![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
302 Cards in this Set
- Front
- Back
|
Inherited disorder of myocardial repolarization due to ion channels defect |
Congenital Long QT syndrome |
|
|
What is the risk of long QT syndrome? |
↑risk of Sudden Cardiac Death due to Torsade de pointes |
|
|
What are the syndrome associates with congenital long QT syndrome? |
Romano-Ward Syndrome Jervell And Lange-Nielsen Syndrome |
|
|
Autosomal dominant, pure cardiac phenotype (no deafness) |
Romano-Ward Syndrome (Congenital long QT syndrome) |
|
|
Autosomal recessive, sensorineural deafness and long QT interval |
Jervell and Lange-Nielsen syndrome (Congenital long QT syndrome) |
|
|
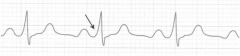
What is torsade de pointes? What can cause it?How can be treated? |
Polymorphic ventricular tachycardia. Characterized by shifting sinosoidal waveforms on ECG. Caused by: Drugs, ↓Mg2+, ↓K+ Tx: Mg2+ |
|
|
What drugs can cause torsade de points? |
Antiarrhythmics: Class III, Class IA Antibiotics/virals: Macrolides, Cloroquine, HIV protease inhibitors Antipsychotics: Haloperidol, respiredone Antidepressants: TCAs Antiemetics: Odansentron Others: Methadone |
|
|
Torsade de pointes can lead to...? What we can do about it? |
Ventricular Fibrillation. CPR → Defibrillation |
|
|
Autosomal dominant disorder + ECG pattern of pseudo-right bundle branch block + ST elevation in V1-V3? |
Brugada Syndrome |
|
|
In what population is Brugada syndrome most common? |
Asian males population |
|
|
Brugada Syndrome can lead to...? What we can do about it? |
Ventriculat tachyarrhythmias and sudden cardiac death. Tx: Implantable cardioverter-defibrillator |
|
|
Most common type of ventricular pre-excitation syndrome |
Wolf-Parkinson-White Syndrome |
|
|
Abnormal fast accesory conduction pathway from atria to ventricle |
WPW syndrome |
|
|
What is the bundle of Kent? What it does? In what disease we can find it? |
--Fast accesory conduction pathway from atria to ventricle. --Bypasses the AV node → ventricle depolarizes earlier --WPW syndrome |
|
|
What findings we can find on ECG in WPW syndrome? What this finding can lead to? |
Delta wave with widened QRS complex and shortened PR interval → SVT |
|
|
How can we treat WPW syndrome? |
Antiarrhythmics: Procanamide, Amiodarone |
|
|
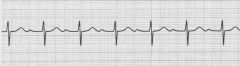
Atrial Fibrillation |
|
|
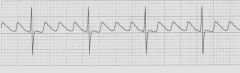
Atrial Flutter |
|
|
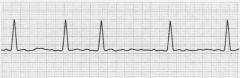
AV block 1st degree |
|
|
AV block 2nd degree type 1 |
|

|
AV block 2nd degree type 2 |
|

|
AV block 3rd degree |
|
|
What characteristic rhythm has Atrial fib? Describe relationship of waves on ECG. |
--Irregularly Irregular rhythm --No P wave in between irregularly QRS complexes |
|
|
Most common cause of Atrial fib? |
--HTN and coronary artery disease --Also HF. |
|
|
Atrial fib treatment. |
--Anticoagulation: heparin/warfarin --Rate control: ß-blockers, CCB --Rhythm control: Antiarrhythmics (Class IA, IC, III) --Cardioversion: if > 48hrs |
|
|
Rapid succesion of identical, back-to-back atrail depolarization waves on ECG |
Atrial Flutter |
|
|
"Sawtooth" appearance on ECG |
Atrial Flutter |
|
|
Completely erratic rhythm with no identifiable waves on ECG |
Ventricle Fibrillation |
|
|
How to proceed when a ventricular fibrillation is on ECG for more than 30 seconds? |
CPR → Defribrillation |
|
|
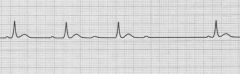
What arrhythmia does have PR interval prolonged (>200msec) on ECG? |
AV block 1st degree |
|
|
What arrhythmia does have a progressive lengthening of PR interval until beat is "dropped" on ECG? |
AV block 2nd degree type 1 |
|
|
On ECG: A P wave not followed by QRS complex; usually asymptomatic |
AV block 2nd degree type 2 |
|
|
What is regularly irregular rhythm? Mention an arrthythmia where can be found. |
Variable RR interval with a pattern. AV block 2nd degree type 1 |
|
|
Dropped beats that are not preceded by a change in the length of the PR interval on ECG |
AV block 2nd degree type 2 |
|
|
On ECG Atria and ventricle beat interdependently of each other w/ Atrial rate > ventricular rate. |
AV Block 3rd degree |
|
|
What bacteria can cause an AV block? |
Borrelia burgdorferi (Lyme Disease) |
|
|
What are the 5Ts of congenital heart diseases? |
Truncus Arteriosus Transposition of the Great Vessels Tricuspid Atresia Tetralogy of Fallot Total Anomalus Pulmonary Venous Return |
|
|
Are the 5 Ts of congenital heart diseases belongs to right-to-left or left-to-right shunts? |
Right-to-left Shunts |
|
|
Which shunt gives early cyanosis? Late cyanosis? |
Early cyanosis: --Right-to-left shunt Late cyanosis --Left-to-right shunt |
|
|
What is the problem in persistence truncus arteriosus? |
Truncus arteriosus fails to divide into pulmonary trunk and aorta due to lack of aorticopulmonary septum |
|
|
Most patient are accompanied by what septal defect in truncus arteriosus. |
VSD |
|
|
What is the problem in transposition of the great vessels? |
