![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
List the 3 spinal tracts and symptoms the are responsible for and at which side? Spinal cord extend to ? |
(1) corticospinal tract (posterolateral cord) – voluntary motor power , ipsilat
(2) spinothalamic tract (anterolateral cord) –pain and temperature from contralat (3) posterior column – proprioception,vibration, & some light touch, from ipsilat Spinal cord extends to L2 |
|
List the spine inures stable (5) vs unstable (13) and the MOI? |
“Jefferson Can Bit Off A Hangman’s Thumb” : all flex except the noted
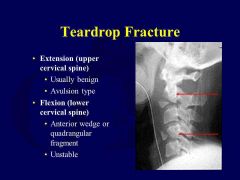
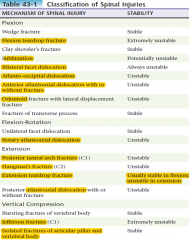
Jefferson (C) Chance # Bilateral facet dislocation Odontoid (types II, III) Atlantoaxial (ant/post/rotary) or atlanto-occipital dislocations Hangman’s fracture (E) Teardrop fracture (F for ****** , E for excellent)
Stable: V body: C Wedge :E SP: direct/ avulsion against flex TP: F Uni facet dislocation: Rot Tear Drop Extension: E |
|

What type of #? When does it become unstable? |
Compresion Wedgefracture |
|

Identify? What is MOI/# involved? |
Clayshoveler’s Flexion against supraspinous ligament → avulsion of SP Stable |
|
|
Subluxation, define/ radiology?
|
No bony injury
Radiographs may be normal, but may show widening of interspinous or intervertebral spacesposteriorly or at facets |
|
|
How to Dx Atlanto-occipital dislocation? |
|
|
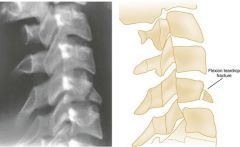
Describe and Dx? |

Flexion teardrop |
|

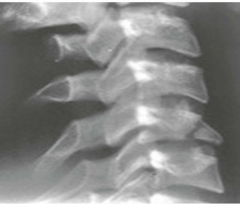
Identify? Which vertebra is #? What are you going to see on AP x ray? What do you call this finding on Lateral x ray? |
Unilateralfacet dislocation. APXray shows SP off midline, Lateral Xray “Bowtie” |
|
|
Bilateral facet dislocation
How does it look like? describe it? |
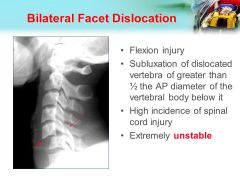
Ant displacement > 50%of vertebral body
|
|
|
Rotary atlantoaxial dislocation
Stability? Best view to assess? |
Unstable. Seen best with open mouthview |
|
|
Extensionteardrop
Appearance? Ass w? |
Assd with central cordsynd |
|

Identify and describe? Stability? |
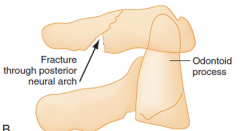
Posteriorneural arch # (C1)
Posterior arch compressed between cranium and C2 SP Unstable. |
|
|
Hangman’s #
Describe? Stable? MOE? |

