![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
347 Cards in this Set
- Front
- Back
|
Suppositories |
- Solid dosage forms intended for insertion into body orifices where they melt or dissolve - Exert local or systemic effects - Commonly used rectally, vaginally, & occasionally urethrally - Have various shapes and sizes Water soluble supp.: dissolve (ex. PEG) Oil supp.: melt (ex. cocoa butter) |
|
|
Types of Suppositories: Rectal |
- Most frequently used to relieve pain, irritation, itching, and inflammation - Popular laxative, glycerin suppositories, promote laxation by local irritation of mucous membranes Astringent (zinc oxide – 10% of weight of supp.) and protectant (base – cocoa butter-35% of weight of supp.) Glycerin supp. For adult use thedose of glycerin is usually 2g/supp., 1.2g/supp. for ped dose |
|
|
Types of Suppositories: Vaginal |
- Mainly used as contraceptives, antiseptics in feminine hygiene, and specific agents to combat as invading pathogen Ex. - Nonoxynol-9 for contraception - Trichomonacides to combat vaginitis caused by Trichonomas vaginalis, Candida albicans, & other microorganisms - Estrogenic substances as dienestrol are used to restore vaginal mucosa state Nonoxynol-9:100mg AI/supp. (base is PEG – water soluble base) Vaginal inserts: other vaginal dosage forms(which usually combine suppository & tablet and are inserted vaginally –usually to treat vaginitis) |
|
|
T/F: Nonoxynol-9 suppositories are used for constipation |
FALSE Used for contraception |
|
|
Advantages of Suppositories |
- Viable administration route in patients with nausea or vomiting, pts who are unconscious, severely debilitated, or infants/small children - Does NOT have taste limitations - Avoid gastric acid and hepatic first-pass metabolism |
|
|
Disadvantages of Suppositories |
- Rectal absorption potentially interrupted by defecation - Relatively smaller area for absorption (as compared to entire GI tract) - Less fluid volume may cause problems with drug dissolution or absorption - Oleaginous base: Absorption of most drugs is erratic and unpredictable - Patients do not prefer this route due to administration difficulties All suppositories: have relatively smaller are of absorption when we compare toorally-taken medicine (tablet). Orally degrades more than rectal (because of gastric enzymes and GI tract) |
|
|
T/F: Rectal suppositories have relatively larger area for absorption as compared to orally taken dosage forms. |
FALSE Has smaller area for absorption |
|
|
Effects of Location |
Local action Systemic action |
|
|
Effects of Location: Systemic action |
- Systemic effects: mucous membranes of rectum and vagina permit the absorption of many soluble drugs - Although rectum is used frequently as site for systemic absorption of drugs, the vagina is NOT as frequently used for this purpose Rectum: systemic site of absorption Vagina: NOT for systemic absorption |
|
|
T/F: The rectal but not the vaginal suppositories are usually used to achieve systemic effects of drugs. |
TRUE |
|
|
Examples of drugs administered rectally in the form of suppositories for their systemic effects |
- Prochlorperazine & chlorpromazine - Oxymorphone HCl - Ergotamine tartrate - Indomethacin - Ondansetron |
|
|
Advantages for Achieving Systemic Effects with Suppositories |
- Drugs destroyed or inactivated by pH or enzymatic activity of stomach or intestines need NOT be exposed to these destructive environments - Drugs that irritate the stomach may be given without causing such irritation - Drugs destroyed by portal circulation may bypass the liver after rectal absorption (first pass) - Route is convenient for administration of drugs to adult or pediatric patients who may be unable or unwilling to swallow medication - Effective route in treating patients with vomiting episodes |
|
|
Rectal Suppositories Absorption Factors |
- Physiologic - Physiochemical factors of drug - Suppository base |
|
|
Physiologic Factors: Colonic content |
- When deemed desirable, an evacuant may be administered and allowed to act before the administration of a suppository of a drug to be absorbed. - Diarrhea and tissue dehydration affects the effect |
|
|
Physiologic Factors: pH & lack of buffering |
- Because rectal fluids are essentially neutral in pH and have no effective buffer capacity, the form in which the drug is administered will NOT be chemically changed by the rectal environment - Suppository base employed has a marked influence on the release of active constituents incorporated into it Which buffer solution can resist pH change more? Lower buffer capacity, or higher buffer capacity? The one with higher, so it will resist more change |
|
|
T/F: Because rectal fluids have high buffer capacity, the drug there can be effectively ionized and obtain better solubility |
FALSE Rectal fluids have no effective buffer capacity |
|
|
Physiologic Factors: Circulation route |
- The lower hemorrhoidal veins surrounding the colon receive absorbed drug and initiate its circulation throughout the body, bypassing the liver - Lymphatic circulation also assists in absorption of rectally administered drugs |
|
|
Physiochemical Factors of the Drug: Lipid-Water Solubility |
- Lipophilic drug is distributed in fatty suppository base in low concentration has LESS tendency to escape to surrounding aqueous fluids, than a hydrophilic drug present in fatty base to an extent approaching its saturation - Water soluble bases (ex. PEG), dissolve in anorectal fluids, release for absorption is in both water-soluble and oil-soluble drugs - Naturally, the more drug contained in a base, the more drug will be available for potential absorption If hydrophilic substances are in fatty base, then this drug can be better released than lipophilic (lipophilic in fatty base want to stay together if surrounded by aqueous fluid) |
|
|
T/F: Water-soluble bases can only be used for water-soluble drugs |
FALSE Can be used for both water-soluble and oil-soluble drugs |
|
|
Physicochemical Factors of the Drug: Particle Size |
- For drugs present in a suppository in undissolved state, the size of drug particle will influence rate of dissolution and availability for absorption - Smaller the particle size, the more readily the dissolution of the particle and the greater the chance for rapid absorption Particles need to be dissolved and finally absorbed. When base dissolves, the AI particles dissolve at the same time (the size of the drug particles will influence the rate of dissolution and absorption) If you want to increase dissolution, then decrease the particle size |
|
|
Solubility and Particle Size Equation |
Log S/S0= 2yV/2.303RTr -S: solubility of particles -S0: solubility of solid -y: surface tension -V: molar volume -T: absolute temperature (K) -r: radius of particles -R: gas constant (8.134*107) |
|
|
Physicochemical Factors of the Drug: Nature of base |
- Possibility of chemical and/or physical interactions between the medicinal agent and the suppository base, which could affect stability and/or bioavailability of the drug - If the base is irritating to the mucous membranes of the rectum, it may initiate a colonic response and prompt a bowel movement, negating the prospect of complete drug release and absorption ------------------ First exam |
|
|
Suppository Bases: Desired Properties for a Suppository Base |
- Remaining solid at room temperature - Melting or dissolving readily at body temperature - Chemically and physically stable - Non-toxic, non-sensitizing, and non-irritating - Expansion and contraction characteristics - Absorb some water - Proper viscosity We want the suppositories to remain solid at room temperature because we apply it in patients at room temperature. It must melt or dissolve at body temperature, otherwise drug cannot be released. It must be stable, otherwise we cannot use suppositories dosage form for patients. Irritation from PEG base is higher than irritation for CB base. For rectal use, use oily base. For vaginal use, we need the least irritating. We need expansion and contraction characteristics (more related to compounding procedure than to body orifice), because after compounding and cooling down, the volume of the suppository decreases (important for compounding – easier to get them out of the mold) Water-soluble bases must contain water absorption characteristics (water and in body absorption). We need viscosity (in liquid form), because if suppository does not dissolve in water, we need to suspend the AI, so we need viscosity to evenly distribute particles in the suppository. (different than suspension because we cannot shake it to re-dispense particles, it’s solid), but can’t be too high of viscosity because we still need pourability when making suppositories |
|
|
T/F: Contraction characteristics is not a desired feature for a suppository base, because we prefer the suppository not to change size |
FALSE |
|
|
Classification of Suppository Bases: Fatty or oleaginous base |
- Theobroma oil - Synthetic triglyceride mixtures |
|
|
Classification of Suppository Bases: Water-soluble and water-miscible bases |
- Glycerinated gelatin - Polyethylene glycols |
|
|
Classification of Suppository Bases: Miscellaneous bases |
- Polyoxyl 40 stearate |
|
|
T/F: Polyoxyl 40 stearate is a water-miscible base |
FALSE |
|
|
Suppositories: Oleaginous Bases |
- Mostly used in rectal suppositories - Seldom (rarely) used in vaginal suppositories |
|
|
Oleaginous Bases Advantages |
- Nonirritating to sensitive membrane tissues - Excellent emollient - Available in grated form |
|
|
Oleaginous Bases Disadvantages |
- May give poor and somewhat erratic release of some drugs - Store products under refrigeration to avoid softening or melting prior to use - If cocoa butter used, then overheating is an issue - Melting procedure is slow Sometimes the release profile is hard to be predicted, so it may cause erratic release. We don’t want them to become soft (we need to controlled temperature), so they don’t melt in our hands. |
|
|
T/F: Oleaginous bases are usually used in vaginal suppositories |
FALSE Usually used in rectal suppositories |
|
|
Suppositories: Theobroma Oil (Cocoa Butter) Base |
- Pale-yellow, edible vegetable solid fat having a faint, agreeable chocolate-like odor - Extracted from the roasted seed of Theobroma cacao - A triglyceride primarily of oleopalmitostearin & oleodistearin - Polymorphic; thus capable of existing in 4 polymorphic forms (γ, α, β, β') - Certain drugs (Chloral hydrate) decrease the MP of theobroma oil ==> Substituting a portion of the cocoa butter with a wax with higher MP (White wax, acetyl esters wax) |
|
|
Theobroma Oil Polymorphic Forms |
Polymorphic form -- MP - γ ------- 18˚C - α ------- 22˚C - β' ------- 28˚C - β ------- 34.5˚C β form is the most desirable form, most chemically stable form, is the natural form |
|
|
T/F: The alpha form of CB is the natural form and has the highest MP of all the polymorphs |
FALSE β is natural form, and has highest MP |
|
|
T/F: Substitution of a portion of the CB with a wax, such as White Wax or Cetyl Esters Wax can reduce the MP of the base |
FALSE We increase the MP. Chloral hydrate decreases the MP of CB, so in order to increase the MP of the mixture, we add a wax with a higher MP. |
|
|
Suppositories: Water-Soluble Bases |
- Primarily used for vaginal or urethral suppositories - DISSOLVE in body fluid but not melt at body temperature |
|
|
Water-Soluble Bases Advantages |
- Can be melted using a microwave - Provide more reliable release of drug - Carefully monitored storage temperatures NOT required We can only use microwave in water-soluble bases (cannot in oleaginous bases) Water-soluble suppositories do not need to be refrigerated. |
|
|
Water-Soluble Bases Disadvantages |
- Irritating to body cavity tissues - Interact with polystyrene, the plastic often used for prescription vials Polystyrene: most used plastic in suppository dosage form |
|
|
T/F: Water-soluble suppository base can be melted using a microwave. |
TRUE |
|
|
Suppositories: Polyethylene Glycol Bases |
- PEGs are polymers of ethylene oxide and water, prepared to various chain lengths, molecular weights, and physical states - Available in a number of MW ranges - Various combination of these PEGs may be combined by fusion, using two or more of the various types to achieve a suppository base of desired consistency and characteristics - DISSOLVE slowly in body's fluids (does NOT melt at body temperature) PEG higher than 1000 MW: solid PEG lower than 1000 MW: liquid |
|
|
T/F: PEG bases melt at body temperature |
FALSE - They dissolve |
|
|
Suppositories: Glycerinated Gelatin Bases |
- Gelatinous preparation made from gelatin, glycerin, and water - Have a tendency to adsorb moisture due to hygroscopic nature of glycerin - Most frequently used in the preparation of vaginal suppositories, where the prolonged localized action of the medicinal agent is usually desired |
|
|
T/F: Glycerinated gelatin bases have a tendency to adsorb moisture |
TRUE |
|
|
Miscellaneous Bases |
- Mixtures of oleaginous and water-soluble or water-miscible materials - May be chemical or physical mixtures - Some are preformed emulsions, generally of the w/o type |
|
|
T/F: Some of the miscellaneous suppository bases are preformed as emulsions, generally oil-in-water type. |
FALSE - Generally w/o type |
|
|
Polyoxyl 40 Stearate |
- Waxy, white to light tan solid that is water-soluble. Its MP is generally between 39°C and 45°C - Mixture of the mono-esters and di-esters of stearic acid or purified stearic acid with polyoxyethylene diols - Average polymer length being equivalent to about 40 (MW) oxyethylene units |
|
|
T/F: The MP of polyoxyl 40 stearate is lower than the normal body temperature. |
FALSE Body temperature: 38°C MP: 39°C-45°C So, MP > body temp. |
|
|
Preparation Methods of Suppositories: Hand-Rolling |
A plastic-like mass is prepared by triturating grated cocoa butter and AIs in a mortar |
|
|
Preparation Methods of Suppositories: Compression Molding |
A mixed mass of grated suppository base and medicaments are forced into a special compression mold |
|
|
Preparation Methods of Suppositories: Fusion and Molding |
Melting the suppository base, and then dispersing or dissolving the drug in the melted base Melting the base => Incorporating API => Pouring to the molds => Cooling and congealing => Removing from molds API: active pharmaceutical ingredient If viscosity is too high, it won’t flow (can’t pour). If flow is too high, the AI won’t be suspended (won’t be evenly distributed), and you can’t overfill the mold -Remember to lubricate the mold |
|
|
Preparation of Suppositories - Molds |
- Commercially available molds can produce individual or large numbers of suppositories of various shapes and sizes - Made from metal, such as stainless steel, aluminum, and brass, or plastic - Can be reusable or disposable |
|
|
Preparation of Suppositories - Lubrication |
- Suppository molds may require lubrication before the melt is poured to facilitate clean and easy removal of the molded suppositories - Rarely necessary when the suppository base is cocoa butter or PEG - Usually necessary when glycerinated gelatin suppository are prepared With steel or metal mold: we MUST lubricate (if we don’t, it will be too hard to remove suppository from mold) Lubricate the mold LIGHTLY. We cannot use too much lubricant in the cavity because the excess amount of lubricant will flow down the suppository mold, and when we pour the melted bases then it will remove the tip (bottom) of the suppository, so the suppository won’t be made correctly (dose won’t be accurate). We must use a small amount with a Q-tip, to prevent this from happening. |
|
|
T/F: You can drop several drops of lubricants to the suppository mold for lubrication purpose. |
FALSE - Only lubricate lightly. |
|
|
Preparation of Suppositories: Determination of Base Amount |