Failure of AP septum to spiral Aorta leaves RV (anterior) and pulmonary trunk leaves LV (posterior) → separation of systemic and pulmonary circulation |
|
|
What we can see in transposition of the great vessels for them to survive? |
Septal defects --VSD, PDA, patent foramen ovale |
|
|
What is tricuspid atresia? What the patients requieres to survive? |
Absence of tricuspid valve and hypoplastic RV. Requieres Septal Defects --ASD and VSD |
|
|
Mention the anomalies of Tetralogy of Fallot |
Pulmonary Stenosis Right Ventricular Hypertrophy Overriding of Aorta VSD |
|
|
What characteristic shape we can see on X-ray of a patient with Tetralogy of Fallot |
Boot-shaped heart |
|
|
Outline the physiologic events that leads to the symptoms of Tetralogy of Fallot. |
Pulmonary Stenosis forces right-to-left shunt flow across VSD → RVH "Tet spells" often caused by crying, fever, exercise due to exarcerbation of RV outflow obstruction. |
|
|
What maneuver can help the symptoms of Tetralogy of Fallot? What parameters affects? |
Squatting ↑Systemic vascular resistance: ↑Afterload ↑Preload (venous return) ↓Right-to-left shunt: improves cyanosis |
|
|
What is the problem on Total Anomalus Pulmonary Veins Return? |
Pulmonary veins drain into the right heart circulation |
|
|
What septal defects are associated with TAPVR? For what purpose they exist? |
ASD, PDA: allow right-to-left shunt to maintain CO |
|
|
What is Ebstein anomaly? |
--Displacement of tricuspid valve leaflet downward into RV --"Atrializing" the ventricle |
|
|
What heart conditions are associated with Ebstein Anomaly? |
Tricuspid regurgitation and right HF |
|
|
Most common cause of Ebstein Anomaly |
Lithium exposure in utero |
|
|
What is the most common congenital heart defect? |
VSD |
|
|
Mention left-to-right shunts anomalies in order of frecuency. |
VSD>ASD>PDA |
|
|
What findings we can expect in VSD? |
--O2 sat ↑ in RA,RV and pulmonary artery --Holosystolic harsh-sounding murmur; loudest @ tricuspid area |
|
|
Are VSD self resolve or they must be surgically fixed? |
Most of them self resolve Larger lesions may lead to LV overload and HF → must be surgically corrected |
|
|
What findings we can expect in ASD? |
O2 sat ↑ RA, RV, PA Loud S1 Wide fixed split S2 Diastolic murmur @ tricuspid area |
|
|
What are the most common defects in ASD? |
1. Ostium Secundum defect 2. Patent Foramen Ovale 3. Ostium Primum defect |
|
|
What are the symptoms of ASD? |
Ranges from asymtomatic to HF Classically: easy fatigability |
|
|
Outline the events in patent ductus arteriosus |
Normally in fetal period: Right-to-left shunt Neonate period: ↓ pulmonary vascular resistance → shunt becomes left-to-right → progressive RVH and/or LVH and HF. |
|
|
In what congenital disease we can find a PDA? |
TGV TAPVR |
|
|
How a PDA can be closed? How to maintain it open? |
Close: Indomethacin (NSAID) Open: Prostagladins (E1,E2) |
|
|
How do you describe the murmur heard in PDA? |
Continuos machine-like murmur |
|
|
What happens if we keep a PDA untreated? |
Can eventually result in late cyanosis in the lower extremities (differential cyanosis) Can evolve into Eisenmenger syndrome. |
|
|
What is Eisenmenger syndrome? |
Uncorrected left-to-right shunt (VSD, ASD, PDA) → ↑pulmonary blood flow → pathologic remodeling of vasculature → pulmonary arterial hypertension → RVH → shunts becomes right-to-left |
|
|
Late Cyanosis + clubbing + polycythemia |
Eisenmenger Syndrome |
|
|
What is coarctation of the aorta? |
Aortic narrowing near insertion of ductus arteriosus |
|
|
Hypertension in upper extremities + weak delayed pulse in lower extremities |
Coarctation of Aorta |
|
|
What defects or conditions are associated w/ Coarctation of the Aorta? |
Turner Syndrome Bicuspid valve |
|
|
In what disease we can see notching of ribs on CXR? What caused this? |
Coarctation of Aorta. With age, intercoastal arteries enlarge due to collateral circulation; arteries erodes ribs |
|
|
What are the complications of Coarctation of the Aorta? |
HF ↑risk of cerebral hemorrhage (berry aneurysm) Aortic rupture Possible endocarditis Aortic Regurgitation |
|
|
What congenital cardiac defect we can see in alcohol exposure in utero? |
VSD, PDA, ASD, Tetralogy of Faloot |
|
|
What congenital cardiac defect we can see in congenital rubella?
|
PDA, Pulmonary stenosis, septal defects |
|
|
What congenital cardiac defect we can see in Down syndrome?
|
AV septal defects (endocardial cushions defects), VSD, ASD |
|
|
What congenital cardiac defect we can see in an infant of a diabetic mother?
|
Transposition of the great vessels |
|
|
What congenital cardiac defect we can see in Marfan syndrome?
|
MVP, thoracic aortic aneurysm and dissection, aortic regurgitation |
|
|
What congenital cardiac defect we can see in prenatal lithium exposure?
|
Ebstein Anomaly |
|
|
What congenital cardiac defect we can see in Turner syndrome?
|
Bicuspid aortic valve, coarctation of the aorta |
|
|
What congenital cardiac defect we can see in Williams syndrome?
|
Supravalvular Aortic Stenosis |
|
|
What congenital cardiac defect we can see in 22q11 syndrome?
