel-care activites goal directed activity is made up of reversing movements normal movement and posture depend upon synergism and balanced interacton of antagonists |
|
|
PNF eval
|
eval reflects developmental sequence proceeding in a proximal to dital direction
vital fxns of respiration, swallowing, voic production, and oral/facial movements are evaled for weakness and asymmetry movements in response to visual, auditory, and tactle stimulation are eleicited to determine which sensory cues reinforce movement head and neck patters are observed during devleopmetnal activiteis diagnoal patters of extremeites evaluated (bilateral symmetrical, bilateral asymmetrical, bilateral reciprocal, unilateral) developmental postures are observed adn noted if the person can assume and maintain them fxnal tasks are observed and evaled throughout the eval process observations of the following are made (dominance of flexor or extensor tone, midline alignment, stability and mobitlity in various patters, influence of head, ncek, and trunk patterns, ROM, quality of movement, timing of movements) |
|
|
PNF intervention
|
diagonal patterns or mass movement patters are utilized during fxnal activities
assisted diagnoal patterns using techniques of chop and lift total patterns of movement during tx utilize a developmental approach PNF tecniques are superimposed on psotures and movement patterns (HOH, quick stretching, traction, approximation or manual compression, max resistance) repeattive contractions of agonists to weaken components, thytmic initiation to improve movemnet initiation promote reversals of antagonists (alternate isotonic contracton of antagonist, rhytmic stabiliation during isometric contraction of antagonists) relaxation techiniques: contract-relax (isometric contractionof antgonist, relax then PROM of antagominst in agonist pattern), hold-relax (isometric contraction of antagonist, relaxation, then AROM of agonist), rhythmic roation (restriction felt during ROM so motion repeated slowly and gently to promote expansion of range) |
|
|
pattern analysis of diagnoal DI flexion (UE)
|
scapula: abd and upwardly rotated
shoulder: flexed, add, ER elbow: slightly flexed forearm: supinated wrist: felxed towards radial side fingers: flexed, add thumb: flexed, add |
|
|
pattern analysis of diagonal DI extension (UE)
|
scapula: add, downwardly roated
shoulder: extended, abd, IR elbow: extended forearm: pronated wrist: extended toward ulabnr side fingers: extended, abd thumb: extended, abd |
|
|
pattern analysis of diagnoal D2 flexion (UE)
|
scapula: add, and upwardly rotated
sholder: flexed, abd, ER elbow: extended forearm: supinated wrist: extended toward radial side fingers: extended, abd thumb: extended, abd |
|
|
pattern analysis of diagnoal D2 Extension (UE)
|
scapula: abd, downwardly rotated
shoulder: extended, add, IR elbow: towards flexion forearm: prontated wrist: flexed toward ulnar side fingers: flexed, add thumb: flexed, abd, opposed |
|
|
Commands during D2, D2 to be said during performance
|
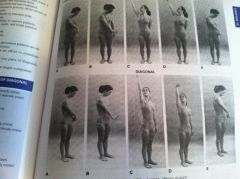
A: ready! look at your hand!
