Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
Cardiac Output
|
@ rest ~5L/min
rest of body depends on it CO = HR x SV |
|
|
Parasympathetic Nervous System
Factors Affecting HR |
Negative chronotropic & dromotropic effects
-SA node, atria, & AV node have parasymp vagal innervation -ventricle has limited innerv. -NT = Ach -acts on muscarinic receptors -Neg Chronotropic effect: decreases HR by decreasing rate of phase 4 depolarization -less Na channels, less steep longer time to reach threshold -fewer AP occur in time bc threshold is reached slower & less frequently -Neg dromotropic effect: decrease CV thru AV node -ECG: PQ segment will be longer, longer periods of time bw QRS segments |
|
|
Sympathetic Nervous System
Factors Affecting HR |
-SA node, atria, AV node, & ventricles have symp innerv (T1-4)
-NT = NE acts on B1 receptors -Pos. Chronotropic: increases HR by rate of phase 4 depolarization -more AP occur per unit time bc the threshold pot is reached more quickly & therefore more freq -more Na channels opened fires @ faster rate -Pos. Dromotropic: increase CV thru AV node -problem when ventricles don't fill properly (lower SV) which decreases CO, less blood to systemic in each pump |
|
|
Hormone Factors Affecting HR
|
-Epi/NE: adrenal medulla, exert similar as SNS,
-imp during stress, exercise, & excitement + chrono & drono -Thyroid (T3&4): elevate HR @ rest -feels like racing heart (pounding chest) -upregulate B1 receptors (increase # of receptors on tissue) thus more receptors to bind to = more physiological response |
|
|
Ion Factors Affecting HR
|
-hyperkalemia & hypokalemia can decrease HR (K)
-age: younger = faster HR metabolic demand higher bc growth, older = HR age slower -Male/Female: males tend to have slower HR -Fitness: marathon runners, resting HR ~40 (very low) bc CO is so high, can pump out a lot of blood in 1 stroke -Body Temp: high = high HR, low = low HR |
|
|
Factors Affecting Stroke Volume
|
-Preload (Frank-Starling Mxn)
-Inotropism (cardiac contractility) -Afterload |
|
|
Preload
|
-heart very elastic, load/stretch on ventricular cardiac muscle before it contracts
-F-S law: w/in physiological limits (intrinsic influence); more ventricles are filled the more force of contraction = heterometric regulation |
|
|
Length-Tension Relationship in the Ventricle
|
-F-S law works in physiol. limits
-increase in EDV cause increase in ventricular fiber length which produces an increase in tension -heart has a range of length that it can form the most cross-bridges -stretched too far: myosin & actin too far from one another can't make x-bridges -not stretched/compacted: overlap of actin/myosin blocks ability of x-bridges to interact |
|
|
Stretch-Calcium Relationship
|
-stretch of myocardium by ventricular filling enhance affinity of troponin C for Ca & increase Ca uptake & release from SR
-more Ca = greater force of contraction |
|
|
Cardiac Contractility
Inotropism |
-independent of F-S law, extrinsic influence
-SNS has + inotropic effect on heart: cause increase in SV at a constant preload -enhance contractility = more complete ejection (lower ESV & greater SV) -homometric regulation |
|
|
Factors Affecting Stroke Volume
|
-Preload (Frank-Starling Mxn)
-Inotropism (cardiac contractility) -Afterload |
|
|
Preload
|
-heart very elastic, load/stretch on ventricular cardiac muscle before it contracts
-F-S law: w/in physiological limits (intrinsic influence); more ventricles are filled the more force of contraction = heterometric regulation |
|
|
Length-Tension Relationship in the Ventricle
|
-F-S law works in physiol. limits
-increase in EDV cause increase in ventricular fiber length which produces an increase in tension -heart has a range of length that it can form the most cross-bridges -stretched too far: myosin & actin too far from one another can't make x-bridges -not stretched/compacted: overlap of actin/myosin blocks ability of x-bridges to interact |
|
|
Stretch-Calcium Relationship
|
-stretch of myocardium by ventricular filling enhance affinity of troponin C for Ca & increase Ca uptake & release from SR
-more Ca = greater force of contraction |
|
|
Cardiac Contractility
Inotropism |
-independent of F-S law, extrinsic influence
-SNS has + inotropic effect on heart: cause increase in SV at a constant preload -enhance contractility = more complete ejection (lower ESV & greater SV) -homometric regulation |
|
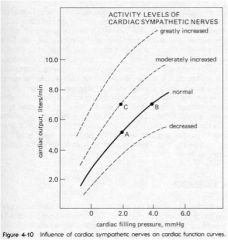
Heart A:
EDV = 130ml ~5L/min Heart B: -EDV = 160ml ~7 L/min Heart C: -EDV = 130 ml ~7L/min How C more than A? |
Heart C under SNS control: NE on B1 receptors
-ventricle contracts more forcefully no matter how much blood is filling -Heart C will have a lower ESV than Heart A bc contracting out more blood |
|
|
Mechanism of Cardiac Contractility
Inotropism Affects of B-Blockers |
1. increase in inward Ca current during plateau of each cardiac AP
2. increase the activity of the SERCA pumps -more Ca accum by SER & thus more Ca is avail for release in subsequent beats -decrease symp effect -decrease HR & SV therefore inhibit these 2 mxns |
|
|
Afterload
|
-load of the heart must overcome after & while it contracts
-back pressure exerted on the aortic & pulmonary semilunar valves by arterial blood in the aorta & pulmonary trunk -increase afterload: ventricle must pump blood against a higher pressure; result in lower SV -decrease afterload: the ventricle pumps blood against a lower pressure; result in an increase in SV |
|
|
Examples of increased afterload:
|
-vasoconstriction: (increased systemic vascular resistance)
-increased BV or viscosity -vasodilators often used to decrease afterload, thus decrease myocardial O2 demand, decrease pressure ex: nitroglycerine, liver rids of it quickly (high 1st pass effect) pt puts under tongue absorbs sublingually |
|
|
CO/Performance enhanced by:
|
increase preload
increase inotropy increase HR decrease afterload |
|
|
CO/Performance depressed by:
|
decrease preload
decrease inotropy decrease HR increase afterload |
|
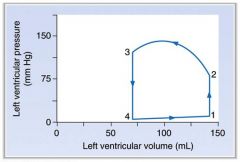
What's happening:
4 --> 1 1 1 --> 2 2 2 --> 3 3 --> 4 4 |
4-1: L ventricular filling (pressure slightly increasing)
1: mitral valve closes, EDV (S1) -right after QRS complex 1-2: isovolumetric ventricular contraction (no change in V) -pressure rising significantly 2: open aortic valve (decrease ventricular volume) 2-3: Rapid Ventricular Ejection 3: closer of aortic semilunar valve 3-4: isovolumentric ventricular relaxation 4: mitral valve opens |
|
|
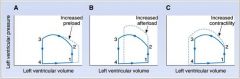
A: Increased preload
-more filling of L ventricle during diastole -bc filled w/ more blood will have more contraction to move extra blood B: Increased Afterload -filling w/ same amt blood, L ventricle has to develop more pressure during contraction -if afterload high - SV decreases C: Increased contractility (inotropy) -heart ejects a lot more blood |