|
Truncus Arteriosus, Tetralogy of Fallot |
|
|
How do you define HTN? |
Persistent systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg |
|
|
Risk Factors for HTN |
Modifiable: --obesity, diabetes, physical inactivity, excess salt intake, excess alcohol intake Non-modifialbe --family history, African American > Caucasian > Asian |
|
|
What is an hypertensive urgency? |
Severe hypertension (≥180 / ≥120 mmHg) without acute end-organ damage |
|
|
What is an hypertensive emergency? |
Severe HTN (≥180 / ≥120 mmHg with evidence of acute end-organ damage |
|
|
What end-organ damage can be seen in a patient with severe HTN? |
Encephalopathy, Stroke, Retinal Hemorrhages and exudes, papilledema, M, HF, aortic dissection, kidney injury, microangiopathy hemolytic anemia, eclampsia. |
|
|
What might cause secondary hypertension? |
Renal/renovascular disease (e.g. fibromuscular dysplasia) Primary Hyperaldosteronism |
|
"String of beads" appearance on Renal Artery |
Fibromuscular dysplasia seen in Renalvascular disease. Common cause of secondary HTN |
|
|
What HTN predisposes to? |
Coronary Arteries Disease Left ventricular Hypertension Heart Failure Atrial Fibrillation Aortic Dissection Aortic Aneurysm Stroke Chronic Kidney Disease Retinopathy |
|
|
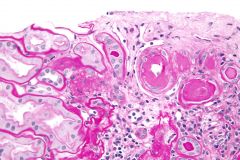
Sg: Plaques or nodules composed of lipid-laden histiocytes in skin |
Xanthomas |
|
|
Sg: Lipid deposit in tendons (especially Achilles) |
Tendinous Xantoma |
|
|
Sg: Lipid deposit in cornea |
Corneal Arcus |
|
|
What are the hyperlipidemia signs? |
Xanthomas, Xanthalesmas Tendinous Xanthomas Corneal Arcus |
|
|
Sg: Hardening of arteries, with arterial wall thickning and loss of elasticity |
Arteriosclerosis |
|
|
What type of vessels do arteriosclerosis affects? |
Affects small arteries and arterioles |
|
|
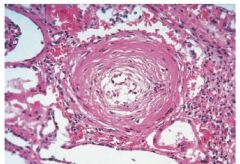
Sg: Thickening of the vessels wall in essential hypertention or diabetes mellitus |
Arteriosclerosis Hyaline type |
|
|
Sg: "Onion Skinning" in severe HTN with proliferation of smooth muscle cells |
Arteriosclerosis Hyperplastic type |
|
|
Which is more common: Arteriosclerosis or Monckeberg sclerosis? |
Arteriosclerosis |
|
|
What are the types seen in arteriosclerosis? |
Hyaline and Hypoplastic |
|
|
What type of vessels Monckeberg Sclerosis affects? |
Affects medium-sized arteries |
|
|
Sg: Calcification of internal elastic lamina and media of arteries |
Monckeberg Slerosis |
|

"Pipestem" appearance on X-ray |
Mockenberg Sclerosis |
|
|
Do Monckeberg Sclosis obstruct blood flow in the vessel affected? |
No. Vascular stiffening without obstruction. |
|
|
Arterosclerosis hyaline type |
|
|
What type of vessels do atherosclerosis affects? |
Elastic arteries and large- and medium-sized muscular arteries |
|
|
What vessels are the most affected by atherosclerosis? |
Abdominal Aorta > Coronary Artery > Popliteal > Carotid Artery |
|
|
What are the risk factor for Atherosclerosis? |
Modifiable: --smoking, HTN, hyperlipidemia (↑LDL), diabetes Non-modifiable: --Age, sex, (↑men and postmenopausal woman), family history |
|
|
Patient present with angina and claudication. What is the most likely diagnosis? |
Atheroslcerosis |
|
|
Outline the events that leads to an atherosclerotic plaque |
Endothelial cell dysfunction → macrophage and LDL accumulation → foam cell formation → fatty streak → smooth muscle migration (PDGF and FGF) → fibrous plaque → complex atheromas |
|
|
What are the cell involve in atherosclerosis? |
Endothelial cells Macrophages Smooth muscle cells |
|
|
What growth factors are involved in smooth cell migration? |
Platelet-derived growth factor (PDGF) Fibroblast growth factor (FGF) |
|
|
What are the complication of Atheroslcerosis? |
Aneurysm Ischemia Infarcts Peripheral vascular disease Thrombus → emboli |
|

|
Aortic Dissection May present with back/abdominal pain |
|
|
Male Patient with tobacco use history, atherosclerosis history with a palpable pulsatile abdominal mass. What is the most likely dx? |
Abdominal Aortic Aneurysm |
|
|
Obliterative endarteritis of vasa vasorum. May first lead to abdominal or thoracic aneurysm, dissection or coartation of the aorta? What organism may cause this? |
thoracic aortic aneurysm due to syphilis (t. pallidum) |
|
|
What aortic disease is associated with cystic medial degeneration? |
Thoracic Aortic Aneurysm |
|
|
What are the risk of factors of Thoracic Aortic Aneurysm? |
HTN Bicuspid aortic valve Connective tissue disease (e.g. Marfan syndrome) |
|
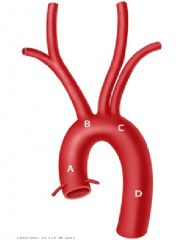
Patient involved in a motor vehicle accident most likely will injure which part of the aorta? |
C: Aortic isthmus (proximal descending aorta just distal to origin of the left subclavian artery) |
|
What are the types of this finding? |
Left: Stanford type A (proximal)→ involves ascending aorta --Tx: Surgery Right: Stanford type B (distal) → involves descending aorta and/or aortic arch --Tx: ß-blockers then vasodilators |
|
|
A pt with tearing chest pain (sudden onset) radiating to the back +/- markedly unequal BP in arms |
Aortic Dissection |
|
|
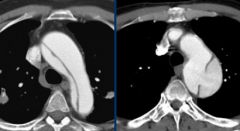
What aortic disease may have longitudinal intimal tearing forming a false lumen, On CXR: mediastinal widening? |