B open and turn your right hand, thumb toward your face C: lift up and out D: now close your hand E: and pull down and accross and repeat and again |
|
|
commands during D1 flexion and extension as perform
|
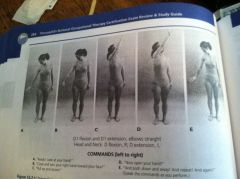
A: ready look at your hand
B: close and turn your right hand toward yoru face C pull up and across D now open your hand E and push down and away and repat and again |
|
|
Brunnstrom's Movement Thearpy
|
outdated, no longer used:
focused on facilitating recoery through specific sequence tx: focused on promotion of movement from reflexive to voltional (7 stages of motor recovery following hemiplegia eval: classify as 1 of 7 stages intervention: progress thorugh recoery stages |
|
|
stage 1 Brunnstrom
|
flaccidiyt, no voluntary or reflexive activity
|
|
|
stage 2 Brunnstrom's
|
minimal voluntary movement, components of synergies arer elicited as relfex reactions. Spasticity begins to develop
|
|
|
Stage 3 Brunnstrom's
|
marked spasticity, synergies are performed voluntarily
|
|
|
Stage 4 Brunnstrom's
|
movements that begin to deviate from synergy can be accomlished on a volitional basis
|
|
|
Stage5 Brunnstom's
|
Movements which differe greatly form the bawsic synergies are utiliszed
|
|
|
Stage 6 Brunnstrom's
|
spasticity is essentially absent; isolated muscle actions are freely perfomred
|
|
|
Stage 7 Brunstrom's
|
normal motor fxn
|
|
|
shoulder girdle synergy movements
|
flexion: elevation/retrqaction
extension: depression/protraction |
|
|
Shoulder synergy basic movements
|
flexion: abd/ER
extension: add/ IR |
|
|
Elbow synergy movements
|
flexion: flexion
extension: extension |
|
|
Forearm basic movement synergies
|
flexion: supination
extension: pronation |
|
|
Hand synergy movements
|
flexed: variable (usually flexion)
extension: variable (usually flexion) |
|
|
Hip synergy movement
|
flexion: flexion, abd, ER
extension: extesnions/add/ IR |
|
|
Knee synergy movement
|
flexion: flexion
extension: extension |
|
|
Ankle synergy movment
|
flexion: dorsiflexion
extension: plantar flexion |
|
|
Foot synergy movement
|
flexion: inversion
extension: inversion |
|
|
Margaret Rood's Approach
|
no longer used in practice.
Assumes: sensorimotor control is developmentall based, has four sequential phases of motor control muscular responses of agonists, antagonist and synergist are believed to be relfexively programmed according to purspose or plan described motor development termed ontogenic motor patterns that includes 8 patters in sequence (supine withdrawal, rollover, prone extension, neck co-contraction, prone on elbows, quadruped, standing) |
|
|
Reciprocal inhibition/innervataion phase of motor control
|
early mobility pattern thats primarily a reflex governed by spianl and supraspinal centers.
|
|
|
Co-contraction phase of motor control
|
defined as a simultanesous contraction of the agonist and antagonist that provides stability in a static pattern
utilized to hold a position or object for a long duration. |
|
|
Heavy work phase of motor control
|
also termed mobility superimposed on stability
in these patterns, proximal muscles contract and move and the distal segments are fixed |
|
|
Skill phase of motor control
|
considered the highest level of control and combines stability and mobility
these patterns consist of stabilized proximal segment while the distal segments move in space |
|
|
Rood's approach eval procedure
|
evaluate distribution of muscle tone
determine level of motor control based on Rood's developmental sequence determinet he therapeutic activity of choice and how to progress the individual to the next level of control |
|
|
Rood's Intervention
|
Normalization of tone and muscular respones are acheived via controlled sensory stimulation
motro resonse that's acheived is dependent on type of sensory stimulation OT applies (facilitation or inhibition) individualts are placed in various developmental postures that evoke particular muscular responses individual is engaged in activities appropriate to developmental patterns in effort to master each level and progress to more difficult patterns/activities purposeful activities provided so person can utilize the evoked movement pattern in context of task repetition/practive is necessary for motor learning |
|
|
5 Point Ashworth Scale
|
objective measurements of spasticity
1=normal tone 5= severe hypertonus/rigidity |
|
|
Modified Ashworth Scale
|
Objective measurement of spasticity
0= no increse in muscle tone 4= the affected part is rigid in flexion or extension |