VBase = Vmold - Vdrug In order to find out the volume of the base, we need to know total volume of mold and volume of drug (we use volume, NOT weight) |
|
|
Preparation of Suppositories: Calibration |
- Each individual mold is capable of holding a specific volume of material in each of its openings - Pharmacist should calibrate each suppository mold for the usual base so as to prepare medicated suppositories each having the proper quantity of medicaments Base only => Weight of suppositories => Average and error Use blank suppositories to calibrate, then you can use medicated base to fill in the cavities |
|
|
Preparation of Suppositories: Calibration Equation |
WBase = Wmold - Wdisplaced WBase: weight of base required Wmold :weight of blank suppositories Wdisplaced : weight of base displaced by drug Density*Volume = Weight |
|
|
Case Study: If 12 mL of CB are required to fill a suppository mold and if the medicaments in the formula have a collective volume of 2.8mL, how many grams of CB is required? (Density of CB is 0.86g/mL) |
Vbase = Vmold - Vdrug Vbase = 12mL - 2.8mL Vbase = 9.2mL Wbase = Vbase * densitybase Wbase = 9.2mL * 0.86g/mL = 7.91g |
|
|
Case Study: If 2mL of PEG base are required to fill a suppository mold cavity and if the medication in the formula for each suppository have a collective volume of 0.2mL, how many grams of PEG is required? (density of PEG is 1.36g/mL) |
Vbase = Vmold - Vdrug Vbase = 2mL - 0.2mL Vbase = 1.8mL Wbase = Vbase * densitybase Wbase= 1.8mL * 1.36g/mL = 2.45g |
|
|
Density Factor (DF) |
- When a drug is placed in suppository base, it should displace an amount of base as a function of its density - DF is used to determine how much base a drug will displace - DF = "the weight of drug, in grams, that will displace 1g of base" - DF will be specific for a drug in a particular base - If the DF is not specified for a drug, assume the base is cocoa butter |
|
|
Density Factor Determination |
- Double cast method - Paddock method |
|
|
Density Factor Determination: Double Casting Technique |
- Initially, only partially fill cavities by drug mixture - Afterward, use blank base to fill remaining of cavities (must overfill them) - Then trim suppositories to make weight accurate - Melt suppositories, so drug is evenly distributed throughout the dosage form. - Refill cavities and wait for suppositories to re-solidify - Extract suppositories The tip of the suppositories is more dense (has drug) so it's a different color (more concentrated) compared to the excess blank base |
|
|
Information Needed to Calculate DF |
- Average weight of blank suppository - Average weight of drug-containing suppository - Amount of drug in each suppository |
|
|
Case Study: A prescription calls for 0.3g of Drug Z in a Polybase vaginal suppository. We check the literature but cannot find a published DF for Drug Z in Polybase. What should we do? |
- Determine the weight of a blank Polybase suppository using our aluminum mold - Pour 6 blank suppositories and determine their average weight to be 2g - Begin the double casting technique as previously described, pouring 6 suppositories - Total amount of drug needed to prepare 6 suppositories, each containing 0.3g, is 1.8g of Drug Z - Upon completing the double casting technique, we find that the average weight of a medicated suppository, is 2.1g Wbase/med supp = Wmed supp - Wdrug/supp 1.8g = 2.1g - 0.3g Wbase displaced = Wblank - Wbase/med supp 0.2 = 2g - 1.8g **1.8 comes from equation above, NOT from 0.3*6 for above bullet point DF is weight of drug displaced per gram of base DF = 0.3g/0.2g = 1.5 |
|
|
Density Factor Determination: Paddock Method |
- Determine average blank weight (A) per suppository using the mold and suppository base of interest - Weigh quantity of base necessary for 10 suppositories - Weight 1g of drug. The weight of drug per suppository (B) is then equal to 0.1g - Melt suppository base and incorporate drug, mix, pour into mold, cool, trim and remove from mold - Weigh the 10 suppositories and determine average weight (C) - Determine DF as follow: DF = B/(A-C+B) This is a better method (more accurate). We need to trim because of the volume of the drug, so the final weight is more accurate - A: blank supp. weight - B: drug weight - C: average weight of medicated supp. |
|
|
Case Study: Prepare a suppository containing 120mg of phenobarbital (DF=1.2) using CB as base. The weight of the blank CB suppository is 2g. What will be the total weight to each suppository? |
Replacement factor = Drug amount / DF Replacement factor = 0.12g/1.2 = 0.1g Wbase = 2g - 0.1g = 1.9g Total weight = 1.9g + 0.12g = 2.02g |
|
|
Case Study: Prepare 12 boric acid 300mg suppositories using CB, where the average weight of the CB blank is 2g and the average weight of the medicated suppository is 2.1g. What is the DF of boric acid? |
Replacement Factor = Drug amount/DF
DF = Drug amount/Replacement factor Wbase = 2.1g - 0.3g = 1.8g RF = 2g - 1.8g = 0.2g DF = 0.3g/0.2g = 1.5 |
|
|
Packaging Suppositories |
- Glycerin suppositories and glycerinated gelatin suppositories are packaged in tightly closed glass containers to prevent a moisture chance in the content of the suppositories - Suppositories prepared from a CB base are usually individually wrapped or otherwise separated in compartmentalized boxes to prevent contact and adhesion |
|
|
Suppositories Storage |
- Necessary to maintain suppositories in a cool place - Suppositories having CB as base must be stored below 30°C, and preferably in refrigerator (2~8°C) - Glycerinated gelatin suppositories are best stored at temperatures below 8°C and can routinely be stored at controlled room temperature (20~25°C) - Suppositories made from PEG base may be stored at usual room temperature PEG and glycerinated are both water-soluble |
|
|
Suppository Application |
- If suppositories must be stored in refrigerator, should be allowed to warm to room temperature before insertion - Patient should be advised to rub CB suppositories gently with fingers to melt the surface, to provide lubrication for insertion - Glycerinated gelatin or PEG suppositories should be moistened with water to enhance lubrication CB is relatively non-irritant, so warming may not always be necessary. - For glycerinated gelatin or PEG: must be warmed because they have a higher chance of irritation |
|
|
Solubility |
- Concentration of solute in a saturated solution at certain temperature - Like dissolves like Saturated: maximum amount dissolved (‘equilibrium’: amount of solute going into solution and being re-crystallized is the same) - It has to be at a certain temperature, otherwise the solubility is not fixed -Like dissolves like: oil dissolves fat or water dissolves aqueous |
|
|
Solubility Designations in USP |
Very soluble: >10^6µg/mL Freely soluble: 10^5 - 10^6 µg/mL Soluble: 3.3*10^4 - 10^5 µg/mL Sparingly soluble: 10^4 - 3.3*10^4 µg/mL Slightly soluble: 10^3 - 10^4µg/mL Very slightly soluble: 100 -1000µg/mL Practically insoluble: <100µg/mL |
|
|
Minocycline has a solubility of 50mg/mL. It is a _________ drug according to the definition in USP? |
Soluble 50mg/mL * 1000 = 5^4µg/mL |
|
|
Solubility and Particle Size Equation |
log S/S0 = [2γV] / [2.303RTr] - S: solubility of particles - S0: solubility of solid - γ: surface tension - V: molar volume - R: gas constant - T: absolute temperature - r: radius of particles |
|
|
Solubility and pH |
Solubility of weak electrolytes can be affected by pH |
|
|
Solubility and pH: For weak acid |
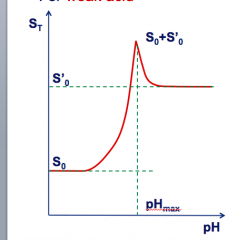
- Ionized at higher pH (charged) - will dissolve better - Unionized at lower pH (uncharged) - will absorb better S0: intrinsic solubility of solute S’0: solubility of salt form S0 + S’0: pH max |
|
|
Solubility and pH: For weak base |
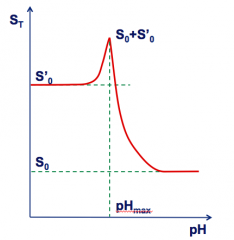
- Ionized at lower pH (charged) - will dissolve better - Unionized at higher pH (uncharged) - will absorb better S0: intrinsic solubility of solute S’0: solubility of salt form S0 + S’0: pH max |
|
|
T/F: The solubility of a weak base increases when the pH increases. Assume the pH is higher than the pH max. |
FALSE - Weak base: Solubility decreases with increasing pH |
|
|
Cosolvent System of Solutions |
Adding a cosolvent to aqueous phase sometimes increases solubility dramatically Ex. Adding alcohol cosolvent in phenobarbital solution: Initial solubility of phenobarb: 0.1g/100mL After addition: - Alcohol: 22% + - Glycerin: 40% - Water: 38% Solubility of phenobarb: 1.5g/100mL |
|
|
Temperature and Solubility |
- Dissolution is usually an endothermic process - Exception: Calcium hydroxide falls slightly from a solubility of 0.185g/mL at 0°C to 0.077g/mL at 100°C Endothermic: this process needs to absorb heat (when you increase temperature, you usually increase solubility) |
|
|
Pharmaceutical Solutions |
Solutions in pharmacy is mostly involved with: - Solids dissolved in liquids - Liquids mixed (miscible) in liquids One of the oldest dosage forms known |
|
|
Why Solutions? |
- Enteral feeding requires liquids for infant, pediatric, geriatric, and some psychiatric patients - Oral liquids are more diverse and have varying dosage strengths/quantities - Greater bioavailability from oral liquids as compared to solids More diverse: we can manipulate dosing (various ranges - take xmg/mL - unlike tablets which have set dose) |
|
|
Solutions: Advantages |
- Bioavailability: Since drugs must be in a solution form before it can be absorbed, this dosage form can be more effective compared to solid dosage dosage form with regard to bioavailability - Many patients (children & elderly) cannot swallow tablets or capsules - Medication is uniformly or homogeneously distributed throughout the preparation - Some drugs are irritating to the gastric mucosa when administered as a large dose through tablet and capsule dosage form. This irritation may be reduced when the drug is administered via solution dosage form because of dilution factor - Solutions can be easily flavored, sweetened, and colored In solution dosage form, it's more diluted (if compared to tablets, which cause greater GI irritation since tablets are very concentrated) |
|
|
T/F: The tablet has less irritation of GI tract compared to solution when a large dose is given |
FALSE - Tablet has more irritation |
|
|
Solutions: Disadvantages |
- Because of bulkiness and liquid nature, it's NOT an easy and convenient dosage form to carry around - It is NOT always easy to prepare solutions for drugs that possess obnoxious taste or odor - Drugs are likely to undergo deterioration much faster, and thus lose potency Some AI have bad taste or odor, so it's not easy to make it as solution (unless we add a flavoring agent). For drugs that can be easily degraded in stomach or GI tract enzymes, solution is not ideal (tablets may be a better dosage form in this case because it takes longer to degrade, so it may pass through these environments) |
|
|
T/F: The drug formulated in solution usually tends to degrade compared to that formulated as suspensions. |
TRUE |
|
|
Solutions: Pharmaceutical Solvents |
- Alcohol, USP - Diluted Alcohol, NF - Alcohol, Rubbing - Glycerin, USP - Isopropyl Rubbing Alcohol - Propylene Glycol, USP - Purified Water, USP These are non-sterile solvents required for oral dosage forms (Parenteral injections require other solvents) |
|
|
Solutions: Solvents & Co-solvents for INTERNAL Use |
- Water - Alcohol - Glycerin - Propylene Glycol - Syrups |
|
|
Solutions: Solvents & Co-solvents for EXTERNAL Use |
- Water - Acetone - Ether - Alcohol - Oils |
|
|
Which solvents or co-solvents can NOT be used internally in formulations? |
Acetone & Ether External use only!!! |
|
|
T/F: Alcohol as co-solvent may be incorporated for internal and external use. |
TRUE |
|
|
Alcohol, USP |
- Alcohol is the most useful solvent in pharmacy next to water. USP, is 94.9 to 96% C2H5OH by volume (i.e., v/v) - Together with water it forms as hydroalcoholic mixture that dissolves both alcohol-soluble and water-soluble substances, a feature especially useful in the extraction of active constituents from crude drugs - Alcohol is frequently used with other solvents, such as glycols and glycerin, to reduce the amount of alcohol required - Also used in liquid products as antimicrobial preservative alone or with parabens, benzoates, sorbates, and other agents - However, concern has been expressed over the undesired pharmacologic and potential toxic effects of alcohol Alcohol USP: Usually 95% in drugs in market - There's hygroscopic alcohol (can adsorb moisture from environment) - There's anhydrous alcohol (does not contain any water in its molecular form) We allow some range in alcohol volume because alcohol may be lost upon storage |
|
|
T/F: The alcohol concentration of Alcohol, USP is 70% |
FALSE It's 95% |
|
|
OTC Age & Alcoholic Limit |
--------- Age ---------------- Alcoholic Limit - Children < 6yrs of age --- 0.5% - Children 6-12yrs of age --- 5% - >12yrs of age & adults --- 10% |
|
|
T/F: The alcohol limitation of a OTC med for a child is 5% |
FALSE - Depends on age |
|
|
Diluted Alcohol, NF |
- Prepared by mixing equal volumes of Alcohol, USP, & Purified Water, USP - Strength of Diluted Alcohol, NF is not exactly half that of the more concentrated alcohol but slightly greater, approx. 49% - It is NOT a useful hydroalcoholic solvent in many pharmaceutical preparations We mix Alcohol, USP (95%) with Purified Water, USP - concentration is 49% because the concentration of alcohol is higher than purified water concentration (greater than half (47.5%)) |
|
|
T/F: The strength of Diluted Alcohol, NF is exactly half that of Alcohol, USP. |
FALSE - It's slightly higher |
|
|
Glycerin, USP |
- Clear, syrupy liquid with a sweet taste - Miscible with water & alcohol - Has preservative qualities - Often used as stabilizer & as auxiliary solvent in conjunction with water or alcohol - Used in many internal preparations Can be used for internal and external preparations |
|
|
T/F: Glycerin can be used as preservative, stabilizer, and co-solvent |
TRUE |
|
|
Rubbing Alcohol |
- Isopropyl rubbing alcohol is about 70% by volume isopropyl alcohol, the remainder consists of water with or without color additives, stabilizers, and perfume oils - Used EXTERNALLY as rubefacient and soothing rub and as vehicle for topical products |
|
|
T/F: Rubbing alcohol can be used internally |
FALSE - External use only!!! |
|
|
Propylene Glycol, USP |
- Viscous liquid, miscible with water & alcohol - Useful solvent with wide range of applications and is frequently substituted for glycerin in modern pharmaceutical formulations Syrupy appearance. Contains better stability than glycerin |
|
|
T/F: Propylene Glycol, USP can be used as preservative, stabilizer and co-solvent |
TRUE - Can substitute glycerin |
|
|
Purified Water, USP |
- Obtained by distillation, ion exchange treatment, reverse osmosis, or other suitable process - Prepared from water complying with the federal Environmental Protection Agency with respect to drinking water Most important solvent in pharmaceutical preparations |
|
|
Purified Water, USP compared with ordinary drinking water: |
- Purified Water, USP is more free of solid impurities - When evaporated to dryness, it must NOT yield greater than 0.001% of residue (1mg of total solids per 100mL of sample evaporated) - Purified Water, USP is intended for use in the preparation of aqueous dosage forms, EXCEPT those intended for parenteral administration (injections) Purified Water, USP: has less solid impurities (though some impurities still exist) |
|
|
Water Purification Methods |
- Distillation - Ion-exchange - Reverse osmosis |
|
|
Water Purification Methods: Distillation Method |
- The first portion of aqueous distillate (10-20%) MUST be discarded - The last portion of water (10%) remaining in the distillation apparatus MUST be discarded and not subjected to further distillation We supply water (entered in inlet), which is regulated by Environmental Protection Agency. Water is heated by heating coil; the vapor is taken by condensing coil. After that, water is cooled by cooling fan, and goes into distilled water container. Even after this process, there are still some impurities. |
