Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
Function of the cerebellum
|
1. maintenance of posture & balance
2. Maintenance of muscle tone 3. Coordination of voluntary motor activity |
|
|
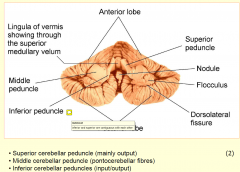
Superior Cerebellar Peduncle
|
- major OUTPUTS from cerebellum
- DENTATOTHALAMIC tract that terminates in the VL thalamus (decussation in the caudal midbrain tegmentum - ONE major afferent Ventral SptT |
|
|
Middle Cerebellar Peduncle
|
RECIEVES pontocerebellar fibres PROJECTS to neocerebellum
|
|
|
INFERIOR cerebellar peduncle
|
3 MAJOR afferents
1. DscT 2. Cuneocerebellar tract 3. Olivocerebellar tract (form contralateral inferior olivary nucleus) |
|
|
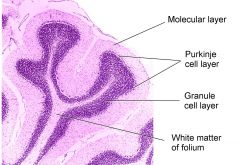
Cerebellar Cortex
|
3 layers
1. Molecular layer (stellate, basket cells & dendritic arbor of the purkinje cells) 2. Purkinje Cell layer lies between the 2 layers 3. Granule layer inner layer overlying the white matter (granule cells, golgi cells and cerebellar glomeruli) |
|
|
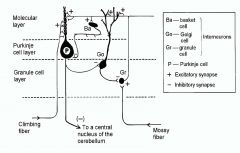
Neurons & Fibres of the cerebellum
|
1. purkinje cells: outputs from cerebellar cortex. inhibitory GABA to cerebellar & vestibular nuclei
2. Granule cells: glutamanergic excitatory cells 3. Parallel fibres; axons of granule cells that extend into the molecular layer 4. Mossy fibres are afferent excitatory fibres of the Spc, Pontocerebellar & vestibulocerebellar Tracts, terminating on granule cell, exciting them then dischargin through parallel fibres 5. Climbing fibres are afferent excitatory (ASP) from olivocerebellar tract |
|
|
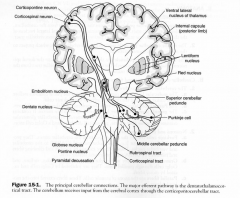
Major Cerebellar Pathway
|
1. Purkinje cells of the cerebellar cortex ptoject to cerebellar nuclei
2. Dentate Nucleus 3. VL thalamus to 1o motor cortex 4. Motor cortex as corticopontine tract to pontine nuclei 5. Pontine Nuclei project as pontocerebellar tract to contralateral cerebellar cortex where they terminate as mossy fibres completing the circuit |
|
|
Denate Nucleus
|
effector nucleus giving rise to DENTATOTHALAMIC tract
|
|
|
Principal Cerebellar Connections
|
|
|
|
Cerebellar Dysfunction;
Tirad |
(think alcoholic)
1. hypotonia (rag-doll appearance with pendular reflexes) 2. Dysequilibrium (loss of balance affecting gait and trunk dystaxia) 3. Dyssynergia (loss of coordinated muscle activity - dysmetria - intention tremor - failure to check movements - nystagmus (coarse and worse when looking towards side of the lesion) - dysdiadochokinesia - dysrhythmokinesia |
|
|
Anterior Vermis Syndrome
|
- involves leg region of anterior lobe
- atrophy of the rostral vermis most commonly due to Alcohol abuse - causes gait, trunk & leg dystaxia |
|
|
Posterior Vermis Syndrome
|
- flocculonodular lobe
- causes truncal dystaxia - due to brain tumours |
|
|
Hemispheric Syndrome
|
- one cerebellar hemisphere
- DUE to brain tumor or abscess (2o to otitis media or mastoiditis) - causes arm, leg, gait dystaxia & ipsilateral cerebellar signs |
|
|
Cerebellar Tumors
|
- 70% of brain tumor in children are found in the post. fossa
- 70% in adults are supratentorially 1. Astrocytomas (30% children) most often in cerebellar hemispheres 2. Medulloblastomas; (20%) and are malignant. believed to orginate from granular layer, and obstruct the CSF flow causing hydrocephalus 3. Ependymomas (15%) fq in 4th ventricle |
|
|
Cerebellum Blood Supply
|
Blood supply from posterior inferior and the anterior
inferior cerebellar arteries (PICA and AICA) and from the superior cerebellar artery (SCA, all vertebral artery system). |
|
|
Cerebellum Landmarks
|
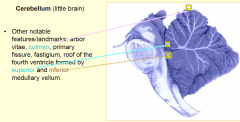
arbor vitae,
culmen, primary fissure, fastigium |
|
|
Cerebellum Anatomy
|
|
|
|
Peduncular surface
|
|
|
|
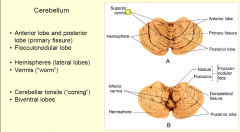
Lobes
|
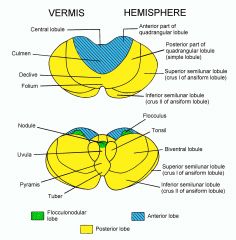
|
|
|
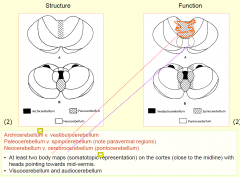
Structure and function
|
|
|
|
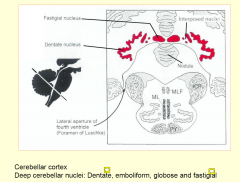
Deep Cerebellar Nuclei
|
|
|
|
Circuitry of cerebellum (simplified
|
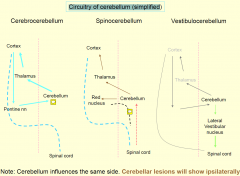
There is considerable amount of crossing in the case of vestibulocerebellum (e.g. uncinate fasciculus) meaning that vestibulocerebellar lesions are likely to produce bilateral deficits.