|
|
Quick Stretch
|
measure spasticity by applying stretch in opposite of muscle groups being tested. Graded as minimal, moderate or severe
min: catch at end range mod: catch in middle range severe: catch at beginning of range |
|
|
intention tremor
|
worsening of action tremor as limb approaches a target in space
|
|
|
dysmetria
|
undershooting (hypometria) or overshooting (hypermetria) of a target
|
|
|
dyssynergia
|
breakdown in movement resulting in joints being moved separately to reach a desired target as opposed to moving in a smooth trajectory; decomposition of movement
|
|
|
dysdiadochokinesia
|
impaired ability to perform rapid alternating movements
|
|
|
ataxia
|
loos of motor control including tremors, dysdiadochokinesia, dyssynergia and visual nystagmus
|
|
|
resting tremor
|
involuntary tremor noted in resting postures
|
|
|
cogwheel rigidity
|
alternative contraction/relaxation of muscles being stretched
|
|
|
lead pip rigidity
|
consistent contraction throughout range
|
|
|
bradykinesia
|
overall slowing of movement patterns
|
|
|
akinesia
|
inability to initiate movement
|
|
|
arthetosis
|
dyskinetic condition that includes inadequate timing, force and accuracy of movements in the trunk/limbs; movement are writhing and worm-like
|
|
|
dystonia
|
involuntary sustained distorted movement or psture involving contraction of groups of muscles
|
|
|
Chorea
|
involuntary movements of hte face and extremities which are spasmodic and of short duration
|
|
|
hemiballismus
|
unilateral chorea charcterized by violent, forceful movmeents of the proximal muscles
|
|
|
Glenohumeral joint subluxation assessments
|
allow person's arm to dangle into gravity
palpate the space underneath the acromion process with your index finger compare to the intact side and document hte width of the space in terms of finger breadths |
|
|
serial splints
|
utilized to acheive slow, progressive increase in motion by progressive remodling
|
|
|
Cock-up splints
|
supports wrist in 10-20 extension, allows digit function
|
|
|
resting hand splint
|
utilized for persons who need to have their wrist, digits, and thumb supported in a functional position for prolonged periods
|
|
|
oppponens splints
|
may be short or long
designed to support the thumb in a psositon of abd, opposition utilized during fxnal activities to compensate for weakness patterns |
|
|
Bobath finger spreader (abduction splint)
|
soft splint positions the digits and thumb in abd in effort to reduce tone
-inhibiting pattern |
|
|
Rood cone
|
cone-shaped splint utilized to reduce flexor spasticity in hand
-sustained deep pressure |
|
|
orthokinetic splints
|
utilizes tactile input to facilitate and/or inhibit appropriate muscle groups
|
|
|
spasticity reduction splint
|
places spastic distal extremity on submaximal stretch to reduce spsticity
|
|
|
Overhead suspension sling
|
orthotic device incorporates an arm support that's supported by a sling and suspended by an overhead rod
used with those whoe have proximal weakness (ALS, Guillian-Barre syndrome, MD) with muscle grades in the 1/5 to 3/5 range are appropriate candidates |
|
|
Balanced forearm orthoses (mobile arm supports or ball-bearing forearm orthoses)
|
arm trought, proximal and distal arms and a support braacket
allow a pt with weak proximal musculature to utilize avaliable control of the trunk and shoulder to engage in fxnal tasks |
|
|
shoulder slings
|
utilized to support a flaccid arm after neurologic insult for short and controlled periods of time
long term use may be detrimental in terms of soft-tissue contracture, eddema, and development of pain syndromes |
|
|
oral motor dysfunction charcteristics
|
impaired speech (dysarthria), swallowing impairments (dysphagia), or psychosocial stresses related to facial asymmetry and/or drooling
|
|
|
Eval of oral motor dysfunction
|
ROM, strength and tone of lips, cheeks and tongue
extra- and intra-oral sensation dentition oral control of bolus presence of swallow relfex aireway protection (gag reflex, volitonal and spontaneous coufgh, vocal fold adduction, and reflexive inhibtion of respiration) relaxation of esophageal sphincter primitive relfexes (rooting, jaw jerk, bite reflex, ATNR/STNR) cranial nerve testing objective testing (modified Barium Swallow/Videofluoroscopy, FEES) |
|
|
jaw jerk
|
center of mandible is firmly tapped 1-2 times
normal response is no reaction pathological response is relfexive jaw closure/oopening response |
|
|
Bite reflex
|
tongue depressor is placed lightly between the upper and lower teeth