Aortic Dissection |
|
|
Angina usually 2° to ischemic myocardium 2° to coronary artery narrowing or spasm |
Stable Angina |
|
|
Angina usually with ST depression on ECG and resolve with nitroglycerin |
Stable Angina |
|
|
Angina that occurs at rest 2ry to coronary artery spasm |
Variable (Prinzmental) |
|
|
Angina with transient SR elevation on ECG |
Variable (Prinzmental) |
|
|
Angina triggered by tobacco, cocaine, and triptans |
Variable (Prinzmental) |
|
|
How to treat a variable angina? |
Tx: Ca2+ channel blockers, nitrates ans smoking cessation |
|
|
Angina due to thrombosis with imcomplete coronary occlusion |
Unstable |
|
|
Angina +/- ST depression and/or T-wave inversion on ECG but no cardiac biomarkers elevation |
Unstable |
|
|
Vessels are maximally dilated at baseline; distal to coronary stenosis. What may you suspect? |
Coronary Steal Syndrome |
|
|
Why vasodilators makes worse the conditions seen in coronary steal syndrome? |
In CSS, vessels are already dilated because of an obstruction of a vessel if vasodilators are administrated it will dilates more the coronary arteries making more blood flow away from the obstructed area. |
|
|
What heart condition may cause death from cardiac cause within 1 hour of Synmptoms? |
Sudden Cardiac Death |
|
|
What is the most common cause of death in SCD? |
Ventricular Fibrillation |
|
|
What are the causes of Sudden Cardiac Death? |
--Coronary arteries disease (70%) --Cardiomiopathy (hypertrophic dilated) --Hereditary ion channelopathies (long QT, brugada) |
|
|
Heart condition with progressive onset of HF over many years due to chronic ischemic myocardial damage. |
Chronic Ischemic heart disease |
|
|
STEMI or Non-STEMI: Trasmural Infarcts Full thickness of myocardial wall involved |
ST-segment Elevation MI (ST elevation + Q wave on ECG) |
|
|
STEMI or Non-STEMI: Subendocardial infarts Subendocardium (inner 1/3) especially vulverable to ischemia |
Non-ST-segment elevation MI (ST depression on ECG) |
|
|
Myocardial Infarction are more often due to...? |
Rupture of coronary artery atherosclerotic plaque. |
|
|
Light microscopy: Early coagulative necrosis, release of necrotic cell contents into blood; edma, hemorrhage, wavy fibers. Neutrophils appear. What time do this correspond? |
Myocardial Infarction 0 -24 hrs |
|
|
What complication does a MI have in the first 24 hrs? |
Ventricular arrhthmias, HF, cardiogenic shock |
|
|
What is reperfusion injury and how many hours/days can occurs after an MI? |
--Reperfusion injury: associated with the generation of free radicals → hypercontraction of myofibrils through ↑ free calcium influx --Occurs in the first 24 hrs after injury |
|
|
Light microscopy: Extensive coaugulative necrosis. Tissue surrounding infarct shows acute inflammation w/ neutrophils What time this coincides after an MI? |
1 - 3 days after MI |
|
|
What complication can occurs in day 1 - 3 after a MI? |
Postinfarction fibrinous pericarditis |
|
|
Light microscopy: Macrophages, then granulation tissue at margins What time this coincide after an MI? |
3 - 14 days after a MI |
|
|
Free wall rupture → tamponade Papillary muscle rupture → Mitral regurgitation Interventricular septal rupture (due to macrophages-mediated structural degradation) LV pseudoaneurysm (risk of rupture) What time this coincides after an MI? |
Complication after in the first two weeks (3 - 14 days) after an MI |
|
|
Contracted scar complete What time this coincide after an MI? |
More than 2 week after an MI |
|
|
Autoimmune phenomenon resulting in fibrinous pericarditis What time this coincide after an MI? |
Dressler Syndrome Complication after 2 week of a MI |
|
|
HF, arrhythmias, true ventricular aneurysm (risk of mural thrombosis) What time this coincide after an MI? |
More than 2 weeks after a MI |
|
|
In the first 6 hrs after a MI, what diagnostic method is the best? |
ECG |
|
|
Which cardiac biomarker is more specific to diagnose a MI? |
Cardiac Troponin I (rises after 4hrs; peaks at 24hrs; ↑ for 7 -10 days) CK-MB is not specific becuase it can be released from skeletal muscle (rises after 6 -12 hrs) |
|
|
Which cardiac biomarker is useful in diagnosing reinfarction following acute MI? |
CK-MB becuase levels return to normal after 48hrs |
|
|
What changes we can see on ECG after a MI? |
ST elevation (STEMI, trnasmural infarction) ST depression (NSTEMI, subendocardial infarct) Hyperacute (peaked) T wave T-wave inversion New left bundle branch block Pathologic Q wave Poor R wave progression (evolving or old trnasmural infarct) |
|
|
On ECG you see leads with ST elevation or Q waves on: V1 - V2 What region of the heart you might suspect to be injured? What artery supplies this region? |
Anteroseptal (LAD) |
|
|
On ECG you see leads with ST elevation or Q waves on: V3 - V4
What region of the heart you might suspect to be injured? What artery supplies this region? |
Anteroapical (distal LAD) |
|
|
On ECG you see leads with ST elevation or Q waves on: V5 - V6
What region of the heart you might suspect to be injured? What artery supplies this region? |
Anterolateral (LAD or LCX) |
|
|
On ECG you see leads with ST elevation or Q waves on: I, aVL