|
|
Water Purification Methods: Ion-Exchange Method |
- On a large or small scale, the ion-exchange method for the preparation of purified water offers a number of advantages over the distillation method - The ion-exchange process permits ease of operation, minimal maintenance, and a more mobile facility There are two chambers. Water (neutral pH) enters the Cation Exchange Bed (Cation Free Water) chamber; cations from solute are removed which increases [H+] and lowers the pH (acidic). In the Anion Exchange Bed chamber (demineralized water), anions are exchanged with OH- after water goes through the first chamber, and pH becomes neutral again and the process of purification is finalized. |
|
|
T/F: Cation free water has higher pH compared to the inlet water in the ion-exchange method |
FALSE - pH is lower in cation free water |
|
|
Water Purification Methods: Reverse Osmosis |
- A pressured steam of water is passed parallel to the inner side of a filter membrane core - A portion of the feed water permeates the membrane as filtrate - The water that has passed through the system is referred to as concentrate - The flow in this crossflow system is from a more concentrated to a less concentrated solution, thus the term reverse osmosis Water passes through a semipermeable membrane (cross-flow filter membrane), impurities do not pass. Reverse osmosis: water moves from higher solute concentration to lower concentration (regular osmosis: water moves to higher solute concentration) |
|
|
T/F: The flow in this cross-flow system (reverse osmosis) is from a more concentrated to a less concentrated solution |
TRUE |
|
|
Reverse Osmosis: Cross-flow filter membranes remove particles defined in the range of: |
- Microfiltration: 0.1 - 2 microns (bacteria) - Ultrafiltration: 0.01 - 0.1 microns (virus) - Nanofiltration: 0.001 - 0.01 microns (organic compounds in MW range of 300-1000) - Reverse osmosis: particles smaller than 0.001 microns Reverse osmosis creates most purified water |
|
|
Pharmaceutical Solutions for Pharmacists |
- Syrups - Elixirs - Aromatic waters - Tinctures - Spirits - Injections Sterile compounding: injections and ophthalmic solutions |
|
|
Syrup |
- Concentrated or nearly saturated solution of sucrose in water - Simple syrup contains ONLY sucrose and purified water (Syrup USP) - Syrups containing pleasantly flavored substances are known as flavoring agents - Medicinal syrups are those to which therapeutic compounds have been added - Syrups have a lower solvent power than water and "salting out" may be a problem Simple syrup: Amount or % of sucrose can be more or less,but only sucrose. Flavoring syrups are different than simple syrup (contains sucrose, water, flavoring substances). Medicinal syrups: contain drugs. When syrup is used instead of water, than ‘salting out’ may be a problem (ends up being a suspension instead of solution). |
|
|
T/F: A simple syrup contains sucrose, purified water, and flavoring substances |
FALSE - Only contains sucrose and purified water |
|
|
Preparation of Syrups: Solution with the aid of heat |
- Quickest - Not applicable to temperature sensitive or volatile APIs - Temperature must be carefully controlled to avoid decomposing and darkening the syrup If substances are temperature sensitive or are volatile, heat will accelerate degradation of materials (method cannot be utilized) |
|
|
Preparation of Syrups: Solution by agitation without the aid of heat |
- Time consuming - Maximum stability |
|
|
Preparation of Syrups: Addition of sucrose to a liquid medication |
- Sometimes may cause precipitation If you add sucrose to another medicated liquid, precipitation may happen because of ‘salting out’ propertiesof the syrup |
|
|
Preparation of Syrups: Percolation |
- Purified water or the medication pass through the bed of crystalized sucrose Percolation (think of coffee machine): One bag of sucrose => water flows through sucrose bag => and syrup is made. (Why crystalized sucrose? Because when liquid passes through it, sucrose is dissolved slowly) (Different from sucrose powder) |
|
|
T/F: Syrups prepared by heat have better stability compared to those prepared by agitation |
FALSE - Agitation is most stable |
|
|
Preserving Syrups |
- Syrup USP (sp gr = 1.313, 85% w/v, 65% w/w) is protected from bacterial contamination by virtue of its high solute concentration - More dilute syrups are good media microbial growth and require the addition of preservatives - To formulate a syrup containing less sucrose, the quantity of alcohol, or other preservatives, can be estimated by considering the USP syrup equivalent and the free water equivalent - Free water is preserved by 18% alcohol |
|
|
What is the specific gravity and concentration of Syrup USP in w/v and w/w? |
- Specific gravity = 1.313 - Concentration: 85% w/v, & 65% w/w |
|
|
USP Syrup Equivalent & Free Water Equivalent |
- In Syrup, USP 850g sucrose occupes an apparent volume of 550mL, then each gram of sucrose will occupy 550/850 or 0.647mL - 850g sucrose preserves 450mL of water, then each gram of sucrose will preserve 450/850 = 0.529mL of water - Free water is preserved by 18% alcohol - If glycerin is present, its volume preserves an equal volume of free water. If propylene glycol is present, it is considered equivalent to ethanol |
|
|
How much Alcohol, USP is required to preserve 1L of syrup containing 500g sucrose? |
V preserved by sucrose = 500g * 0.529mL/g = 265mL V occupied by sucrose = 500g * 0.647mL/g = 324mL Free water equivalent = 1000mL - 265mL - 324mL = 411mL V of pure alcohol required = 411mL* 18% = 74mL V of Alcohol, USP = 74/95% = 78mL |
|
|
How much Alcohol, USP is required to preserve 200mL of syrup containing 80g of sucrose? |
V preserved by sucrose = 80g * 0.529mL/g = 42.32mL V occupied by sucrose = 80g * 0.647mL/g = 51.76mL Free water equivalent = 200mL - 42.32mL - 51.76mL = 105.92mL V of pure alcohol required = 105.92mL * 18% = 19.06mL V of Alcohol, USP = 19.06/95% = 20mL |
|
|
Elixirs |
- Clear, sweetened, hydroalcoholic liquids intended for oral use - Their alcohol content ranges from 5 - 40% (10 - 80 proof). The concentration of alcohol is determined by the amount required to maintain the drug or volatile oil in solution - Glycerin often is added to enhance the solvent properties - The addition of aqueous solutions to elixirs may cause turbidity or separation by lessening the alcohol concentration |
|
|
T/F: The alcohol content range of the elixir is from 5-40 proof |
FALSE - It's 10-80 proof |
|
|
Preparation of Elixirs: by Simple Solution |
- Most common elixir vehicle is aromatic elixir - Some syrups now contain alcohol, so the distinction between syrups and elixirs is sometimes vague |
|
|
Preparation of Elixirs: by Mixture of 2 Liquid Ingredients |
- Dissolve alcohol soluble ingredients in the alcohol - Dissolve water soluble ingredients in the water - Add the AQUEOUS phase to the ALCOHOL solution (do NOT make the reverse) If reversed, drug will precipitate out |
|
|
When Preparing Elixirs, Consider... |
- Consider whether the salt of the drug or the free acid or base form should be used - Glycerin and propylene glycols can be used as cosolvents |
|
|
T/F: When you prepare elixirs by mixing two liquids, it's actually to add the aqueous phase to the alcohol solution |
TRUE |
|
|
Elixirs Trouble Shooting: Frequently the final mixture is not clear. What is the reason behind this? |
- An excess of aromatic oils may have been added Oil is used to enhance the order of the preparation |
|
|
Elixir Trouble Shooting: What can you do if the obtained solution is cloudy? |
- Talc filtration can be used - Add approximately 1 - 2g of talc per 100mL of solution, mixing and filtering Talc is porous, when we mix talkwith oil, the oil is adsorbed to talc (then talc becomes a filtration bed with a large surface area) |
|
|
Tinctures |
- Alcoholic or hydroalcoholic solutions prepared from vegetable materials or from crude chemical substances - Alcohol contents ranges from 15 - 80% (30 - 160 proof) Higher alcoholic contents than elixirs |
|
|
T/F: Tinctures are preparations by simply mixing the ingredients (already manufactured ingredients) with the solvent |
FALSE - It's usually prepared from crude, original materials |
|
|
Aromatic Waters |
- Saturated solutions of aromatic or volatile substances in water - They possess an odor similar to the plant or volatile substance from which they are made - Due to their pleasant odor, they are used as flavoring or perfuming vehicles in certain pharmaceutical preparations - Mostly exert NO therapeutic action - Can be internal or external vehicle |
|
|
T/F: Aromatic water usually has therapeutic function |
FALSE - NO therapeutic action |
|
|
Preparation: Solution Method - Shaking |
- 2g (or 2mL if liquid) of volatile substance with 1000mL of purified water for 15 min - Set aside for 12hr, filtered through wetting filter paper |
|
|
Preparation: Solution Method - Talc |
- Incorporating thoroughly 2mL volatile oil with 15g of talc or with sufficient quantity of purified siliceous earth - Adding 1000mL water gradually - Filtering the water and adjusting to 2000mL |
|
|
T/F: When the aromatic water is prepared by talc, talc is mixed with water |
FALSE - Talc is mixed with volatile oil |
|
|
Spirits |
- Alcoholic or hydroalcoholic solutions of volatile substances - Alcoholic concentration of spirits is usually 60% - Spirits can contain a greater concentration of volatile substances than the corresponding aromatic waters - Can be used internally or externally |
|
|
Ophthalmic Preparations |
- Specialized dosage forms designed to be instilled onto the external surface of the eye (topical), administered inside (intraocular) or adjacent (periocular) to the eye or used in conjunction with an ophthalmic device - Most commonly employed ophthalmic dosage forms are solutions, suspensions, and ointments - These preparations when instilled into the eye are rapidly drained away from ocular cavity due to tear flow and lacrimal nasal drainage - The newest dosage forms for ophthalmic drug delivery are: gels, gel-forming solutions, ocular inserts, intravitreal injections and implants Including contact lenses |
|
|
Ophthalmic Factors Affecting Drug Availability |
- Rapid solution drainage by gravity, induced lachrymation, blinking reflex, and normal tear turnover - Superficial absorption of drug into conjunctiva and sclera, and rapid removal by peripheral blood flow - Low corneal permeability (act as lipid barrier) |
|
|
T/F: The slower the peripheral blood flow of the eye,the poorer the absorption of drug into the conjunctiva and sclera |
FALSE - Blood flow is not good for the absorption of drug because the drug is removed faster so absorption becomes poorer. If the blood flow is slower, the absorption should be better (not poorer) |
|
|
Ophthalmic General Safety Consideration: Sterility |
- Ideally, all ophthalmic products should be terminally sterilized in the final packaging - Only a few ophthalmic drugs formulated in simple aqueous vehicles are stable to normal autoclaving temperatures and times (121°C for 20-30 min) - Such heat-resustant drugs may be packaged in glass or other heat-deformation-resistant packaging and thus can be sterilized in this manner Ideally, after manufacturing, packaging, and sealing, the whole thing has to be sterilized. Not all ophthalmic preparations can be sterilized by autoclaving, such as heat-sensitive drugs. |
|
|
T/F: Ophthalmic preparations should be terminally sterilized in the final packaging |
TRUE |
|
|
General Safety Considerations: Ocular Toxicity & Irritation |
- Albino rabbits are used to test ocular toxicity and irritation of ophthalmic formulations - The procedure based on examination of the conjunctiva, the cornea or the iris |
|
|
General Safety Considerations: Ocular Toxicity & Irritation - Ex. USP procedure for plastic containers |
- Containers are cleaned and sterilized as in the final packaged product - Extracted by submersion in saline and cottonseed oil - Topical ocular instillation of the extracts and blanks in rabbits is maintained and ocular changes are examined |
|
|
General Safety Considerations: Preservation and Preservatives |
- Preservatives are included in multiple-dose eye solutions for maintaining product sterility during use - Preservatives NOT included in unit-dose package - Use of preservatives is prohibited in ophthalmic products that are used for eye surgery - Most common organism that grows in the cornea and cause loss of vision is Pseudomonas aeruginosa |
|
|
T/F: Both unit-dose eye solutions and ophthalmic products for eye surgery need preservatives |
FALSE - Unit-dose: not included - Eye surgery products: prohibited use |
|
|
T/F: Ophthalmic preparation used at eye surgeries should be packaged in multiple-dose containers |
FALSE - You have to use preservatives in multiple dosage containers and we cannot do that in surgery |
|
|
Ideal Ophthalmic Delivery System |
- Good corneal penetration - Prolong contract time with corneal time tissue - Simplicity of instillation for patient - Non-irritative and comfortable form - Appropriate rheological properties |
|
|
Topical Eye Drops |
- Selection of the appropriate salt form depends on: ==> Solubility, ocular toxicity, pH, tonicity, buffer capacity, compatibility, irritation - Most common salt forms used: ==> Hydrochloride, sulfate, nitrate, phosphate - Salts that may be used: ==> Salicylate, hydrobromide, bitartrate |
|
|
Which salt forms are mostly recommended in ophthalmic solutions? |
HCl, sulfate, nitrate, phosphate SNiPH |
|
|
Topical Eye Drops |
- Solutions - Suspensions - Powder for reconstitution - Gel-forming solutions |
|
|
Topical Eye Drops: Solutions |
Ophthalmic solutions are sterile, essentially free from foreign particles, suitably compounded and packaged for instillation into the eye |
|
|
Topical Eye Drops: Disadvantages of Eye Solutions |
- Stays at eye surface for very short time - Retention of solution in eye is influenced by viscosity, hydrogen ion concentration and instilled volume - Poor bioavailability (major portion, i.e., <75% is lost via nasolacrimal drainage) - Instability of dissolved drug - Necessity of using preservatives |
|
|
Topical Eye Drops: Suspensions |
What drugs? - Not sufficient water solubility - Not good stability in solution - Not good bioavailability The major topical ophthalmic suspensions are the steroid anti-inflammatory agents (Prednisolone acetate, dexamethasone, fluorometholone, and rimexolone) Ophthalmic suspension should use drug in microfine form - 95% or more of drug particles have a diameter of 10μm or less |
|
|
T/F: The drugs in topical eye solutions always have better bioavailability then those in ophthalmic suspensions |
FALSE - Opposite of suspensions in which solution has better bioavailability than suspension (in this case, particles are dissolved in the liquid medium) - In ophthalmic preparations, bioavailability depends on the dosage form itself and on contact time with the eyes (if drug can stay in target site longer, then definitely can increase chance of absorption and bioavailability is improved) |
|
|
Topical Eye Drops: Powders for Reconstitution |
What drugs? - Very limited stability in liquid form - Such as α- chymotrypsin and acetylcholine Manufactured by lyophilization: - Mannitol - Potassium acetate |
|
|
Topical Eye Drops: Gel-Forming Solutions |
- Liquid in container, but gel on contact with tear fluid - Enhanced contact time Mechanism: Temperature, pH, low sensitivity, lysozymes Ex. Timolol maleate gel-forming solution |
|
|
Ophthalmic Preparations: Osmotic Agents |