reflexive bite indicates pathology |
|
|
oral motor dysfunction intervention
|
direct therapy techniques that utilize bolus: modification of consistency, amount and pacing of solids and liquids, chin tuck, head tilt, head turn, swallowing adaptations (supraglottic swallow techinque to voluntarily close/protect airway during food intake or Mendlesohn's maneuver: voluntarily prolonging the rise of the larynx by prolonging tongue contraction)
Indirect therapy don't include use of bolus: thermal (cold) stimulation, reflex facilitation, strengthening, facilitation and coordination of oral movements, aireway adducton procedures, positioning to maintain the trunk/head/neck in correct postures |
|
|
Cranial Nerve 1: Olfactory
|
fxn: sensory: carries impulse for sense of smell
testing procedure: person asked to sniff varous aromatic substances |
|
|
Cranial nerve 2: Optic
|
fxn: sensory: carries impulses for vision
testing procedure: eye chart testing, visual field testing |
|
|
Cranial Nerve 3: Oculomotor
|
fxn: motor: fibers to superior, inferior, and medial rectus muscles of the ege and to the smooth muscle controlling lens shape. Medial and vertical eye movments. Sensory: proprioception of the eye
testing procedure: pupil sizes are compared for shape and equality, pupillary reflex is tested, visual tracking is tested |
|
|
Cranial nerve 4: Trochlear
|
fxn: prioprioceptor and motor fivers for superior oblique muscle of hte eye. downward and inward eye movement
testing procedure: tested with cranial nerve 3 releative to following moveing objects |
|
|
cranial nerve 5: trigeminal
|
fxn: motor & sensory for face, conducts sensory impulses form mouth, nose, eyes; motor fibers for muscles of mastication. Control of jaw movements
testing procedure: pain, touch, temp are tested with proper stimulus; corneal reflex tested with a wisp of cotton; person is asked to move jaw through full ROM |
|
|
Cranial nerve 6: Abducens
|
fxn: motor and proprioceptor fibers to/from lateral rectus muslce. lateral eye movments
testing procedure: tested in conjuntion with cranial nerve 3 releative to moving eye laterally |
|
|
Cranial nerve 7: facial
|
fxn: mixed (sensory & motor): sensory fibers to taste buds and anterior 2/3 tongue, motor fibers to muscles of facial expression and to salivary glands
testing procedure: check symmetry of face, ask person to attempt varous facila expressions; sweet, salty, sour, and bitter substances are applied to tongue to test tasting stability |
|
|
Cranial nerve *: vestibulocholear (acoustic)
|
fxn: sensory: transmits impulses for senses of equilibirum and hearing
testing procedure: hearing is checked with a tuning fork |
|
|
cranial nerve 9: glossopharyngeal
|
fxn: motor fibers for pharynx and salivary glands; sensory fibers for pharynx and posterior tongue. Tst sensation for sweet, bitter and sour
testing procedure: gag and swallow reflexes are checked, posterior one third of tongue is tested for taste |
|
|
cranial nerve 10: Vagus
|
fxn: sensory/motor impulses for larynx and pharynx; parasympathetic motor fibers supply smooth muscles of abdominal organs; sensory impulses from viscera
testing procedure: tested in conjunction with cranial nerve 9 |
|
|
Cranial nerve 11: spinal accessory
|
fxn: sensory/motor fibers for sternocleidomastoid, trapezius muscles, muscles of soft palate, pharynx, and larynx. Movement of neck an dshoulders
Testing procedure: sternocleidomastoid and trapezius muscle testing |
|
|
Cranial nerve 12: hypoglossal
|
fxn: motor/sensory fibers to/from tongue, movement of tongue
testing procedure: ask person to stick out tongue, positional abnormalities are noted |
|
|
sensory integration FOR for sensory processing disorders assumptions
|
developed by A. Jean Ayres
views neural organization of sensory info for an adaptive response plasticity fo CNS allows for modifications sensory integration occurs in developmental sequential manner higher cortical processing fxns are dependent on adequate processing andn organization of sensory stimuli by lower brain centers adequate modulation of sensory stimuli must occur for an adaptive response to occur (facilitory or inhibitory) adaptive responses faciliate the integration of sensory stimuli individuals seek out sensorimotor experiences that have an organizing effect |
|
|
Sensory Integration and Praxis Tests (SIPT)
|
std sensory integration tests for children 4-8 yrs. 17 test primarily address relationship of tactile processing, vestibular proprioceptive processing, visual perception and practic ability.