What region of the heart you might suspect to be injured? What artery supplies this region? |
Lateral (LCX) |
|
|
On ECG you see leads with ST elevation or Q waves on: II, III, aVF
What region of the heart you might suspect to be injured? What artery supplies this region? |
Inferior (RCA) |
|
|
On ECG you see leads with ST elevation or Q waves on: V7 - V9 and ST depression + tall R wave on: V1 - V3
What region of the heart you might suspect to be injured? What artery supplies this region? |
Posterior (PDA) |
|
|
What is an Important cause of death before reaching the hospital after MI? |
cardiac arrthymia |
|
|
Sharp pain + aggravated by inspiration + friction rub after MI What time this coincide after an MI? |
Postinfarction fibrinous pericarditis (1 - 3 days after MI) |
|
|
Posteromedial papillary muscle rupture can result in ...? How long after an MI this can occur? Which blood vessel supply this structure? |
Mitral regurgitation (After 2 - 7 after MI) Posterior Descending artery |
|
|
Contained free wall rupture can decrease _____ and have a risk of ____, and_____. |
Ventricular Pseudoaneurysm formation (3 -14 days after MI) ↓Cardiac Output Risk of arrhythmia, embolus from mural thrombosis |
|
|
Free wall rupture leads to _____. |
5 -14 days after MI Cardiac tamponade |
|
|
Outward bulge with contraction ("dyskinesia") associated with fibrosis |
True ventricular aneurysm ( > 2 weeks after MI) |
|
|
Treatment for Unstable angina/NSTEMI (7) |
Anticouagulation (heparin) Antiplatelet therapy (aspirin + ADP receptor inhibitor [clopidrogrel]) ß-blocker ACE inhibitors Statins Sx control w/ nitroglycerin and morphine |
|
|
Treatment for STEMI (7+1) |
Tx for Unstable angina/NSTMI + repefusion therapy (percutaneous coronary intervention preferred over fibrinolysis) |
|
|
What is the most common cardiomyopathy? |
Dilated cardiomyopathy (90%) |
|
|
Mention etiologies that may cause dilated cardiomyopathy. |
Most often: Idiopathic or Familial Others: Chronic alcohol abuse, Wet beriberi, Coxsackie B viral myocarditis, Chagas Disease, Cocaine use, Doxorubicin toxicity, hemochromatosis, sarcoidosis, peripartum cardiomyopathy |
|
|
What are the ABCCCD of dilated cardiomyopathy |
Etiologies: Alcohol abuse (chronic) Beriberi (wet) Coxsackie B virus (myocarditis) Chagas Disease Doxorubicin (toxicity) |
|
|
HF + S3 + systolic regurgitant murmur + balloon appearance of heart on CXR |
Dilated cardiomyopathy |
|
|
What abnormal heart sound can be heard in dilated cardiomyopathy? |
S3 |
|

Balloon appearance of heart on CXR |
Dilated cardiomyopathy |
|
|
Treatment for dilated cardiomyopathy (7) |
Na+ restriction, ACE inhibitors, ß-blockers, diuretics, digoxin, ICD, heart transplant. |
|
|
What is eccentric hypertrophy? With what cardiomyopathy is associated? |
Sarcomere added in series Associated w/ Dilated cardiomyopathy |
|
|
What is marked ventricular hypertrophy? With what cardiomyopathy is associated? |
Myofibrillar disarray and fibrosis Associated w/ Hypertrophic cardiomyopathy |
|
|
What type of dysfunction is seen in dilated cardiomyopathy? |
Systolic dysfunction |
|
|
What type is dysfunction is seen in hypertrophic cardiomyopathy? |
Diastolic Dysfunction |
|
|
What is the most common cause of hypertrophic cardiomyopathy? |
Familial (Autosomal dominant) → commonly a ß-myosin heavy-chain mutation) |
|
|
Which cardiac disease is associated with Friedreich Ataxia? |
Hypertrophic cardiomyopathy |
|
|
What hear condition causes syncope during exercise and may lead to SCD due to ventricular arrhythmia? |
Hypertrophic cardiomyopathy. Especially in young athletes |
|
|
What abnormal heart sound can be heard in hypertrophic cardiomyopathy? |
S4 |
|
|
S4 + systolic murmur + may see mitral regurgitation due to impaired mitral valve closure |
Hypertrophic cardiomyopathy |
|
|
Is the size of the heart is normal, bigger or smaller in hypertrophic cardiomyopathy? In dilated cardiomyopathy? |
HC: Normal DC: Bigger |
|
|
Treatment for hypertrophic cardiomyopathy (4) |
Cessation of high-intensity athletics, ß-blocker, Non-dihydropyridine Ca2+ channel blockers, ICD (if pt is high risk) |
|
|
Asymmetric septal hypertrophy and systolic anterior motion of mitral valve leads to what? |
Outflow obstruction → dyspnea, possible syncope in Obstructive hypertrophic cardiomyopathy |
|
|
The major causes of this cardiomyopathy is sarcoidosis, amyloidosis post radiation fibrosis, endocardial fibroelastosis and hemochromatosis |
Restrictive/infiltrative cardiomyopathy |
|
|
What cardiac disease is associated with Loffler syndrome? |
Restrictive/infiltrative cardiomyopaty |
|
|
What dysfunction can be seen in restrictive/infiltrative cardiomyopathy? |
Diastolic dysfunction |
|
|
Cardiomyopathy that has low-voltage ECG despite thick myocardium. |
Restrictive/infiltrative cardiomyopathy |
|
|
Shortness of breath when lying down + Breathless awakening from sleep + rales |
Left heart failure |
|
|
Nutmeg liver + venous distension + pitting edema |
Right heart failure |
|
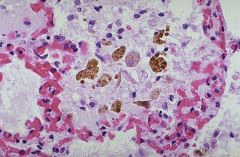
Presence of hemosiderin-laden macrophages in lungs What heart condition you might suspect? |
Left heart failure |
|
|
