![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
51 Cards in this Set
- Front
- Back
|
Dextrocardia |
Heart on the R hand side Due to abnormal heart looping Apex beat palpated in R 5th intercostal midclavicular line If isolated, can be severe; usually accompanied by other severe cardiac anomalies, such as single ventricle/ ventricular septal defect |
|
|
Situs invertus |
All organs are inverted i.e. liver and appendix are on the left side instead of the right side if heart is on the right side with other organs, you will still survive |
|
|
Where is apex beat usually palpated for? |
Left 5th intercostal mid-clavicular line **mitral valve auscultation |
|
|
Atrial septal defects (list them only) |
10% of congenital heart diseases are ASD's: 1. osteum secundum 2. endocardial cushion defect with osmium primium defect 3. sinus venosus defect 4. common atrium "tricolare biventriculare" |
|
|
Osteum secundum |
Atrial septal defect (ASD) Second hole where apoptosis occurs can get larger or can hop in another spot |
|
|
Endocardial cushion defect with osteum primium defect |
Atrial septal defect (ASD) Septum doesn't grow all the way to endocardial fusion mesoderm; osteum prim. not closing towards EC mesoderm |
|
|
Sinus venosus defect |
Atrial septal defect (ASD) Opening of superior vena cava; pulmonary veins come out from R atrium instead of L atrium. Surgery needed |
|
|
Common atrium |
"Cor tricolare biventriculare" Atrial septal defect (ASD) Rare; three chambered heart (cortriloculare biventriculare) = 3 chambers with 2 ventricles i.e.biventricle and thus one atrium |
|
|
Probe Patent Foramen Ovale |
1. 1 in 4 people have this (25% population) 2. Usually asymptomatic 3. If symptomatic, you have another cardiac defect 4. Common association with migraines 5. Probe between R and L atriums 6. doesn't close; analogy to VSD |
|
|
Premature closing of foramen ovale |
Before birth leads to death shortly after delivered Results in hypertrophy of the right side of the heart and under-development of the left side |
|
|
Ductus venosis |
Umbilical vein -->Highly o2 blood bypasses liver into R atrium |
|
|
Foramen ovale |
post natal "fossa ovales" R atrium bypasses R ventricle to R pulmonary trunk to lungs and goes straight to L atrium |
|
|
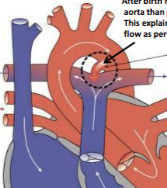
Ductus arteriosus |
Shunt system used to treat TRANSPOSITION OF GREAT VESSELS; blue baby Prostaglandins keep this open NSAID's keep this closed (PDA) Since some blood does go to pulmonary trunk; bypasses lungs and enters Aorta |
|
|
Persistent Truncus Arteriosus |
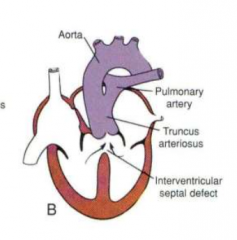
1:1000 live born infants
Failure to separate Truncus Arteriosus from persistent Conus Cordis (Conus cordis= cranial bc) 1 outflow tract. Failure to divide into ventral aorta, aortal sac, and pulmonary trunk No neural crest cell migration to membranous intraventicular septum ALWAYS: ventricular septum defect of membranous type. mixing of blood// no oxygenated blood cyanosis: blue baby
|
|
|
Transposition of Great Vessels |
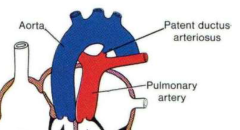
Overall annual incidence: 20-30 per 100,000 live births. Males >Females 3:1 No spiral septum; formed "straight down" aorticopulmonary septum (normally separates into 2 tubes spirally) Aorta -R ventricle/ Pulmonary trunk- L ventricle. Oxygenated blood stays in lungs and never goes to body Tx: Prostaglandins- opens Ductus arteriosus shunt system: Bypass of lungs and into Aorta from Pulmonary trunk (picture) |
|
|