4 overlapping group categories administration requires certification |
|
|
DeGangi-Berk Test of sensory Integration (TSI)
|
std for 3-5 yrs
measures sensory integrative fxn with focus on vestibular system categorized into 3 areas: bilateral motor coordination, postural control, and reflex integration |
|
|
Test of Sensory Functions in Infants
|
std test for 1-18 months
assesses level of infant's sensory responsiveness to a variety of sensory stimuli |
|
|
Sensory Processing Measure (SPM)
|
test for elementary school age children
measures sensory processing, praxis, & social participation across different environments assess visual, auditory, tactile, olfactory-gustatory, proprioceptive, and vestibular behaviors home form is completed by primary caregiver, main classroom form is completed by primary classroom teacher, and school environments form is completed by otehr school personnel involved with the child in other settings |
|
|
Sensory Integration Intervention
|
follows principles of SI theory: control sensory input to improve sensory processing, faciliate sensory integration, and elicit and adaptive response. create environment to faciliate active participation; ensure registation of meaningful sensory input to obtain and adaptive response; balance stgructure and freedom, tapping into the child's inner drive to obtain neural organization;/ graually introduce activities requireing mroe mature and complex patterns of behaviors; promote organized adaptive responses to enhance a child's general beahvioral organization, including socialization
|
|
|
Grading of type and rate of movement
|
firm pressure and resistance is less threatening than light touch
linear movment is less threatening than angular slow movement is less threatening than rapid movement |
|
|
Sensory processing deficits intervention for tactile
|
tactile modulation for tactile defensiveness, hypersensitivity/over-responsivity; and hyposensitivity/under-responsitivy and sensory seeking:
-self applied stimuli are more tolerable than passive application of tactile stimuli -provide deep touch/firm pressure where teh child can see the source of the stimuli, which tends to be more tolerable vs light touch stimuli tha ttends to be aversive, especially to the face, abdomen, and palmar surfaces of teh extremities -provide controlled sensory activities that simultaneoulsy provide tactile and vestibular-proprioceptive info -begin with slow linear movements and deep touch-pressure -apply tactile stimuli in the direction of hair growth which is less aversive -follow tactile stimuli with joint compression -monitor and adjust stimuli that seem to influence modulation of stimuli -be alert and assess child's behavioral responses up to a few hours following tx when negative impacts may still demonstrated -tactile defensiveness and sensory-seeking can be reduced if tx approach is effective |
|
|
sensory processing intervention for tactile discrimination
|
provide deep touch pressure to hte hands as well as the body
deficits rarely seen in isolation and somatodyspraxia is typically seen;p therefore, tx for tactiel discrimination is usually performed simultaneously when providing tx for deficits in motor planning provide graded activities requiring tactile discrimination activities using a mix of textures and items |
|
|
Sensory integration intervention for proprioception
|
deficits in modulation demonstrated by over-responsitivity/under-responsitivity and sensory seeking:
-provide firm touch, pressure, joint compression or traction -provide resistance to active movement to help the child learn the appropriate amt of force to perform tasks -provide activiteis in various body positions combining vestibular proprioceptive info -provide slow linear movement, restistance, and deep pressure -use adaptive techniques discrimination deficits: provide tx as noted above, provide activities requireing the child to demonstrate teh ability to grade the force or efforts of movement |
|
|
Sensory integration intervention for vestibular
|
deficits in modulation fo vestibular input include over-respnosivity/under-responsitivity, hyhpersenstivity (aversion response), sensory seeking, and gravitational insecurity (fear response)
-grade for type of rate of movement and for amt of resistance (precautions must be observed) -slowly introduce linear movemtn with touch pressure in prone and provide resistance to active movements, esp for gravitational insecurity -use linear vestibular stimuli to increase awarenss of spatial orientaiton (otolith organ) -provide rapid rotary and angular movemetns with frequent starts/stops and acceleration/deceleration to increse ability to distinguqish the pace of movement (semicircular canals) |
|
|
other sensory integration interventions
|
special and advanced training and knowledge of the effects of various sensory stimuli is required
provide compensatory skill development reduce environmetnal barriers and identify facilitators of occupational performance use group tx to develop the social interaction skills needed for imporved occupational perforamnce in a classroom, with peer groups, and/or in afterschool programs consult with and/or educate teachers and parents share intervention strategies for specific sensory processing deficits |