- Osmotic pressure equal to that of tear fluids, generally agreed to be equal to saline - Range is NOT fixed: ==> Range of 0.5 - 2% NaCl equivalency does not cause marked pain response ==> Range of ~ 0.7 - 1.5% should be acceptable to most persons - The eye seems to tolerate hypertonic solutions better than hypotonic ones - Common tonicity adjusting ingredients include: NaCl, KCl, dextrose, glycerin, PEG, mannitol, & buffer salts |
|
|
T/F: Mannitol is a commonly used tonicity-adjusting ingredient in ophthalmic preparations |
TRUE |
|
|
Rx Atropine Sulfate 2% NaCl qs Aqua. dist. q.s. ad. 30mL M. ft. ophthalmic solution Eatropine = 0.13 NaCl is used as osmotic agent |
0.9g/100mL = xg/30mL = 0.27g NaCl 2g/100mL = xg/30mL = 0.6g Atropine 0.6g * 0.13 = 0.078g (Atropine to NaCl equivalent) 0.27g - 0.078g = 0.192g (Amount of NaCl to add) |
|
|
Rx Atropine Sulfate 2% NaCl qs Aqua. dist. q.s. ad. 30mL M. ft. ophthalmic solution Eatropine = 0.13 , Eba = 0.50 Boric acid is used as osmotic agent |
0.9g/100mL = xg/30mL = 0.27g NaCl 2g/100mL = xg/30mL = 0.6g Atropine 0.6g * 0.13 = 0.078g (Atropine to NaCl equivalent) 0.27g - 0.078g = 0.192g (Amount of NaCl to add) 0.192g/0.50 = 0.384g (Amount of boric acid to add) |
|
|
Ophthalmic: pH Adjustments and Buffers |
- Render formulation more stable - Improve safety of product - Reduce irritation of product - Enhance aqueous solubility of drug - Enhance drug bioavailability - Maximize preservative efficacy (preservative does better in unionized form) |
|
|
Ophthalmic: Stabilizers |
- Ingredients added to a formula to decrease the degradation rate of the drug |
|
|
Ophthalmic: Antioxidants |
- Are principal stabilizers added to some ophthalmic solutions, primarily those containing epinephrine and other oxidizable drugs ==> Sodium bisulfite or metabisulfite are used in concentration up to 0.3% in epinephrine HCl and bitartrate solutions ==> Antioxidant systems consist of ascorbic acid, acetylcysteine, and sodium thiosulfate |
|
|
Which is the most common used stabilizer in eye drop preparations? |
Antioxidants |
|
|
Ophthalmic: Viscosity-Imparting Agents |
- Used to increase viscosity of ophthalmic solutions and suspensions - In suspensions, the agents are used to retard the sedimentation rate of the suspensoids - In ophthalmic solutions, the agents increase ocular contact time, decrease drainage rate, increase mucoadhesiveness, thus increasing drug bioavailability - A secondary benefit of the agents is lubricating effect - The major commercial viscous vehicles are hydroxypropyl methyl cellulose (Isopto) and polyvinyl alcohol (Liquifilm) |
|
|
T/F: Viscosity-imparting agents also serve as thelubricants in the eye drops. |
TRUE |
|
|
Ophthalmic Vehicles |
- Purified Water USP - Oils |
|
|
Ophthalmic Packaging |
- Eye drops have been packaged almost entirely in plastic dropper bottles (Drop-Tainer plastic dispenser) - Main advantages of Drop-Tainer: ==> Convenience of use by patient ==> Decreased contamination potential ==> Lower weight, and lower cost - Plastic bottle and dispensing tip is made of low-density polyethylene (LDPE) resin, which provides necessary flexibility and inertness - The cap is made of harder resin than the bottle |
|
|
Advantage of LDPE resin |
- Compatible with very wide range of drugs and formulation components |
|
|
Disadvantages of LDPE resin |
- Sorption and permeability characteristics (e.g., volatile preservatives (Chloramphenicol)) - Weight loss by water vapor transmission - Transluscent Compatibility must be inert - Some preservatives can permeate through the wall of container and formulation can be modified - Autoclave cannot be used to sterilize these bottles (plastic - heat sensitive) |
|
|
T/F: The eye drop bottle made by LDPE resin isusually sterilized by autoclave. |
FALSE - Because it’s plastic, it will go under weight loss if we use autoclave |
|
|
What drugs need glass bottle? |
- Drugs with special stability considerations - Powders for reconstitution - Sterilized by dry-heat or steam autoclave sterilization - Amber glass is used for light-sensitive products With glass bottles we can autoclave (not heat sensitive) |
|
|
T/F: Powders for reconstitution for eye use are usually packaged in LDPE resin containers |
FALSE - Can’t use for powder reconstitution because of manufacturing (we can only use glass-containers). Powders of reconstitutionis made through lyophilization (requires usage of glass container) |
|
|
Specific gravity of an alcohol that has a volume of 1000mL and weighs 810g |
810g/1000mL = 0.81 sp gr = g/mL |
|
|
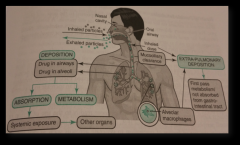
Pulmonary Drug Delivery |
- Drugs being delivered to the lungs - Long history: Atropa belladonna leaves; smoking marijuana - Achieved either by delivery through nose or oral cavity - Originally for local respiratory system but recently systemically - Ex. Proteins, amino acid peptides, steroids, cardiac agents, vaccines Pulmonarydrug delivery systems: most popular is through the mouth(very rarely aerosols are used through the nose) Flu inhaled vaccines can be used inpatients under 55. Patients over 55 can only take injectable flu shots becauseof toxicity |
|
|
T/F: Because of the large size of protein, they cannot be used for pulmonary delivery. |
FALSE - Best delivery way for protein and peptides because it avoids degradation |
|
|
Respiratory Tract Anatomy and Physiology |
- Respiratory tract starts at nose and ends at alveolar sac in lungs - Is divided into three regions: ==> Nasopharyngeal and Oropharyngeal ==> Tracheobronchial ==> Alveolar |
|
|
Branching of Airways |
- Symmetric series of dichotomous branches
- Every branching leads to "new generation" of airways - The further away from the mouth, the larger the area We use “generation” to determine how far the branching is, 1 generation is less farther than 10 generations Alveolar sac (furthest one) has largest surface area - Ex. The alveoli sac has 8X theamount of surface area than just a sphere |
|
|
Surface Area of Airways |
- Surface area of airways increases with increase in generation - It also increases with increasing distance of airways from the glottis - Diameter of airways decreases with increasing generation of airways |
|
|
T/F: Surface area of airways decreases with increasing distance of the airway from the glottis |
FALSE - It increases |
|
|
Pulmonary Drug Delivery Advantages |
- Rapid onset of action - Avoids first pass effect and degradation in GI tract - Lower dose that can minimize adverse reaction - Aerosol containers and valves are tamper-proof - Non-invasive, needle free - Can produce both systemic and local effect |
|
|
T/F: Pulmonary delivery usually has delayed onset of action compared to the oral dosage forms |
FALSE - Rapid onset of action |
|
|
Pulmonary Drug Delivery Disadvantages |
- Cost of device - Complex engineering to develop divide - Possibility of local side effects due to oropharyngeal deposition - Not suitable for drugs that do NOT get absorbed via pulmonary route - Lung barriers must be overcome by efficient deposition |
|
|
Pulmonary Drug Delivery: Factors Affecting Particle Deposition |
- Physiological factors -Tidal volume - Coordination of aerosol generation and inhalation - Breath holding - Disease states - Pharmaceutical factors -Tidal volume: volume of inhaled air one time -Coordination for aerosol generation and inspiration: must be trained -Patients needs to hold their breath for a few seconds after administration of medication |
|
|
Factors Affecting Particle Deposition: Physiological Factors - Lung Anatomy |
- Probability of deposition increases with each bifurcation - Particles have to pass through a series of branching tubes with decreasing diameter and constantly change direction to remain airborne - Thus, normal anatomical features of the lung can affect particle deposition as they influence particle velocity |
|
|
T/F: Probability of particle deposition increases with each bifurcation |
TRUE |
|
|
Factors Affecting Particle Deposition: Physiological Factors - Route of Particle Inhalation |
- If inhaled by nose, most particles are deposited in nose and pharynx - For pulmonary delivery, aerosols are administered via mouth and can reach the deeper lung - Formulation for nasal delivery should NOT be administered by mouth as nasal sprays produce larger droplets that cannot travel through the nasopharyngeal tract and deposit in lungs |
|
|
T/F: Pulmonary delivery dosage forms are inhaled through the mouth but not the nose. |
TRUE - Pulmonary delivery we inhale medications through our mouth (not the nose), unless we only need medication delivered to the nose. |
|
|
Factors Affecting Particle Deposition: Physiological Factors - Inspiratory Flow Rate |
- An increase in inspiratory flow rate (IFR) leads to: ==> Deposition in first few generations of airway ==> Increase in particle momentum and turbulence resulting in increased impaction in proximal tracheobronchial regions - Airflow changes with physical activity - Slow inhalation flow rate allows the aerosol to penetrate more readily to target receptor site in small peripheral airways (further branches) If patient increases IFR, the deposit of particles will stay in first few generations of branching in the lungs (more proximal). Patients must inhale slowly so the inhalation solution can reach the further generations of branching in the lungs |
|
|
Factors Affecting Particle Deposition: Physiological Factors - Tidal Volume |
- Volume of air inhaled in a single breath - Increase in tidal volume results in greater penetration of aerosol particles deeper into distal tracheobronchial and alveolar regions |
|
|
Factors Affecting Particle Deposition: Coordination of Aerosol Generation and Inspiration |
- For pressurized metered dose inhalers (pMIDs), the momentum of aerosol particles generated depends on the device rather than the patient's IFR - A failure in syncing between firing of pMDI and inspiration may cause enhanced oropharyngeal deposition and reduced entry into the deep lung |
|
|
T/F: For pressurized metered dose inhalers, themomentum of aerosol particles generated depends on the device rather than the patient’s IFR |
TRUE |
|
|
Factors Affecting Particle Deposition: Breath Holding |
- Time for sedimentation of particles can be extended by prolonging the interval between inspiration and exhalation - For efficient deposition, breath-holding for a period of 5 -10 seconds after inspiration is recommended |
|
|
T/F: For efficient deposition, breath holding for a period less than 5 seconds after inspiration is recommended |
FALSE - Hold breath for at least 5 seconds (5-10s) for efficient deposition |
|
|
Factors Affecting Particle Deposition: Disease State |
- Lung disease could lead to inflammation, bronchoconstriction or airway narrowing and this could affect the penetration, deposition and absorption of drugs to lungs - Bronchoconstriction and obstruction of airways may cause the airflow to divert to unobstructed airways - Narrowing of airways by mucus, inflammation or bronchial constriction can increase linear velocities, enhance inertial deposition and produce more deposition in central airways We increase linear velocity because theamount of air should be the same, even if the area of airway issmaller/narrower -If IFR increases, it goes intoproximal branches (oropharyngeal region) -If IFR decreases, it goes intodistal branches |
|
|
Factors Affecting Particle Deposition: Pharmaceutical Factors - Aerosol Velocity |
- For pMDIs: If droplet velocity is higher than IFR, the aerosol droplet is likely to deposit in oropharyngeal region
- For dry powder inhalers (DPI) and nebulizers, the aerosol droplet is carried by inhaled air, and thus aerosol velocity is controlled by IFR |
|
|
Factors Affecting Particle Deposition: Pharmaceutical Factors - Physical Stability |
- Particles may interact with each other due to attraction or repulsion - Hygroscopicity and solvent evaporation can also affect particle size Hygroscopicity: adsorption of water can affect size Evaporation: can decrease particle size |
|
|
Factors Affecting Particle Deposition: Pharmaceutical Factors - Size, Shape and Density of Inhaled Particles |
- Aerosol particle size is one of the most important factors in defining dose deposited and distribution of drug aerosol in lung - In general, formulation particles have irregular shapes with actual geometric diameter that are difficult to measure - Drug particles for pulmonary delivery are typically characterized by aerodynamic diameter rather than geometric diameter. The velocity at which the drug settles is proportional to aerodynamic diameter (AED) - Inhaled particles with unit density and diameter of 1-5 µm exhibit efficient penetration into lungs - Mass Median Aerodynamic Diameter (MMAD): Diameter of a sphere of unit density having the same settling velocity in air as the aerosol particle in question |
|
|
MMAD |
MMAD = d * [p / (p0 * x)]^1/2 - d = geometric mean diameter obtained from particle size analysis - po = reference density of 1g/cubcm - p = tapped density of inhaled particles - x = shape factor which is assumed to be 1 for spherical particles MMAD can be obtained from the cumulative distribution curve at the 50% point - Particle size vs. cumulative % less than stated size (So it is the particle size value on the y-axis when cumulative & less than stated size is 50%) |
|
|
Mechanism of Deposition of Inhaled Particles |
- Drugs are delivered as droplets or particles - Must be deposited in correct region and in the right quantity for efficacy - Mechanism of particle deposition from an inhaler to the respiratory tract involves a complex interplay between the dosage form and the structure of the tract - Three principal mechanisms for particle deposition in the lungs: ==> Inertial impaction ==> Gravitational sedimentation ==> Brownian diffusion |
|
|
Mechanism of Deposition of Inhaled Particles: Inertial Impaction |
- Greater than 5 µm in diameter - Inertial deposition increases with particle velocity, diameter, and density increase - It occurs in zones of highest airflow velocity, i.e., The first 10 generations (more proximal) |
|
|
Mechanism of Deposition of Inhaled Particles: Gravitational Sedimentation |
- Between 0.5 to 0.3 µm in diameter - Rate of sedimentation proportional to square of the particle diameter and varies with time and density - Deposition by sedimentation occurs where the air stream velocity is relatively low, usually last 5 to 6 generations - As deposition by sedimentation is time dependent, it mainly occurs in small airways |
|
|
T/F: Deposition by gravitation sedimentation mainly occurs in the lung periphery |
TRUE - Lung periphery = small distal airways |
|
|
Mechanism of Deposition of Inhaled Particles: Brownian Diffusion |
- Smaller than 0.5 µm in diameter - Deposition by diffusion increases with decrease in particle size, and breath-holding following inhalation - Important in bronchioles, alveoli, and bronchial bifurcations Inverse relationship: smaller particle size, greater deposition by diffusion |
|
|
T/F: Deposition by diffusion increases with increasein particle size |
FALSE - Increases with DECREASE in particle size (inverse relationship) |
|
|
Particle Deposition Pattern |
- Particles larger than 10µm deposit in the upper airways and are rapidly removed by coughing, swallowing and mucociliary processes - Inhaled particles between 5 - 10 µm diameter are deposited on the tracheobronchial surface by impaction - Particles between 0.5 - 5 µm are deposited in alveolar levels by impaction and sedimentation - About 50% of 0.5µm particles are deposited in the alveoli by diffusion and the rest are exhaled or may not deposit at all - Overall, particles with a diameter of 1 - 5µm show efficient penetration into the lungs |
|
|
Barriers to Pulmonary Absorption
|
- Mucus - Mucociliary Clearance - Alveolar Clearance |
|
|
Barriers to Pulmonary Absorption: Mucus |
- First barrier encountered by particles - Drug particles in dry powder inhaler first dissolve in mucus layer that contain 90-95% water - Dissolution in the mucus is the rate limiting step for absorption of POORLY water soluble drugs - Highly water soluble drugs may dissolve at very high relative humidity in the airways - Once in solution, the drug diffuses through the mucus layer and enters the aqueous environment of the epithelial lining fluid |