|
|
|
Molecular layers of Cerebellum
|
|
|
|
Mossy Fibres
|
• Mossy fibres (excitatory; +), bifurcate many times and form “rosettes”.
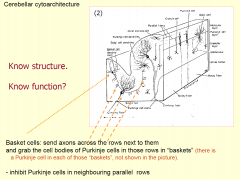
• Each rosette synapses with about 20 granule cells • Granule cells produce parallel fibres (excitatory; +) • Parallel fibres (PF) contact Purkinje cells (PC) and basket cells (BC, inhibitory) • Each PF fires the PC in its path and inhibits the PC in the path of the PF next to it: the most excited parallel fibre will win! • PF also contact Golgi cells which send inhibitory feedback to the rosette and cut off the signal • Result: sharpening of the signal in space and time (digitization?) -160,000 paralell fibres/ purkinje cell - * inhibitory to PC’s in the neighbouring rows, i.e. not quite as the picture shows. |
|
|
Cerebellar cytoarchitecture
|
|
|
|
Climbing Fibres
|
coming form the contralateral inferior olivary comples contact between 2/10PC
- each PC recieves only one CF - repeated firing of CF will slow down the activity of PC "long term depression" LTD cerebellar LEARNING? |
|
|
Only output form cerebellar cortex via
|
-PC
- GABAergic inhibitory cells |
|
|
Dentate; projection (Cerebrocerebellum)
|
contralateral VL n, then cortex
|
|
|
Globose, emboliform, fastigal (spinocerebellum)
|
to contralateral red nucleus and RF
|
|
|
Lateral vestibular (deiters)n (vestibulocerebellum
|
vestibulospinal tract and RF
|
|
|
PROPOSED MOA of cerebellum
|
• Removing “noise” from processed signals (“sharpening in time and space”)
• Comparing intended and executed movement (most likely including spinocerebellum). • Making the “right” signals long-lasting (“cerebellar learning” or “cerebellar programming”): Long term depression (LTD) and other mechanisms |
|
|
Compare Basal Ganglia to Cerebellum
|
BG:
1. input from prefrontal cortex output focused on supplementary motor areas 2. conscious initiation and lannning of movement C 1. wider input, output focused of area 4 (primary motor) 2. preprogrammed automated movements |
|
|
Cerebellum lesions and associated deficits
|
• Archicerebellum: Unsteadiness, swaying, falling. Tendency to fall backwards
when walking. Muscle tone not changed all the time. No asynergy or tremor in the limbs. Signs are usually bilateral. • Paleocerebellum: no specific deficits known in humans but could be similar to decerebration in animal experiments. • Neocerebellum (incl. paravermal regions i.e. parts of spinocerebellum): loss of muscle tone and fatigue, asynergia, dysmetria (hypermetria, pastpointing), intention tremor, dysdiadochokinesia (inability to perform rapid successive movements), nystagmus, speech disturbances (slurred speech, separating of syllables). |
|
|
Main functions of cerebellum
|
• Maintaining posture and balance while standing and moving (vestibulocerebellum).
• Monitoring the movement as it is executed (spinocerebellum) • Coordinating synergy of mucle activity in groups of muscles to generate complex movements (cerebrocerebellum) • Integrating of sensory input to help to plan and execute complex and precise movement essential in activities such as sports or playing musical instruments (spinocerebellum, visuocerebellum, audiocerebellum, very probably cerebrocerebellum, too). Automation of such movements through cerebellar “learning” (cerebellum as a computer?). • Automation of complex mental activities (calculus)? • Involvement of cerebellum in emotions, cognition, language..???* |