What are the most common cause of Right heart failure and Cor pulmonale? |
RHF: due to LHF CP: RFH due to pulmonary cause |
|
|
What is systolic dysfunction? |
Reduced EF, ↑EDV; ↓contractility often 2° to ischemia/MI or dilated cardiomyopathy |
|
|
What is diastolic dysfunction? |
Preserve EF, normal EDV; ↓compliance often 2° to myocardial hypertrophy |
|
|
What drug reduce mortality in HF? |
--ACE inhibitors (-pril) --ARB (-artan) --Aldosterone antagonist (spironolactone/eplerenone) --ß-blockers (metoprolol, carvedilol) |
|
|
What drugs are used to relief the Sx in HF? |
---Loop Diuretics in severe cases (Furosemide, bumetanide, torsemide) or Thiazide Diuretes in mild cases (Hydrochlorothiazide, chlorthalidone, metolazone) ---Digoxin ---Vasodilators (nitrates, hydralazine*) *certain pts |
|
|
How to treat a pt w/ chronic HF? |
ACE inhibitors + Aldosterone Antagonist + ß-blockers Relief of Sx: Loop or thiazide diuretics, Digoxin |
|
|
How to manage an acute HF? |
NO LIP Nitrates Oxygen Loop Diuretics Inotropic Drug (Dobutamine) Positioning (Sit up pt) |
|
|
What is the pulmonary capillary wegde pressure (PCWP)? |
PCWP = Measure left atrium pressure (via a Swan-Ganz catheter) = Left Diastolic Pressure PCWP ~ 12 mmHg; LDP ~ 10 mmHg |
|
|
What is BNP? what differs from ANP? |
Brain Natriuretic Peptide = released from the ventricle in response to ↑ tension Atrial natriuretic peptide = released from atria in response to ↑blodd volume/pressure |
|
|
How does ANP works? |
Acts via cGMP → vasodilation + ↓Na+ reabsorption at the renal collecting tubules. Dilates afferent renal arterioles + constrict efferent arterioles → promotes diuresis ans constribute to "aldosterone escape" mechanism. |
|
|
What blood test can be done to diagnose HF? |
BNP (very good negative predictive value) |
|
|
What recombinant form of drug can be use to treat HF? |
BNP → nesiritide |
|
|
Which has longer half-life, ANP or BNP? |
BNP |
|
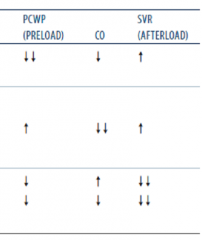
What type of shock correspond the following PWCP and SVR values? |
1) Hypovolemic Shock 2)Cardiogenic/Obstructive 3)Distributive |
|
|
Mention causes of hypovelemic, cardiogenic/obstructive and distributive shocks. |
--Hypovelemic: Hemorrhage, dehydration, burns --Cardiogenic: Acute MI, HF, valvular dysfunction, arrhythmia --Obstructive: Cardiac tamponade, pulmonary embolism --Distributive: Sepsis, anaphylaxis, CNS injury |
|
|
Skin condition in shock: Cold, clammy skin? Warm, dry skin? |
Cold, clammy skin: hypovolemic, cardiogenic/obstructive Warm, dry skin: Distributive |
|
|
Treatment used in shock: IV fluid only? IV fluis + pressor? Inotropes, diuresis? Relieve obstruction? |
IV fluids only: hypovolemic IV fluids + pressor: Distributive Inotropes, diuresis: Cardiogenic Relieve ibstruction: Obstructive |
|

Round white spots on retina surrounded by hemorrhage. What is the most likely dx? |
Roth spots (Bacterial endocarditis) |
|

Tender raised lesions on finger or toe pads |
Osler nodes (Bacterial endocarditis) |
|

Small, painless, erythematous on palm or sole |
Janeway lesions (Bacterial endocarditis) |
|
|
Glomerulonephritis + septic arterial or pulmonary embolis + splinter hemorrhages on nail bed |
Bacterial Endocarditis |
|
|
What valve is most common affects in bacterial endocarditis? |
Mitral valve tricuspid valve in IV drug abuse |
|
|
What organism is most common in acute bacterial endocarditis? |
S. aureus (high virulence) |
|
|
What organism is most common in subacute bacterial endocarditis? |
Viridans streptococci (low virulence) |
|
|
How do you describe the vegetation found in acute and subacute bacterial endocarditis? |
ABE: Larger vegetations on previously normal valve SABE: Smaller vegetations on congenital abnormal or diseased valves |
|
|
What procedure can be a sequela of bacterial endocarditis? |
Dental Procedure |
|
|
What organism may cause bacterial endocarditis in colon cancer patients? In patients with prostatic valves? |
S. bovis = colon cancer patients S. epidermis = prostatic valves |
|
|
What may cause nonbacterial endocarditis? |
Marantic/thromobic 2ry to malignancy, hypercoagulable state, or lupus |
|
|
If culture comes negative in bacterial endocarditis (BE), what organism may cause BE? |
--Coxiella burnetti (Q fever; cattle/sheep amniotic fluid) --Bartonella (Cat scratch fever, bacillary angiomatosis) --HACEK (Haemophilis, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) |
|
|
Tricuspid valve endocarditis is associated with ____? What organism can cause it? |
IV drug abuse. S. aureus, Pseudomonas and Candida |
|
|
What heart related disease is a consequence of pharyngeal infection with group A ß-hemolytic streptococci? |
Rheumatic fever |
|
|
Which valves does rheumatic heart disease affects? |
Mitral > aortic >> tricuspid (high-pressure valves affected most) |
|
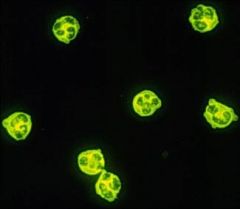
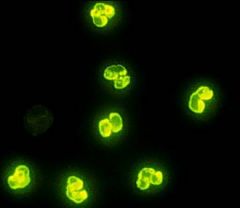
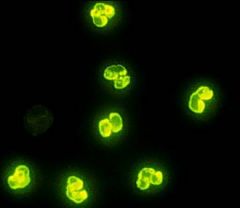
Granulomas with giant cells. What disease you might suspect? |
Aschoff bodies (Rheumatic heart disease) |
|
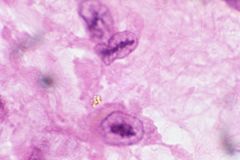
Enlarged macrophage with ovoid, wavy, rod-like nucleus. What disease you might suspect? |