|
|
Barriers to Pulmonary Absorption: Mucus - Rate of diffusion through much depends on: |
- Thickness on mucus layer - MW of drug - Interaction between drug and mucus (i.e., binding of positively charged drugs with mucus glycoprotein) MW of drug determines size of drug, which has an inverse relationship with the diffusion coefficient |
|
|
T/F: Dissolution in the mucus is the rate-limitingstep for absorption of water-soluble drugs in the aerosols |
FALSE - Rate-limiting step for absorption of POORLY water-soluble drugs - Water-soluble drugs: dissolution procedure is very fast, so this step is fast; so it’s not rate-limiting step,but absorption is the rate-limiting step |
|
|
Barriers to Pulmonary Absorption: Mucociliary Clearance
|
- Self-cleansing mechanism of respiratory system - Elimination of fluid, microbes and particulates from respiratory tract due to ciliary function - Removed from respiratory tract within a few hours after being deposited |
|
|
Barriers to Pulmonary Absorption: Alveolar Clearance
|
- Particles deposited in alveolar region may be engulfed by macrophages - Engulfed particles may then be eliminated via the lymphatic system or absorbed into the pulmonary circulation |
|
|
Fate of Inhaled Particles |
|
|
|
Aerosols
|
- Pressurized dosage forms that emit a fine dispersion of liquid and/or solid materials containing one of more AI in gaseous medium - Require same consideration with respect to formulation, stability and therapeutic efficacy - However, they depend on functioning of container and added component, propellant, to deliver medication Aerosol: liquid or solid in gas Propellant: key ingredient to deliver aerosol dosage form |
|
|
Aerosol Systems |
- Two-Phase System: propellant + AI (solution) - Three-Phase System: emulsion or suspension + propellant (dispension) |
|
|
Aerosol Components |
- Aerosol formulation consists of two components: ==> AI combined with required adjuncts like antioxidants, surfactants, solvents to prepare a stable and efficacious product ==> Propellant |
|
|
Propellant |
- When propellant is a liquefied gas or a mixture of liquefied gases (e.g., CO2, nitrogen, nitrous oxide) - Most commonly used propellants: chlorofluorocarbons (CFCs), are not PROHIBITED (Dichlorodifluoromethane, dichlorotetrafluoroethane, trichloromonofluoromethane) - Hydrocarbons are used instead: Blends of butane, propane, isobutane, compressed air, nitrogen, nitrous oxide It’sprohibited because CFC released to air can reduceozone in air, if excessive amount of CFC, then it increase UV radiation in theenvironment |
|
|
Case Study: What is a vapor pressure of a 60:40 mixture of propane and isobutane. Information as follows: - Propane: 44.1 (MW), -43.7°F (BP), 110psig (VP), 0.5g/mL (liquid density), -156°F (flash point) - Isobutane: 58.1 (MW), 10.9°F (BP), 30.4psig (VP), 0.56g/mL (liquid density), -117°F (flash point) How to determine the vapor pressure of this mixture? |
Assume an ideal solution: For Raoult's law, we need to determine number of moles of each propellant npropane=60/44.1 = 1.36 nisobutane =40/58.1 = 0.69 -From Raoult’s law, the partial pressure exerted by the propane is: Ppropane = npropane/(npropane + nisobutane) * Ppropane 1.36/ (1.36+0.69) * 110 = 72.98 psi partial pressure propane Ppropane = nisobutane/(npropane + nisobutane) * Pisobutane 0.69/(1.36+0.69) * 30.4 =10.23 psi partial pressure isobutane Total vapor pressure = 72.98 + 10.23 = 83.21 psi |
|
|
Aerosol ressurized Containers: Glass |
- Good chemical compatibility - Poor pressure resistance |
|
|
Aerosol Pressurized Containers: Metal |
- Tin plated steel, aluminum, stainless steel - Special coatings can be used |
|
|
T/F: Tin plated steel is usually used for smallvolume aerosols. |
FALSE - Tin plated steel used for larger aerosols. Stainless steel used for small volume aerosols |
|
|
Aerosol Pressurized Containers: Plastics |
- Permeable to vapor inside of container - Drug-plastic interactions |
|
|
Aerosol Valve Assembly: |
- Function of valve assembly is to permit expulsion of contents of can in the desired form, at desired rate, and in case of metered valves, in proper amount of dose - Among materials used in the manufacture of various valve parts are plastic, rubber, aluminum, and stainless steel |
|
|
Aerosol Parts |
1. Actuator: Button that user presses to activate the valve assembly for emission ofthe product 2. Housing: Prevent leakage of the formulation when valve is in closed position. 3. Gasket: the link between the dip tube and the stem and actuator 4. Mounting cup: Hold the valve in place 5. Dip Tube: Bring the formulation from the container to the valve 6. Spring: Mechanism by which the actuator retracts when pressure is released, thereby returning the valve to the closed position 7. Stem: Supports the actuator and delivers formulation in proper form to the chamber of the actuator |
|
|
Aerosol Container and Valve |
- Formulation must NOT react with container or valve components - Container and valve must be capable of handling pressure - Must resist corrosion - Valve must contribute to the form of product emitted |
|
|
Working Principles of Aerosols: Pressured Metered Dose Inhalers (pMDIs) |
- Allow administration of metered doses - Drug is dispersed in propellants and device facilities aerosolization of drug - Metered dose inhaler consists of three major components: Container/canister, metering valve, & spray actuator |
|
|
Drug Status in Aerosol Systems: Drugs may be dissolved in propellant system |
- Smaller spray particle size can be achieved after complete propellant evaporation - Simplified manufacturing process - Drug must be soluble - Chemical degradation may occur faster |
|
|
Drug Status in Aerosol Systems: Drug may be suspended or emulsified (dispersed) in propellant system |
- Can be used to deliver insoluble drugs - Higher doses can be delivered - Constant agitation during manufacture and use is required - Physical instability might be a problem |
|
|
T/F: If the drugs are suspended or emulsified in thepropellant system, agitation during manufacture and use is required. |
TRUE |
|
|
Aerosol Quality Assurance |
- Container is tested under various environmental conditions for leaks or weaknesses in valve assembly or container - Valve discharge rate: Determined by discharging a portion of previously weighed aerosol during a fixed period and calculating the difference in weight. Expressed as grams of contents discharged per unit time (g/min) - Aerosols may also be tested for spray patterns, particle size distribution, accuracy and reproducibility of dosing |
|
|
T/F: Valve discharge rate of an aerosol is the amount of the drug discharged per unit volume |
FALSE - It's amount go drug discharged per unit TIME |
|
|
Aerosol Packaging, Labeling and Storage |
- Packaged as part of manufacturing process - Protective cap or cover should fit snugly over valve - Medicinal aerosols are labeled by manufacturer with peel-away labels that can be replaced by pharmacist - Auxilary labels |
|
|
Aerosol Packaging, Labeling and Storage: Auxilary labels |
- Do not puncture container - Do not use or store near heat or an open flame - Store at 15 - 30°C - Shake before use - Hold at specific angle or distance |
|
|
Aerosol Patient Counseling |
- Patients should be advised about importance of coordination between pMDI actuation and breathing - Breath holding for 10 seconds - Shake container well before use - Wait for ~1min between actuations if multiple dosing is recommended Wait~ 1 min: Actuator needs to reset so dose can be accurate, particles we inhaled in the first inhalation need time to deposit in pt’s lung |
|
|
Nebulizers |
- Transform solutions or suspensions containing drugs into aerosols that can be taken by inspiration - Available as unit doses or concentrated solutions for administration after dilution - Classified as: ==> Air-Jet Nebulizers: High Velocity Airstream Dispension ==> Ultrasonic Nebulizers: Ultrasonic Energy Dispersion |
|
|
Air-Jet Nebulizers |
- Pressured jet air stream delivered by compressor forced through Venturi - Venturi effect: Fluid speed increases - Jet stream strikes the rising liquid and breaks up into droplets of varying sizes - Air stream pushed droplets out of nebulizer as a cloud |
|
|
Ultrasonic Nebulizers |
- Piezo-electric crystals produce high frequency sound waves in the nebulizer solution - High frequency vibration is sufficient to produce a vapor miss - Advantage: Lighter and quieter than air-jet nebulizer |
|
|
Disadvantages of Older Nebulizers |
- Aerosol is produced at a constant rate - Air-Jet: Crystallization of drug may occur due to evaporation of solvent - Ultrasonic: Cannot nebulize high-viscosity liquids. Increase in temperature causes degradation of thermo-sensitive drugs |
|
|
Nebulizer Patient Counseling |
- Nebulizers should be kept upright - Breath slowly and deeply and hold breath for up to a few seconds - No mixing any other medications with prescribed medication for nebulization |
|
|
Dry Powder Inhalers |
- Solid drug suspended in dry powder mix that can be fluidized when patient inhales - Dry powder aerosol is dispersed from static powder bed. Aerosol is generated by moving the particles from the powder bed - Particles can be moved from formulation by two mechanisms: ==> Passive Inhalers: Pts active and inhale ==> Active Inhalers: Power assisted, use pneumatic impact and vibratory force |
|
|
Dry Powder Inhalers Patient Counseling |
- More patient friendly and require less coordination between patient breathing and drug inhalation - Device must be kept parallel to ground to keep powder aerosolized - Pt must be careful while puncturing blister - Breathe in deeply and steadily - Pts should be cautious about exposing DPI to humid environment |
|
|
Solid Dosage Forms |
- Hard gelatin capsule, soft gelatin capsules, powders, etc.. - Can we make any therapeutic agent in any solid dosage form? No, there are limitations to each therapeutic agent. - What is an important property in solid dosage form? Compressibility (if poor, then we consider making capsule – we have powder inside capsule and we don’t have to compress into tablet dosage form). - There is NOT a single dosage form we can make without using excipients. But the wrong excipient or in the wrong amount, may damage the final product. - Suspension: therapeutic agent + viscosity enhancing agent (as inactive ingredient). - Each excipient is used for specific purpose. Ex. Tablet needs compressibility – powder must be compressible, so powder must contain good flow. - Evaluation tests: applies to all dosage form final products (assures pt, physicians, etc, that pt will receive the dose they’re supposed to take). - Weight variation: weigh capsule and find mean weight of capsule – difference between all tablets - variation should be minimum - Remember**: The higher the surface area, the faster the drug dissolution Dissolution equation: Noyes-Whitney Most important property in formulating suspensions: Equilibrium solubility Striking difference between 1st and Zero order: K |
|
|
Solid Dosage forms include: |
- Powder - Capsule - Tablet - Controlled released of modified released CR and IR are not interchangeable because the technology to make CR is different than IR tablets (Why are they not interchangeable if dose is the same? If one is XL and one is SR – absorption characteristics are different so they’re not interchangeable). |
|
|
Powder Properties Include |
While discussing all solid dosage forms, it's important to recognize that all powder properties, intrinsic and derived, play an important role in influencing the performance of the finished product - Size and size distribution - Particle size - True and bulk apparent density - Surface area and specific area **Know these properties – know units (tortuosity, porosity have NO unit). - Size and size distribution: particle size of therapeutic agent and particle size of inactive ingredients used - It’s ideal that these particle sizes are very close in size to each other. Always expressed by using average size of powder particles (because they’re all different so we use the range, the mean). Size distribution influences content uniformity of drug. We want AI to be present in same amount in each capsule or tablet that we make. Particle shape: Powders have different, irregular shape (The smaller the particle size, the more irregular the shape, the least they will flow uniformly) True and bulk density: True density is intrinsic property (doesn’t change no matter what the particle size is). Bulk density can change depending on particle size (derived property). If density of AI and excipients are too different, then these particles may not mix well and will not become homogenous uniform mixture. We want a homogenous distribution of the therapeutic agent with excipients – that’s why density is so important. Surface are is related to particle size: The smaller the particle size, the larger the surface area (Specific surface: Surface area/gram of powder), the larger the specific surface. We want small particle size to help with dissolution but sometimes we create different problems. |
|
|
Additional Powder Properties Include |
- Porosity, angle of repose, and flow - Adsorption, wetting phenomenon, contact angle, hygroscopicity, and deliquescence - Equilibrium solubility of drug and its dissolution Porosity: void space present in powder material (influenced by particle size – smaller particle size, higher porosity (more irregular the particle size)). If porosity is too high, tablets may split in middle upon storage (Will influence content uniformity). Angle of repose: determines flow of powder material (if angle of repose is high, then flow is not good) – influenced by particle size (we need an inactive ingredient to aid with flow). Adsorption: surface phenomenon in surface of powder materials (Kaolin is strong adsorbing agent) Wetting: surfactant promotes wetting by reducing contact angle, if contact angle is reduced the wetting increases and the particle dissolution is better (Ex. Span & Tween are wetting agents –hydrophobic material + base). If we don’t use wetting agent, the AI will stay on top layer of aqueous layer. We want AI to be dispersed through the aqueous layer. Used in very hydrophobic drug dosage forms. Hygroscopicity: AI adsorbs moisture from atmosphere – we reduce hygroscopicity by adding desiccator into final container of drug dosage forms (Desiccator adsorbs moisture & keeps it from adsorbing it from drug). If drug adsorbs moisture (#1 cause of chemical degradation is hydrolysis, which is promoted by water), it’s likely to degrade much faster. Deliquescence: material is so hygroscopic, that small amount of moisture turn powder into liquid. |
|
|
Powder Dosage Form Use |
- Powders represent one of the oldest dosage forms. - Recently, due to declining use of crude drugs and increasing use of highly potent compounds, powders have been replaced by tablets and capsules. - Powder, as dosage form, still represents a very small portion of all solid dosage forms Powder has been replaced largely by capsules and tablets (due to fancy equipment to make tablets, and less use of crude drugs). |
|
|
Advantages of Powder as Dosage Form |