(C2)Bilateralpedicle #’s +/- dislocation
Unstable Extention |
|
|
Vertebralburst
MOI How to differentiate from wedge compression & flexion teardrop |
MOI: Vertical compression Differentiating: Frontalplane (AP) shows vertical # unlike wedge compression & flexionteardrop |
|
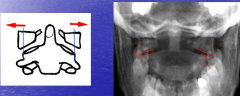
Dx? Describe? MOI? How to make Dx? |
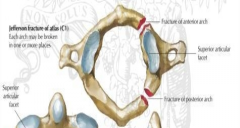
Jefferson# (C1)
MOI:Vertical compression Fracturesof: 1. ant and post arches 2. disruption of TV ligament Dx: Sum of displacement of left and right sides>7mm = # |
|
|
What nerves are responsible for the following: Diaphragm Horner’s syndrome Priapism |
Diaphragm innervated by C3-5
Horner’s syndrome (ptosis, miosis, anhidrosis) possible with injury to sympathetic trunk C7-T2 Priapism with severe SCI |
|
|
What type of motor neuron lesion with:
Paralysis with intact reflexes Paralysis w/o DTRs |
Paralysis with intact reflexes → UMN (spinal cord lesion);
Paralysis w/o DTRs → LMN (nerve root, cauda equina) |
|
|
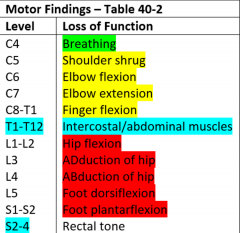
MotorFindings in spinal inj
|
|
|
|
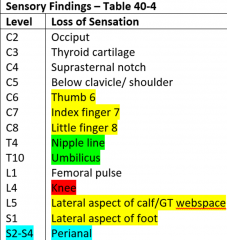
SensoryFindings in spinal inj
|
|
|
|
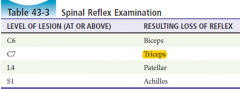
Reflex? |
|
|
|
What is the Frankel classification of SCI:
|
A (complete – no sensory, no motor), B, C, D, E (normal) A = Complete B = Sensation, no motor C = Preserved motor but major muscle groups have strength :heart: D = Preserved motor with most major at least 3 E = Normal |
|
|
What improves prognosis in Complete cord lesions
|
Search for sacral sparring(perianal sensation, normal rectal tone, flexor toe movement NOT anal wink orbulbocavernosus reflex)
|
|
|
Central cord syndrome
S/S? Prognosis? Brown-Sequard syndrome S/S? MOI? Anterior cord syndrome: S/S? MOI? |
Central cord syndrome MOI: Buckling of ligamentumflavum into cord with extension Prognosis >50% ambulatory and regain bowel and bladderfunction Brown-Sequard syndrome S/S:- ipsilateral motor and vib/sensation loss, -contralateral loss of pain/temperature MOI: penetrating trauma Anterior cord syndrome S/S: legs>arms motor/pain/temp with preservation of (touch, vibration) MOI: flexion injuries orvascular mechanism |
|
|
Posteroinferior cerebellar artery syndrome
S/S MOI |
Posteroinferior cerebellar artery syndrome
S/S: dysphagia, dysphonia, hiccups, N/V, dizziness/vertigo, and cerebellar ataxia MOI: severe hyperextension and resulting compression of vertebral arteries |
|
|
Conus medullaris vs caudaequina?
|
Cauda equina : diminished sensation, reflexes, including Babinski, and power (LMN lesion)
Conus medullaris : bilateral,can have intact bulbocavernosus reflex, normal/↑ rectal tone, may have ↑reflexes (UMN lesion), possibly ↑muscle tone (spasticity) |
|
|
CanadianC-Spine Rule
Inclusion/exclusion? Define dangerous mechanism? Simple rear-end MVCexcludes? |
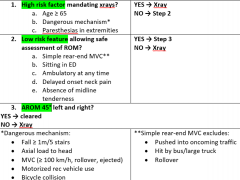
Included:alert (GCS 15) and stable trauma patients with neck pain or no neck pain butinjury above the clavicles, not ambulatory, AND dangerous mechanism
Excluded: -<16yo, -minor injuries (laceration), -GCS<15, -injury >48h, -grossly abnormal VS - penetrating trauma (open), -paralysis -vertebral disease (RA, AK, previous sx, stenosis) -Pregnancy |
|
|
NEXUS?
|
– “NSAID” –
1. Neurologic deficit 2. Spine tenderness (midline) 3. ALOC 4. Intoxication 5. Distracting injury |
|
|
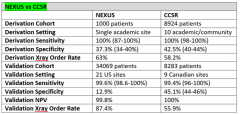
NEXUS vs CCSR Derivation Setting Derivation Sensitivity Derivation Specificity Derivation Xray Order Rate Validation Cohort Validation Setting Validation Sensitivity Validation Specificity Validation NPV Validation Xray Order Rate |
|
|
|
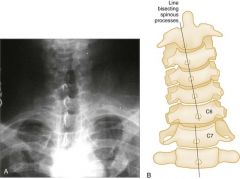
In lateral C spine x ray: How to know its adequate? Lines? |
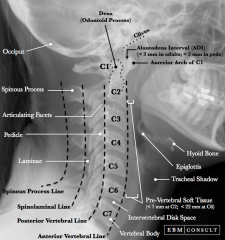
Adequacy (T1)
Lines: 1. Anterior vertebral 2. Posterior vertebral 3. Spinolaminal line, 4. SP line Soft tissues, retropharyngeal space: Generalrule – above C4 < ½ vertebral body; below C4 1 vertebral body 7 @C2 , 2 @C7 |
|
|
How to do Atlanto-occipital assessment?
|
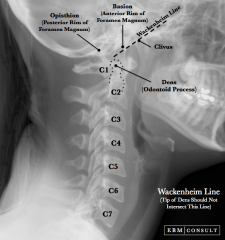
Power’s ratio and Wackenheim’s line (linedrawn from clivus passes tangentially to the posterior tip of odontoid)
|
|
|
What is posterior cervical line in peds (swischeck)?
Pseudosubluxation? normal Predental space in peds and adults? |

Connectsthe points bisecting the bases of the spinous processes of C1 and C3
Pseudosubluxationallowed in children at C2/C3 ≤ 2 mm Predentalspace: 3mm in adults, 5 mm in children
|
|
|
Indications for C-spine CT
|
|
|
|
MRI spine in trauma good for the Dx of? |
Gold standard for acute
1. Disk herniation, 2. Ligamentous injury, 3. Epidural and subdural hemorrhage, 4. Vertebral artery occlusion |
|
|
Differential Diagnosis for Bradycardia + Hypotension in Trauma
|
1. Spinal shock (diagnosis of exclusion)
2. Cushing’s Response 3. Cardiac contusion 4. Retroperitoneal hemorrhage (b/c ↑ vagal tone) 5. Hemorrhage in person who is β-Blocked |