Anitschkow cells (rheumatic heart disease |
|
|
What valve lesion can be seen as an early lesion in rheumatic heart disease? As a late lesion? |
EL: Mitral regurgitation LL: Mitral Stenosis |
|
|
What blood test can be done to diagnose rheumatic fever? |
Anti-streptolysin O (ASO) |
|
|
What type of hypersensitivity occurs in rheumatic heart disease? How does it do it? |
HS II; Antibodies to M protein cross-react with self antigens (molecular mimicry) |
|
|
What drug can be used for prophylaxis or to treat Rheumatic fever? |
Penicillamin |
|
|
What are the major criteria for rheumatic fever? |
J♥NES Joint (migratory polyartheritis) ♥ (carditis) Nodules in skin (subcutaneous) Erythema marginatum Sydenham chorea |
|
|
Sharp pain aggravated by inspiration and relieve by sitting up and leaning forward + friction rub |
Acute pericarditis |
|
|
What heart disease have an ECG change include widespread ST-segment elevation and/or PR depression? |
Acute pericarditis |
|
|
What are the Causes of acute pericarditis? |
Most common: idiopathic (viral) Confirm infection (coxsackie virus) Neoplasia Autoimmune (SLE, RA) Uremia CV (acute STEMI/Dressler syndrome) Radiation therapy |
|
|
WHat are the Types of pericarditis? |
--Fibrinous = Load friction rub = dressler syndrome, uremia, radiation --Serous = viral pericarditis, non infectious inflammatory disease --Suppurative = bacterial infection |
|

What is the most likely dx? |
Cardiac tamponade |
|
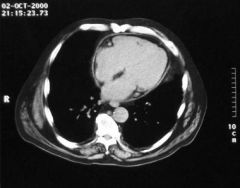
What is the most likely dx? |
Pericarditis |
|
|
Hypotension + distended neck veins + distant heart sounds |
Beck traid (Cardiac Tamponade) |
|
|
What heart disease may have an ECG that shows low-voltage QRS and electrical alternans (due to "swinging" movement of heart in large effusion)? |
Cardiac tamponade |
|
|
What is Pulsus paradoxus? With what conditions is associated? |
↓in amplitude of systolic BP by > 10mm Hg during inspiration. ---Seen in cardiac tamponade, asthma, obstructive sleep apnea, pericarditis, croup |
|
|
What is Pulsus parvus et tardus? With what condition is associated? |
Pulses are weak with delayed peak. ---Seen in aortic stenosis |
|
|
What layers has to be pierced in order to do a periocardiocentesis? |
Skin → superficial/deep fascia → pectoralis major muscle → external/internal costal membrane → thoracic muscle → fibers of pericardium → parietal layer of serum pericardium |
|
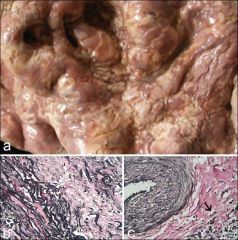
"tree bark" appearance of aorta |
3° syphilis |
|
|
What disease may disrupt vasa vasorum of the aorta with consequence atrophy of vessel wall? |
3° syphilis |
|
|
Dilatation of the aorta and valve ring + calcification of aortic root and ascending aortic arch |
3° syphilis |
|
|
What are the cardiovascular consequence of 3° syphilis? |
Aneurysm of ascending aorta or aortic arch, aortic insifficiency |
|
|
What is the most common cause of cardiac tumors? |
Metatasis --Melanoma, Lymphoma |
|
|
Most common 1° tumor in adult |
Myxoma (90% occur in atria; mostly left atrium) |
|

"Ball valve" obstruction in left atrium |
Myxoma |
|
|
Most frequent 1° cardiac tumor in children |
Rhabdomyosarcoma |
|
|
What disease is associated with rhabdomyosarcoma? |
Tuberous sclerosis |
|
|
What heart condition may cause an early diastolic "tumor plop" sound? |
Myxoma |
|
|
What is Kussmaul sign? In what diseases can be seen? |
↑ in JVP on inspiration instead of a normal ↓ Seen in constrictive pericarditis, restrictive cardiomyopathy, right atrial or ventricular tumors |
|
|
Outline the events seen in Kussmaul sign |
Inspiration → negative intrathoracic pressure not transmitted to heart → impaired filling of right ventricle → blood back up into venae cavae → JVD |
|
|
Which vasculitides affects large-sized vessels? |
Temporal (giant cell) arteritis Takayasu arteritis |
|
|
Which vasculitides affects medium-sized vessels? |
--Polyarteritis nodosa --Kawasaki disease (mucocutaneous lymph node syndrome --Buerger disease (thromboangiitis obliterans) |
|
|
Which vasculitides affects small-sized vessels? |
--Granulomatosis with polyangititis (Wegener) --Microscopic polyangiitis --Eosinophilic granulomatosis with polyangiitis (Chrug-Strauss) --Henoch-Schonlein purpura |
|
|
Usually elderly females + unilateral headache + pain after chewing + pain in shoulder and hips |
Giant cell (Temporal) Arteritis *Pain after chewing (jaw claudication) **Pain in shoulder and hips (polymyalgia rheumatica) |
|
|
Vasculitis with ↑ ESR + focal granulomatous inflammation |
Giant cell (temporal) arteritis |
|
|
What vasculitis most commonly affects branches of carotids artery? |
Giant cell (temporal) arteritis |
|
|
What vasculitis may lead to irreversible blindness due to ophthalmic artery occclusion? |
Giant cell (temporal) arteritis |
|
|
What vasculitis is associated with polymyalgia rheumatica? |
Giant cell (temporal) arteritis |
|
|
Vasculitis usually in asian femoles > 40 years old |
Takayasu Arteritis |
|
|
Vasculitis: "Pulseless disease" (weak upper extremity pulses) |
Takayasu Arteritis |
|
|
Vasculitis: Fever, night sweat, arthritis, myalgia, skin nodules, ocular disturbance |
Takayasu arteritis |
|

With what vasculitis is this related?