- Offers flexibility in compounding - Relatively good chemical stability (Generally, drugs are more stable in solid dosage forms than in solution form) - Due to small particle size (i.e., greater specific surface), powders promote rapid dissolution compared to compressed solid dosage form such as tablet Flexibility: We can make powder into any particular strength, then adjust the dosing given to patients (unlike tablets which are made into one strength per tablet) Powders have better stability than liquid dosage forms (ex. Solution, emulsions, etc.) because use aqueous medium in liquids and the number one cause of degradation is hydrolysis. If we keep drug away from water, it’s likely to stay stable for longer period of time.Preservatives in liquids may lose its quality over time, so it’s safer to take solid rather than liquid dosage form after expiration date). Dissolution is influenced by particle size (equation Noyes-Whitney) **Review equation. Higher the surface area, the smaller the particle size, the higher the dissolution of the AI. If dissolution begins, then absorption begins (if drug dissolves rapidly, then it will reach general circulation rapidly – peak time will be short, onset of action will be quicker) |
|
|
Disadvantages of Powder as Dosage Form |
- Time consuming to prepare - Not a good dosage form for dispensing many unpleasant tasting, hygroscopic, and deliquescent drugs Hygroscopic AI: will adsorb moisture. Unpleasant taste AI: if it’s bad taste,patient won’t want to take it. |
|
|
Powders Fall Into Two Categories: |
1. Divided powders 2. Bulk powders Divided powders: individual dose is wrapped into individual paper. Bulk powder: Container with large quantity of AI. |
|
|
Divided Powders |
Refers to single dose of powder drug mixtures individually enclosed in paper, cellophane or metallic foil wrappers or packets Ex. Goody's Headache Powder |
|
|
Bulk Powders |
Refers to powders intended to be administered in quantities which are safe for patient to measure |
|
|
Bulk Powders Frequently Used as: |
- Dusting powders (talc powder) - Antacid products - Laxatives (Metamucil and others) - Dietary nutrient supplements (powder fiber type products intended to be administered in large dosage) - Dentifrice (dental powders) Particle size becomes important for bulkpowders. Talc: adsorbs moisture. The smaller the particle size, the larger the surface area, the greater the adsorption of moisture. We minimize irritation to skin in topical dosage forms by reducing the particle size. Antacids neutralize excess of acid, this is influenced by particle size (small particle size neutralizes much faster than larger particles) Ex. Laxatives (Miralax, Golytely, Metamucil), Dusting Powders (Quinsana, Baby Bee, Nystop (fungal infections - topical use)) |
|
|
Powder Preparation Techniques |
In the manufacturing and extemporaneous preparation of powders, the general techniques of sifting and mixing will play an important role. In addition: - Use of geometric dilution technique for incorporation of small quantities of potent drugs - Reduction of particle size of all ingredients (drug and excipients) to approximately same range to prevent stratification of large and small particles - Sieving (i.e., passing powder mixture through sieves) - Necessary to achieve good mixing and reduction of agglomerates, especially in preparation of dusting powders into which liquids have been incorporated - Protection against humidity, air oxidation and loss of volatile ingredients Sifting: mixing powder material by using mortar and pestle, and pass through sifts to make uniform powder (The higher the sift, the finer the particle size. The lower the sift, the bigger the particle size). Geometric dilution: important when AI is present is in small quantity. So to mix properly we use geometric dilution to have a uniform mixture. Reduction of particle size: particles must be similar in size to prevent stratification of large and small particles (separation of large and small particles). We need to ensure mixing is done correctly to prevent agglomeration of powder materials. If AI is hygroscopic or if it's susceptible to oxidation, we need to minimize adsorption by incorporating protection to dosage form (ex. inactive ingredient and/or wrap dosage form into individual wrappers) |
|
|
Packaging of Divided Powders |
Specially manufactured papers and boxes are available for dispensing divided powders - Vegetable Parchment paper: thin semi-opaque moisture resistant paper - White bond paper: opaque paper with NO moisture resistant properties - Glassine paper: glazed, transparent moisture-resistant paper - Waxed paper: transparent water-proof paper Hygroscopic and volatile drugs can be protected best by used of waxed paper, double wrapped with bond paper to improve appearance. Moisture resistant paper: if AI issusceptible to moisture it’s likely to undergo degradation so we can use this paper to protect the dosage form. White bond paper: no moisture resistant properties, can be used to wrap after other types of paper to help with adsorption (shouldn’t be used alone – can be used to double wrap) |
|
|
Special Problems with Divided Powder Packaging |
Incorporation of the following into powder paper require special attention: - Volatile subtances - Eutectic mixtures - Liquids - Hygroscopic and deliquescent substances |
|
|
Eutectic Mixture |
- When solid compounds like phenol, camphor, menthol, salol, thymol, antipyrine, acetanilide, aspirin, and phenacetin are mixed at room temperature, formation of liquid occurs - This phenomenon of liquefaction of a powder in the presence of another powder, at room temperature, is described as eutectification, and is the results of lowering the MP of constituents of mixture by other drug When mixed together, these compounds form a liquid (only when together, they remain solid when separated) |
|
|
What causes liquefaction? |
- Presence of low intermolecular forces as reflected in low MP - Soft crystalline structure or ready sublimation probably will liquefy a chemical when mixed with chemical of similar structure. Obviously, it would be difficult to prepare a powder, capsule or tablet with a melt Low intermolecular forces: weak attractive forces - low MP, low BP |
|
|
How to handle eutectic compounds |
- Each compound should first be mixed with a portion of diluent (adsorbing agent) and then gently blended together. Generally, a ratio of 1:1 (adsorbing agent : eutectic compound) is sufficient to handle this problem - Another approach is deliberate forcing of formulation of liquid by direct trituration of two eutectic compounds, followed by adsorption of moist mass on diluent (adsorbing agent). Though this technique offers advantage of extended product protection, it requires use of more amount of diluent than first method Good adsorbing agents: Kaolin, talc (these compounds protects powders to adsorbing to each other). Deliberate forcing of forming liquid,then add Kaolin to reduce adsorption of powders. |
|
|
Adsorbing Agents |
Traditionally employed as inert protective agents include: - Kaolin - Mg2+ oxide & Mg2+ carbonate - Talc & silicic acid Kaolin is already available in a fine particle size. Magnesium oxide and magnesium carbonate need to sometimes be subjected to decreasing particle size before being able to use them as adsorbing agents. |
|
|
Bulk Powders: Classified as... |
- Oral products - Dusting powders - Oral powders These are generally supplied as fine powders or as effervescent granules. Effervescent granules are intended to be suspended or dissolved in water or juices or soft food prior to administration |
|
|
Effervescent Granules |
- Contain an AI, sodium bicarbonate, and either citric acid, tartaric acid and sodium biphosphate. - Upon mixing of effervescent granules with water, CO2 is liberated as a result of acid-base reaction - Effervescence is due to release of CO2, and serves to mask the taste of salty of bitter medications Specific ingredients we need to prepare effervescent granules: - Sodium bicarbonate: alkaline - Citric & tartaric acid: acidic The mixture of these ingredients will cause the effervescent properties to happen. Must have one alkaline, one acidic, and AI to prepare effervescent granules. When they’re mixed, we have to imply heat (we induce moisture to form acid-base reaction in presence of water) Ex. Alka-Seltzer, Zantac, Effydral |
|
|
Dusting Powders |
- Locally applied non-toxic preparation that are intended to have NO systemic action - Should always be dispensed in a very fine particle size (or large specific surface) to enhance effectiveness and minimize skin irritation - When necessary, may be micronized or pass through sieves of greater than 160 - 200 mesh - Applied to various parts of body as: anti fungal protective, adsorbent, antiseptic, antipruritic, & astringent -No systemic action, only local affect (AI doesn’t pass through skin into general circulation, it’s only for local affect). -The smaller the particle size, the lesser the skin irritation produced. Effectiveness is enhances by using smaller amount of drug (we want to use less drug if it works instead of more toreduce irritation) -Larger the mesh number, the smaller the particle size. Smaller mesh number, the larger the particle size. Ex. Quinsana Plus, Baby Bee, Nystop |
|
|
Capsule as Defines by U.S.P |
"Solid dosage form in which the drug is enclosed in either a hard or soft soluble container or shell of suitable form of gelatin" Hard gelatin: used to incorporate solid material (Capsule has 2 parts). Soft gelatin: used to incorporate liquid material (liquid is prepared by using non-aqueous material, such as oil) (Capsule has 1 part). Gelatin was originally used to prepare capsule dosage form, but there are more materials used to prepare capsule dosage form -No compressibility needed (powder material filled into hard gelatin capsule) -Coated beads can also be incorporated into hard gelatin capsules (ex. Prilosec, Nexium, Micro-K), these beads contain AI (CR dosage forms) |
|
|
Capsule Generalities |
- Popular dosage form - About 20% of products are available in this dosage form - Solid as well as liquid drugs can be administered through this dosage form |
|
|
Capsule Advantages |
- Easy to administer drugs with unpleasant taste or odor through practically tasteless shell - Since pharmacists can prepare capsules quickly and conveniently, a physician is able to vary dosage and combination of drugs to suit individual needs - Generally, availability of drugs from well-formulated capsule is better than tablet dosage form (though drugs have been reported to be better and poorer absorbed) - Gelatin shell (capsule) containing drug will rupture in gastric fluid in few minutes (<5min) and drug is available for dissolution immediately Some drugs only come in bulk because it's not worth making it into tablet (economical), so the bulk is sold and capsules can be made into a variety of doses within the pharmacy. Some studies say bioavailability is improved in tablet dosage form, some say it's better in capsule. But well formulated capsule, one would expect the bioavailability to be better in capsule than tablet because powder material does NOT need to disintegrate once administered (unlike tablets). Gelatin capsule shell ruptures: there's a hole in the capsule and drug will dissolve immediately |
|
|
Capsule Disadvantage |
- NOT recommended for administration of very soluble compounds such as KCl due to localized irritation and gastric distress If drug is highly soluble, then concentration of solution will be very large and it will cause gastric distress once administered. (ex. Potassium chloride: extremely soluble molecule) |
|
|
Capsule Capacity |
- Empty capsules are sold by sizes. For human use, 8 different sizes are available - Capacity of each size varies according to the combination of drugs and their true density and apparent or bulk density - Veterinary capsules are available in 10, 11, and 12 and their approximate capacities are 30, 15, and 7.5 grams The higher the numeral value, the smaller the capsule size (ex. 3 is smaller in size than 0) - Which capsule to use is determined by how much powder will be inserted into capsule. Each capsule has different capacity If you have a particular capsule size andyou know what the volume is for that capsule that, then find out how much drugyou can put there – this is determined by the true density (g/cc) of the drug (how heavy it is) -Two different drugs may have different true density which will influence how much of them can be put into capsule -Capsule size is dependent on bulk density since it’s dependent on particle size |
|
|
Table of capacity of capsule sizes in terms of aspirin |
Cap size ----- Aspirin (mg) - 000 --------- 1000 -- 00 ----------- 600 --- 0 ----------- 550 --- 1 ----------- 330 --- 2 --------- 250 --- 3 --------- 200 --- 4 --------- 125 --- 5 --------- 60 The larger the number, the smaller the capacity |
|
|
Quantity of powder that fits in each capsule size depends of compounds' density |
Density is very important – true density is different for different drugs - So if different true density, then bulk volume will be different, and volume will be different – so cap size may be different for the same quantity of two drugs Volume for different capsule numbers are fixed, the only thing that changes is the amount of different materials it can hold - Variation occurs because true density of each powder is different - Particle size is also different, which will change bulk density and bulk volume Same weight material may have different size capsule because of true density difference, bulk density difference, bulk volume difference. |
|
|
Hard Gelatin Capsule Structure |
Cap of capsule + body of capsule (2 part) (Includes locking device to prevent premature opening) Commercially marketed capsules appear in all colors for product identification and to encapsulate ingredients that are unattractive through colorless capsules (ex. Pyridium) |
|
|
Capsule Figure |
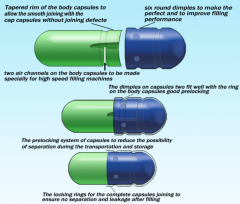
|
|
|
Examples of Hard Gelatin Capsule Products |
- Amoxicillin - Cephalexin - Tetracycline - Doxycycline - Temazepam - Omeprazole (modified release product) |
|
|
Hard Gelatin Capsule Composition |
Since hard gelatin capsules, most often, contain powdered drugs, the drug dissolution depends upon drug particle size, and excipients used in the formulation Particle size is important in hard gelatin capsules, and excipient used is also very important (We need the right excipient in the right amount to ensure that drug dissolution is proper) -Smaller particle size, larger surface area, large specific surface, the faster the drug dissolution |
|
|
Composition of Empty Capsules |
- Made of gelatin blends (principally) and may contain small amounts of certified dyes, opaqueing agents, plasticizers, and preservatives - Capsules have also been made with methylcellulose, polyvinyl alcohol and denatured gelatins to modify their solubility and produce enteric effects - Gelatin is obtained by irreversible hydrolytic extraction of treated animal collagen. Common sources of collagen include animal bones, hide portions, & frozen pork skin. They are prepared by using blends of gelatin obtained from bones and pork skin - Bone gelatin gives tough and firm film, but tends to be hazy and brittle. - Pork skin offers plasticity and clarity to blend Certified dye – all coloring agent contain FD&C number (means they’re approved for pharmaceutical use). We need preservatives because gelatin isobtained from animal source. Methylcellulose, polyvinyl alcohol: used when people can’t use animal source capsules for personal reasons. |
|
|
Storage of Capsules |
- Storage of empty gelatin capsules should be given special consideration. Capsules (as received from suppliers) have moisture contents of 12 to 15% and these levels should be maintained during storage - Exposure to extremely high or low humidity conditions for extended period cause capsules to gain or lose moisture - At high humidity, capsules absorb sufficient moisture and may soften and become tacky. - At low moisture level, capsules may become brittle and suffer dimensional changes. - Thus, handling gelatin capsules (during manufacturing & storage) should be carried out within relative humidity range of 30 to 45% Moisture content in gelatin capsule is critical to keep capsule intact. We don’t want trouble within 3-5 months after preparing dosage form. High moisture level: the capsule will gain moisture and soften (may degrade faster) Low moisture level: the capsule will lose moisture and become brittle |
|
|
Capsules: Product Identification |
- It's not unusual for pharmacist to be asked the identity of unknown capsule - The imprinting or branding of capsules by manufacturer with their name, initials, code number or symbol is now required like tablet dosage form and it facilitates identification Identification is not unique to capsule dosage forms. It also applies to tablets, soft and hard gelatin capsules. It facilitates identifying strengths by manufacturer (color and number) |
|
|
Manufactures of capsules are required to perform the following tests to assure the patient received required dose of drug: |
- Drug content uniformity (smaller Std. Dev.) - Weight variation (minimum variation) - Drug dissolution (% of drug dissolved against time) Drug content uniformity: we want to make sure when pt takes capsule or dosage form, every capsule will capsule said amount of AI. In order to find out such strength, they analyze the content in every capsule and find out how much AI present in all capsules. Weight variation: weigh capsules and make sure all capsules have similar weight with minimum variation – the smaller the standard deviation, the greater the uniformity of that particular strength Drug dissolution: whenever we have suspension (powder dispersed), powder must be dissolved – same with powder, tablets, and hard gelatin capsule – plot graph: % dissolved vs. time - At time zero: no drug is dissolved - As the time increases, the amount of drug dissolved should increase - At time t, almost all drug is dissolved in fluid - If drug dissolves fast, then it reaches the general circulation quickly and starts causing therapeutic affect |
|
|
Example of Hard Gelatin Capsule Formulation |
1. AI (250mg) 2. Lactose (143mg) 3. Sodium Starch Glycollate (25mg) 4. Mg Stearate (2mg) Package insert will give you list of AI (API – active pharmaceutical ingredient) and inactive ingredients present in a particular dosage form. Excipients have different functions when present in dosage forms. Sometimes we have greater amount of inactive ingredient when compared to AI, and they're all necessary for their function with the specific powder material. |
|
|
Soft Gelatin Capsule Uses |
Because of their special properties and advantages, they're used in a variety of industries, manly pharmaceuticals. In the closely related cosmetic industry, they may be used for breath freshener, perfumes, bath oils, bubble baths, shampoos, suntan oils, and skin creams. To keep capsule intact, must have non-aqueous liquid inside capsule (not water soluble) |
|
|
Soft Gelatin Capsule Structure
|
Gelatin outside, and drug with fill liquid inside (oily, semisolid, or viscous liquid) Liquid medication goes into apparatus, gelatin ribbon encapsulates AI, and soft gelatin capsule containing therapeutic agents is made. ONE PART CAPSULE (liquid contains AI). |
|
|
Soft Gelatin Capsule: Pharmaceutical Application
|
Essentially they are solid dosage forms containing liquid medication, thus the advantages are: - Permit liquid medication to become easily portable - Accuracy and uniformity of dosage form from capsule to capsule and lot to lot variation - Bioavailability is often improved since they contain drug in solution or suspension form (disintegration and dissolution steps are eliminated) Solid and hard gelatin capsules are still considered solid dosage forms. Not a lot of variation - smaller standard deviation, higher uniformity. Bioavailability is improved because AI is present in liquid dosage form, so it reaches general circulation immediately upon administration (it's already available in molecular form in liquid) |
|
|
Commercially available soft gelatin capsule product examples |
- Amitiza - Benzonanate (100 - 200mg) - Lovaza - Starzor (Valproic acid) - Mi-Omega, N.F - Nifedipine (Procardia) - Prometrium (Peanut Oil) - Do not use if allergic to peanuts. Peanut oil is used to dissolve AI - Terazosine - Ritonavir (Norvir) - Ritonavir initially came out as hard-gelatin capsule, then they experience polymorphism and dissolution problem and they took it off the market – then prepared it as solution dosage form, but patient didn’t like the taste – then they change to soft-gelatin capsule (it was recommended to store in refrigerator) – and now it’s available in tablet dosage form - Vitamin D capsules - Colace (Docusate Sodium) |
|
|
Capsule vs. Tablet: Plasma concentration vs. Time |
Peak plasma concentration and AUC were NOT significantly different from tablet compared to capsule Rate of absorption: Cpmax and Tmax Extent of absorption (relative amount): AUC Bioavailability from tablet and capsule dosage form formulations are compatible, since Cpmax, Tmax, and AUC are not significantly different. |
|
|
Example of Soft Gelatin Capsule Formulation |
- PEG 400 (337mg) - Tween 80 (195mg) - Oleic acid (80mg) - HPMC (74mg) - DMAE (34mg) - Propyl gallate (2mg) |
|
|
Tablets |
- USP and NF describe tablet as solid dosage form containing medicinal substances with or without suitable diluents - Are available in many sizes, shapes, and colors - Are available as uncoated, coated, and scored tablets It's impossible to make a tablet without excipients. If something goes wrong in 4-5 steps involved in making tablet dosage form, the consequence is shown in the quality of the final product – it affects the bioavailability of the drug. Tablets are likely to contain more inactive ingredients than other types of dosage forms (followed by CR dosage forms). Why are some tablets scored? Because it's easier to break/cut tablets (sometimes physician writes Rx for 1/2 tablet so scoring becomes important) |
|
|
Advantages of Tablets as Dosage Forms |
- Ease of administering accurate dose of drug - Portability and compactness - Physical chemical stability of drugs - Economy in manufacturing For these reasons, tablet is a very popular dosage form. Drugs are more stable in solid dosage form than in liquid dosage form, because there’s less moisture there than in liquid dosage form (the number one property that degrades drugs is hydrolysis). |
|
|
Disadvantages of Tablets as Dosage Forms |
- Difficulty in swallowing tablets (infants & elderly)
- Developing optimum formulation is quire challenging, particularly for hydrophobic drugs This is attributed to the fact that the AI, which is a powder, may not always possess desired powder properties (i.e. flow, angle of repose, bulk density, true density, cohesiveness, compressibility, and particle size and shape). Imparting compressibility, cohesiveness, and uniform flow require incorporation of inactive ingredients (excipients) in the formulation. Hydrophobic drugs are problematic drugs,and sometimes it’s hard to maintain optimum formulation. -The higher the contact angle, the more hydrophobic the drug is, the more excipient we will need to prepare that formulation and maintain an optimum formulation. If powder does not possess cohesiveness, it’s not easy to make tablet dosage form. Powder must possess a certain degree of compressibility in order to be made into a tablet dosage form (this is not an issue for capsule dosage forms) – we measure compressibility by Hausner and Carr’s index. Content uniformity, drug dissolution, weight variation, hardness are all dependent on these powder properties. Every therapeutic agent possess different chemical properties, so inactive ingredients incorporated into each dosage form will be different and the amount needed for these inactive ingredients will also be different. |
|
|
Important Steps in Tablet Manufacturing |
Failure to follow proper techniques and use of right excipients in right amount leads to adverse effects on the quality of finished product 1. Mixing of solid ingredients of formulation. This will include AIs, and some excipients such as diluent and part of disintegrating agent (Principles of solid-solid mixing) 2. Mixing of a liquid, when applicable, and preparation of wet powder mass or mixture. Addition of binding agent (solution form), coloring agent, if required followed by thorough mixing of all components (Principles of solid-liquid mixing) 3. Passing moist powder mass through a sieve (#10, 20 or 30) and prepare wet granules 4. Drying of moist granules (Heat) 5. Mixing of dried granules with other excipient (lubricants and portion of disintegrating agent) (Principles of solid-solid mixing) 5. Compression of granules into tablet of suitable size and shape by employing tablet press 6. Ejection of tablet from tablet die Each batch of a product, generally, consists of 100,000 to million tablets. Thus, powders (drugs and excipients) used in making a lot, weigh in kg quantities Failure to follow proper techniques will result in failure of certain tests of the final product. Diluentis added in the first step with the AI and disintegrating agent.Toget optimum mixing, we need to calculate how much time do we need to getoptimum mixing of this powder mixture (we cannot mix for too long or not longenough). Moist powdered mixture is important. 3rdstep: Granule is powder material that is in individual unit: moist material –identical composition of AI and inactive ingredient. 4thstep: we heat these granules to dry material (caution with heat sensitivematerials) . 5thstep: Dried granules are mixed with other inactive ingredients (Lubricant isvery important in tablets, it’s used to improve flow of powder mixture) &disintegrating agent. Disintegrating agent may be incorporatedin the first and last step. If any errors occurs during these steps,then the bioavailability of drug will be affected on the final product. Homogeneity is desired and seen when final tablet product possesses uniformity. The smaller the particle size, the more irregular the particles, the harder it will be for them to flow (angle of repose is measured). If flow is not ideal, we add lubricant to dosage form. |
|
|
Apparatus Used in Tablet Manufacturing |
- Cone blender use for mixing powder granules Anything that goes wrong in the first few steps will cause a problem in the bioavailability of the final product of the drug.- If the procedure says “mix for 20 min”, that’s the standard operating procedure –from that mixture, they will collect the powder samples from 5-6 different are as of the mixer and they will analyze these samples to determine how much AI in present in each sample (if the samples contains AI within the same range,this will be reflected in the quality of the final product). - Vertical mixer - V-shaped blender |
|
|
Tablet Press |
- Granules in hopper: Powder flow, granule size, porosity, and density - Punches and Dies: Compressibility, lubrication and tablet ejection If density is too different, then it will create separation of the granules. If porosity is too different, then air will repress powder material and there won’t be enough AI on each tablet & if there’s too much air inside the tablet it will split the tablet open - If tablet has high porosity, it means the powder material will be replaced with air, which will influence the uniformity and quality of the final product. If doesn’t possess compressibility, then it can’t be made into tablet dosage form. Often, binding agents require preservatives and if you don’t add enough preservatives then microbial growth can occur in finished product. Granules flow through hopper, and into the punches and dies – during this step, there’s continuous monitoring to see if mixture is sufficiently uniform. When the powder floes and goes through punches and dies, it will flow and punch will compress tablet, and tablet comes out on other side. 1. Granule properties (inserted) 2. Granule compression 3. Compressed tablet 4. Tablet ejection |
|
|
Tablet Classification |
Based on method of manufacture and intended use What is the intended use of the particular product? In most cases we use tablet-compressed dosage form (But we can also have SL dosage forms, chewable tablets, etc.) – The difference between these forms lies in the inactive ingredients used to accommodate different characteristics needed for each dosage form - Nature of inactive ingredient could be quite different between these dosage forms(different inactive ingredients for different physiological conditions targeted) For all dosage forms: Just because of a particular drug is suitable for a particular dosage form, it doesn’t mean we put this drug in every available dosage form – there must be certain physical chemical properties present in order to incorporate the particular drug into dosage form- If a drug is too soluble, we can’t make it into suspension dosage form. |
|
|
Tablet Classification: Tablets Delivered into GI tract - Compressed |
- Compressed - normal step in compounds - Multiple Compressed - more than one layer (one layer of drug, another layer of another drug) compressed multiple times - Enteric Coated- specific type of coating material used which makes tablet sensitive to pH, it does not dissolve in gastric fluid but will dissolve in intestinal pH (protects AI against stomach pH - dissolves at higher pH, not lower pH) - Sugar Coated - AI taste is improved by addition of sugar coating, also labor intensive process & expensive - Film Coated - similar principle to sugar coating, but we apply thin film of polymeric material which protects solid material in dosage form from unpleasant taste - Effervescent - effervescent powder compressed in tablet - Chewable - designed for children, inactive ingredient is different from regular compressed tablet - must be sweet/flavoring agent - Sustained-Action (modified release) |
|
|
Tablet Classification: Tablets Used in Oral Cavity |
- Buccal & Sublingual - Lozenges & Troches SL: disintegrate very rapidly due to special inactive ingredients |
|
|
Tablet Classification: Tablets of Other Uses |
- Vaginal - Implantation - Diagnostic |
|
|
Conventional Compressed Tablets
|
Prepared by a single compression of powder mixture. - Ex. Aspirin, alprazolam, Ambien, metoprolol, Diovan, ibuprofen, Tylenol |
|
|
Multiple Compressed Tablets |
Aka: Layered tablet Compressed tablets that are prepared by subjection to more than a single compressed cycle. Thus, there are two or more layers. - Ex. Meclizine, Allegra D Advantage: There may be a possible interaction between the two chemicals that is avoided by this method |
|
|
Enteric Coated Tablets |
Compressed tablets that are covered with coating, which resist drug dissolution in stomach but dissolves the drug in intestinal tract - Ex. Ecotrin or enteric coated aspirin pH sensitive (does NOT dissolve in stomach, & dissolves in intestine) |
|
|
Sugar Coated Tablets |
Compressed tablets that are coated with several successive thin layers of colored or colorless sucrose solution |
|
|
Film Coated Tablets
|
Compressed tablets coated with colored or colorless thin film of water soluble polymeric material which disintegrated rapidly in GI tract - Ex. Biaxin and Erythromycin |
|
|
Effervescent Tablets |
Compressed tablets which effervesces when in contact with water and liberate drug - Ex. Alka-seltzer Effervescent tablet must contain alkaline and acid material with AI, so it can cause effervescent effect as soon as it comes in contact with water |
|
|
Chewable Tablets |
Compressed tablets designed to be chewed before swallowing - Ex. Amoxicillin, Augmentin, Singulair Needs diluent: usually sweet tasting material |
|
|
Sustained Action Tablets |
Tablets provide initial sufficient amount of drug to cause a rapid onset of desired therapeutic response and an additional amount that maintains the response at the initial level for a longer period than obtained after administration of conventional single dose of that drug 2 portions: 1 portion is available as immediate release which causes effect right away, after a certain amount of time the 2nd portion of the formulation will come into effect |
|
|
Buccal & Sublingual Tablets |