|
Takayasu arteritis --Granulomatous thickening and narrowing of aortic arch and proximal great vessels |
|
|
Vasculitis: Young adult + Hepatitis B positive |
Polyarteritis nodosa |
|
|
Vasculitis: Typically involves renal and visceral vessels, not pulmonary arteries |
polyarteritis nodosa |
|
|
Vasculitis: Trasmural inflammation of the arterial wall with fibrinoid necrosis (Immune complex mediated) |
Polyarteritis nodosa |
|
|
Vasculitis: Different stages of inflammation may coexist in different vessels |
Polyarteritis nodosa |
|
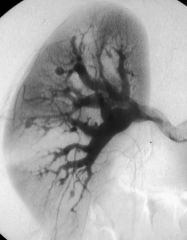
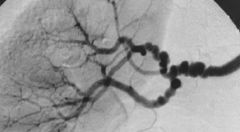
"String of Pearls" Vasculitis or fibromuscular dysplasia? |
Polyarteritis nodosa --Innumerable renal microaneurysm and spams |
|
|
Vasculitis: Asian children < 4 years old + conjunctival injection + rash + adenopathy |
Kawasaki disease Rash (polymorphous → desquamating) Adenopathy (cervical) |
|
|
Vasculitis: Oral mucositis + edema and erythema on hand/foot |
Kawasaki disease Strawberry tongue (oral mucositis) Hand-foot changes |
|
|
Vasculitis: May develop coronary artery aneurysm |
Kawasaki disease |
|
|
Vasculitis: Treat with high-dose corticosteroid prior to biopsy |
Giant cell (temporal) arteritis --prevents blindness |
|
|
Vasculitis: Treat with corticosteroids |
Takayasu arteritis |
|
|
Vasculitis: Tx: corticosteroids or cyclophosphamide |
Polyarteritis nodosa Granulomatosis with polyangiitis (Wegener) Microscopic polyangitis |
|
|
Vasculitis: Treat with IV immunoglobulin and aspirin |
Kawasaki |
|
|
Vasculitis: Treat with smoking cessation |
Buerger Disease (thromboangiitis obliterans) |
|
|
Vasculitis: Heavy smokers < 40 years |
Buerger Disease (thromboangiitis obliterans) |
|
|
Vasculitis: Intermittent claudication may lead to gangrene |
Buerger Disease (thromboangiitis obliterans) |
|
|
Raynaud phenomenon + autoamputation of digits + superficial nodular phlebitis |
Buerger Disease (thromboangiitis obliterans)
|
|
|
Vasculitis: Segmental thrombosing vasculitis |
Buerger Disease (thromboangiitis obliterans)
|
|
|
Vasculitis + Upper respiratory tract: perforation of nasal septum, chronic sinusitis, otitis media, mastoiditis |
Granulomatosis with polyangiitis (Wegener) |
|
|
Vasculitis + Lower respiratory tract: hemoptysis, cough, dyspnea |
Granulomatosis with polyangiitis (Wegener)
Microscopic Angiitis |
|
|
Vasculitis w/ Renal: hematuria, red cell cast |
Granulomatosis with polyangiitis (Wegener)
|
|
|
Chronic sinusitis + hemoptysis + red cell cast in urine |
Granulomatosis with polyangiitis (Wegener)
|
|
|
--Focal necrotizing vasculitis --Necrotizing granulomas in the lung and upper airway --Necrotizing glomerulonephritis |
Granulomatosis with polyangiitis (Wegener)
|
|
PR3-ANCA/c-ANCA Associated with what disease? |
Granulomatosis with polyangiitis (Wegener)
|
|
|
Vaculitis w/ CXR: large nodular densities |
Granulomatosis with polyangiitis (Wegener)
|
|
|
Necrotizing vasculitis involving lung, kidneys and skin without granulomas |
Microscopic polyangitis |
|
MPO-ANCA/p-ANCA Associated with what disease? |
Microscopic polyangitis
|
|
|
Vaculitis associated with Asthma, sinusitis, skin nodules or purpura, peripheral neuropathy (wrist drop/foot drop) |
Eosinophilic granulomatosis with polyangiitis (churg-strauss) |
|
|
Vasculitis associated with Paucini-immune glomerulonephritis |
Eosinophilic granulomatosis with polyangiitis(churg-strauss)
|
|
|
Vasculitis that can involve heart, GI, kidneys |
Eosinophilic granulomatosis with polyangiitis(churg-strauss)
|
|
|
Granulomatous + necrotizing vasculitis with eosinophils |
Eosinophilic granulomatosis with polyangiitis(churg-strauss)
|
|
MPO-ANCA/p-ANCA ↑IgE level Associated with what disease? |
Eosinophilic granulomatosis with polyangiitis(churg-strauss)
|
|
|
Chilhood vasculitis often follows upper respiratory infection |
Henoch-Schonlein purpura |
|
|
Palpable purpura on buttocks/legs + arthralgias + abdominal pain |
Henoch-Schonlein purpura
|
|
|
Vasculitis 2° to IgA immune complex deposition |
Henoch-Schonlein purpura
|
|
|
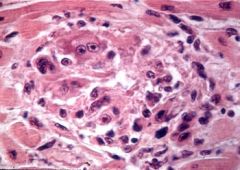
Arteriosclerosis hyperplastic type |
|
|
Vasculitis Associated with IgA nephropathy (Berger disease) |
Henoch-Schonlein purpura
|