Compressed tablets, usually flat or oval in shape, intended to provide systemic action by being placed in buccal pouch between cheek and gum or beneath the tongue - Ex. Nitroglycerin, Levsin Rapid dissolution, drug is available very quickly in general circulation |
|
|
Lozenges & Troaches |
Disk shaped solid dosage form made of therapeutic and flavoring agents intended for slow dissolution in mouth for continuous local application of drug to mucous membrane of oral cavity |
|
|
Vaginal Tablets
|
Ovoid or pear shaped conventional compressed tablets intended for insertion into vagina. They usually contain antiseptics, astringent, steroid and anti-fungal agents. They are usually inserted by means of plastic tube inserter |
|
|
Compressed Tablet Composition |
Comprised of two basic groups of ingredients: - Therapeutic agent (AI) - Excipients (aka additives) |
|
|
Excipients |
Classified into two groups according to the part they play in the finished product We have different types of excipients: binding agent, disintegrating agent, coloring agent – chemicals which do not exert any pharmacological action. Only AI exerts pharmacological action. The excipient used depends on the particular purpose the AI needs (ex. Lubricants: oil – decreases wear and tear) |
|
|
Excipients: Group 1 |
- Diluents - Binders - Lubricants The excipients impart satisfactory compression and flow properties to tablet formulation Group 1: likely present in every dosage form.When we make tablets, flow must be uniform and consistent (will show on final product quality). |
|
|
Excipients: Group 2 |
- Disintegrating agent - Coloring agent - Flavoring agent - Sweetening agent - Surface active agent These excipients help to lend additional desirable physical characteristics to finished tablets Group 2: these excipients may not be present in every formulation (ex. Coloring agent may not be present in a particular tablet dosage form). Surface active agent reduces contact angle when the drug is very hydrophobic |
|
|
Criteria for Each Excipient |
- Compatibility with AI - Physically stable - Should be physiologically inert - Low cost and good tablet properties When we make any dosage form, other than AI, any other ingredient should be pharmacologically inert, and must be compatible with AI (no interaction at all with AI) (there’s a possibility of chemical reaction between AI and excipient which may lead to discoloration of powder, and degradation) |
|
|
Tablets: Diluent or Fillers |
Diluents are added to formulation to increase bulk of tablet to a practical and convenient size. This is important for low dose drugs. They are essential to produce tablet of reasonable size. - Ex. Digoxin, levothyroxine, Captopril When therapeutic agent has very low dose,we cannot compress such dose into a tablet, so to do that we have to add a diluent or filler. |
|
|
Commonly Used Diluents
|
- Lactose - Spray dried lactose - Microcrystalline cellulose - Mannitol - Dry starch (must be dry!!) - Powdered sugar Diluents such as mannitol, lactose, sorbitol, sucrose are commonly used in chewable tablets |
|
|
Tablets: Binders or Binding Agents |
Incorporated in the formulation to impart cohesive property to powder mixture (granules) Cohesiveness ensures that tablet will remain intact after compression and until pt takes it |
|
|
Commonly Used Binders |
- Dry acacia or acacia mucilage (2 - 5% aqueous solution) - Dry tragacanth or tragacanth mucilage (1 - 3% aqueous solution) - Warm gelatin solution (1 - 4%) Generally, these agents are more effective when used as mucilage, compared to dry powder and require presence of preservative - Starch paste (5 - 10%): Effective (one of the best) as binding agent only in paste form - PVP (Polyvinul Pyrrolidone) (3 - 5% aqueous or alcoholic solution) Starch paste: used as effective binding agent (we also use starch in powder form, but we use only paste for binding purposes – forms viscous product) – starch powder is NOT effective binding agent. PVP alcoholic solution is used when powder is sensitive to moisture (soluble in water and alcohol) as binding agent -The previous ones were only soluble in water. We are given ranges (not specific values) |
|
|
Additional Binding Agents |
Cellulose derivatives - Methyl cellulose (1 - 4% aqueous solution) - Ethyl cellulose (Insoluble in water) (0.5 - 2% alcoholic solution) - Hydroxypropyl methyl cellulose (1 - 4% - soluble in water, alcohol, chloroform, and methylene chloride) Methylcellulose: suspending agent in suspensions, and can be used as binding agent in tablets A lot of excipients can be used for multiple purposes depending on the particular dosage forms. |
|
|
Lubricant Advantages |
- Improve flow of granules - Reduce adhesion of powder material (granules) to punches and dies during compression - Easy release of compressed tablet from mold or die - Act between surfaces in relative motions to prevent friction and wear - Help granules slip and slide to form compact in the die wall of a tablet press - Inadequate lubricant is evident by screeching sound and scratch marks on edge of tablet They are subdivided into three categories according to function |
|
|
Glidants |
- Material that improve flow characteristics of granules - Act by reducing inter-particulate friction - When used in right amount, they serve to assure smooth and uniform flow of granules |
|
|
Anti-adherents |
- Function to prevent tablet granules from sticking to faces of punches and die wall Most lubricants possess more than one of 3 attributes described. Usually, it may be necessary to employ combination of two lubricants in a formulation. Flow is important when we look at hard gelatin capsules, as well as tablets. It’s not uncommon to see a glidant and a lubricant in hard gelatin capsules (does not apply in soft gelatin capsules). |
|
|
Commonly Used Lubricants |
- Magnesium stearate (<1% w/w): Excellent lubricant but poor anti-adherent or glidant. If used in >1% concentration, it may retard drug dissolution - Corn Starch: (5 - 10%) Excellent glidant and anti-adherent but poor lurbricant - Talc (1 - 5%): Poor lubricant but excellent anti-adherent, & reasonably good glidant - Stearic acid (1 - 5%): Good lubricant. Poor anti-adherent and glidant - Water soluble lubricants: Carbowax 4000 & 8000, & sodium lauryl sulfate (1 - 5%) |
|
|
Excellent lubricant, but poor anti-adherent or glidant |
- Magnesium stearate - Stearic acid |
|
|
Poor lubricant, but good anti-adherent or glidant |
- Corn Starch - Talc |
|
|
Lubricant Generalities |
- Whether water soluble or insoluble, should be of very fine particle size - Function by forming a thin film around granules, their effectiveness is related to particle size and specific surface Powder particle with high specific surface = very fine powder particle - Smaller particle size, the lesser amount is needed for lubricant effect. Lubricant forms a thin film around tablet granules. The smaller the particle size, the lesser amount needed to form film. |
|
|
Disintegrant |
- Purpose: to facilitate tablet breakup following its administration - Rapid disintegration is LIKELY to result in rapid drug dissolution; though it's NOT an absolute guarantee Binding agent: binds cohesivess of powder material Disintegrant: will facilitate disintegrating of powder material (breaks tablet apart). Binding and disintegrating agentswork against each other (works exact opposite to each other – but we need bothof these agents). Rapid disintegration does always meanrapid dissolution. Dissolution is more important. But we should NOT assumethat if a tablet is breaking quickly that it will also dissolve quickly. |
|
|
Tablet Disintegration Process |
Aqueous fluid will enter tablet through capillary structure; swelling of disintegrating agent will build pressure inside the tablet Every tablet has certain degree of porosity present, and because of that there’s a porous structure there. Fluid in gastric and intestine will enter tablet – liquids penetrates tablets and comes into contact with disintegrating inactive ingredient (responsible ingredient that breaks tablet apart). Liquid swells tablet and builds pressure inside tablet, and disintegrates tablet. If tablet disintegrates to small granules, surface area will be higher, absorption will be likely higher (Smaller the particle size, the higher the disintegration and likely absorption) |
|
|
Dissolution vs. Disintegration |
Rapid and complete dissolution is more critical and vital than rapid disintegration alone for rapid and complete drug absorption (bioavailability) to occur. Complete absorption: high AUC (extend of absorption) - entire dose reaching general circulation & rapid dissolution (rate of absorption: Cpmax is high, Tmax is short) |
|
|
When to add disintegrating agent? |
May be added prior to granulation or during lubrication step prior to compression or at both steps - The effectiveness of many disintegrants is affected by their position (inter granular of extra-granular) within tablet |
|
|
Disintegrating agents: Inter-granular |
Presence of disintegrant inside granules |
|
|
Disintegrating agents: Extra-granular |
Presence of disintegrating agent between granules |
|
|
Commonly Used Disintegrants |
- Various starches: MOA is water uptake through pores of tablets due to capillary action, resulting in tablet expansion followed by disintegration - Primojel or Explotab: Low substituted carboxymethyl starch. Used in 1 - 8% (optimum 4%) concentration - Pre-gelatinized starch - Microcrystalline cellulose (Avicel) - Other disintegrants include alginates, cross-linked PVP, Veegum HV |
|
|
Colorants Advantages |
- Identifies different products - Identifies different strengths of same product (ex. Warfarin, levothyroxine, digoxin) - Minimize possible mix-up during manufacture - For aesthetic and/or marketing value The previous talked about excipients are present in all active agents. Now we look at excipients not used in every one dosage form (ex. colorant) |
|
|
Colorants Additional Info |
All colorants used in pharmaceuticals must be approved and certified by FDA. Any water soluble dyes, mixture of dyes and their corresponding lakes may be used as colorants for tablet manufacture. - Dyes are water-soluble - Lakes are formed by adsorption of water-soluble dye on hydrous oxide (Aluminum oxide) in insoluble form of dye Dyes and lakes are photosensitive and photosensitivity is affected by the drug, excipient and method of manufacture - Pastel shades generally show least amount of mottling (uneven distribution of color, yielding darker spots on tablet) - Yellow and green color (midrange of visible spectrum) will show less mottling compared to blue and red - Problems of mottling become more pronounced when concentration increases |
|
|
Migration of Colorant on Surface of Granules |
- Presence of excipients, which include colorant inside granule - Migration of colorant on surface of granules Each granule has identical composition: AI, diluent, liquid binding agent, and coloring agent. So moist powder material must be dried before compression. If colorant is not evenly distributed throughout formulation, migration and mottling occurs. |
|
|
Mottling Phenomenon |
- Uniform distribution of coloring agent - Spots of coloring agent (mottling) Related to concentration of dye, type of coloring agent, and slow vs. rapid drying of granules - Drying granules slowly at low temperature and with continuous stirring can reduce migration of color to surface and reduce mottling Even distribution of coloring agent, and all of a sudden a tablet will have a darker spot on top of the tablet (mottling phenomenon). This occurs depending on dying or drying of the tablets (uniform distribution of coloring agent in the formulation – does not mean product is bad, but psychologically the patient may think it’s not the correct product since the color is off). Dryinggranules becomes important. It should be dried slowly and with continuousstirring (Should not be dried fast with too increased of temperature), thisreduces migration of colorant to surface and reduces mottling phenomenon. Socolor is uniformly distributed on the granules and color is evenly distributed. |
|
|
Commonly Employed Colorants |
- FDC #40 - FDC #5 & #6 - FDC Blue #1 & 2 - FDC Green #3 Coloring agents are used in very small concentration (0.05 - 0.1%) |
|
|
Incorporation of Coloring Agents |
Generally mixed with binding agent solution (acacia, tragacanth or gelatin) and then mixed with other powder mixture - Much easier to incorporate coloring agent as solution than as powder (More effective in producing coloring effect in solution form than in powder form) - Thorough mixing of colorant is very critical to avoid problems of mottling Lakes, on other hand, are blended with dry excipients because of their insoluble nature |
|
|
Colorants Considerations |
If we use coloring agent is higher concentration sometimes produces opposite effect. All excipients we use in dosage forms, there is a critical concentration that should NOT be exceeded or negative (adverse) effects will appear in the dosage form. Plasma concentration vs. Time Graph: In the absence of coloring agent, the plasma concentration of drug at each time was higher if compared to the plasma concentration of the drug with coloring agent. - Coloring agent can form thin layer surrounding granules. If it’s very thin it’s ok, but if it’s thicker it may decrease dissolution |
|
|
Methods of Preparing Tablets |
- Wet granulation - Dry granulation - Direct compression |
|
|
Choice of Method of Preparing Tablets Depends Upon: |
- Powder properties (flow, size and size distribution, true and bulk density, hydrophobicity) - Dose of drug (small or large) - Available equipment - Practical and regulatory concerns When we prepare the granule, they’re wet. Dry granulation: no liquid at all,excipient used is specially processed Hydrophobic drug ALWAYS present problemwith dissolution, weighting, etc. Regulatory concern from FDA (will FDA approve this method?) |
|
|
Wet Granulation |
- Powdered drug is mixed with diluents, disintegrant, colorant, and binding agent (solution) - Wet powder mixture is passed through sieve (# mesh 20 or 40) and granules are prepared - Granules are dried, mixed with lubricant, and compressed into tablets The larger the mesh size, the smaller the particle size. Sieve number 60, 60 openings per square inch. If you have more opening in one square inch, it means the particle size is smaller. Granules are not so fine, so they pass through sieves 20 or 40. |
|
|
Advantages of Wet Granulation |
- Uniform drug distribution in granules makes it ideal method for low dose drugs - Provides good cohesiveness and compressibility to powder material due to addition of liquid binder - Minimum segregation of powders in mixture Digoxin weighs 100mg and AI is 0.125mg. AI is such a tiny amount so this method is an advantage. Minimum segregation: granules have identical composition, so there’s no way the powder can segregate from each other unless you have a dry granule (which is not in this case). If segregation isn’t there, then uniformity is much better so AI is more evenly distributed. Content uniformity is the most important test = same dose of drug each time patient takes the medication |
|
|
Disadvantages of Wet Granulation |
- Cost (greatest disadvantage) - Moisture sensitive drugs may require use of non-aqueous binder solution (PVP in alcohol) - Migration of water soluble dyes may cause unequal distribution of color - Heat sensitive drugs may be difficult to formulate Moisture sensitive drugs: use non-aqueous method |
|
|
Direct Compression |
In this method, the powder blend of AI and excipients is compressed into a tablet. Steps involved include: - Milling (reducing particle size) of drug and excipients to approximately same size - Mixing of drug and other excipients Reduce powder material (AI + inactive ingredient) and bring them to around the same size. If they’re not similar in size, the granules will segregate. |