Tetralogy of Fallot |
Anterior displacement of aorticopulmonary septum Tetralogy: 1. pulmonary stenosis (smaller pulmonary trunk) 2. overriding aorta (larger aorta) 3. Membranous type- ventricular septal defect 4. R ventricular hypertrophy caused by higher pressure on the R side (lots of blood trying to get through vessel) Cyanosis; blue baby poor oxygenation; decreased of blood to lung depending on stenosis Tx: surgical |
|
|
Ventricular septal wall defect - muscular type |
swiss cheese |
|
|
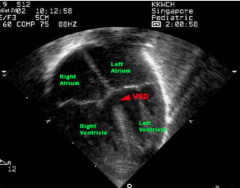
Ventricular septal wall defect-membranous type |
More common due to dual embryological origins in endocardial cushion mesoderm and aorticopulmonary septum 1. shunting of oxygenated blood from R ventricle to L ventricle 2. mixed blood to lungs = cyanosis blue babies 3. less oxygenated blood going through systemic circulation 4. pulmonary HTN 5. cardiac failure |
|
|
Common ventricle |
Ventricular septal wall defect Cor triculare biatrium 2 atriums, 1 ventricle 3 chambered heart no ventricular septum whatsoever |
|
|
VSD's summary |
membranous and muscular defects majority are small not as many as atrial septal defects usually membranous more common bc more complex due to dual embryological origin unlike probe patent foramen ovale, VSD's do close.*can be detected before birth |
|
|
Persistent Stapedial artery |
2nd Aortic Arch artery becomes spatial arteries which degenerates in adults and is normally are fetal only congenital vascular anomaly tinnitus carotid formation defects |
|
|
1st Aortic Arch Artery |
Symmetric R and L Maxillary arteries |
|
|
2nd Aortic Arch Artery |
Symmetric R and L Stapedial arteries (fetal only- role in carotid arteries) |
|
|
3rd Aortic Arch Artery |
Symmetric R and L 1. Carotid arteries long left, short right 2. Internal carotid arteries (distally) |
|
|
4th Aortic Arch Artery |
Asymmetric LEFT: majority of arch of aorta RIGHT: proximal R subclavian artery (7th intersegmental arteries--> distal segment) Subclavian artery has dual embryo origin |
|
|
5th Aortic Arch Artery |
no structures |
|
|
6th Aortic Arch artery |
Asymmetric RIGHT: R Pulmonary artery (majority of it) LEFT: L Pulmonary artery and Ductus Arteriosus (shunt from pulmonary artery to aorta) |
|
|
Pre-ductal Coarctation of Aorta |
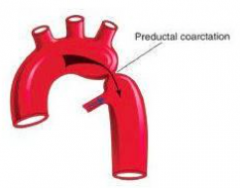
Constriction before it reaches Ductus Arteriosis No alternative route; baby dies |
|
|
Post-ductal Coarctation of Aorta** |
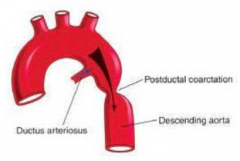
Constriction after it reaches Ductus Arteriosus Alternative route: COLLATERAL CIRCULATION: Left subclavian-->Internal thoracic artery-->Anterior intercostal artery (1-6) anastomoses with Posterior intercostal artery (3-9)--> Descending Aorta/Thoracic Aorta |
|
|
Double Aortic Arch |
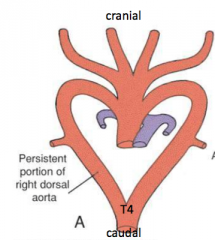
Cranial to T4 Two arches instead of one Right Dorsal Aorta (arch) not degenerating as it should normally
constriction of esophagus and trachea** Stridor &dysphagia |
|
|
5th intersegmental artery becomes? |
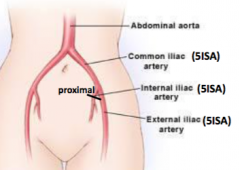
1. Common iliac artery 2. Internal iliac artery** 3. External iliac artery Proximal segment of internal iliac artery fuses with proximal umbilical arteries pre-natal |
|
|
Vitilline arteries become what 3 gut arteries? |
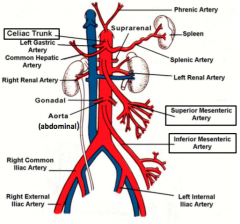
Vitilline aa. fuse with abdominal aorta (fusion caudal to T4 from dorsal aorta): 1. Coeiliac artery (T12- foregut) 2. Superior Mesenteric Artery (L1-midgut) 3. Inferior Mesenteric Artery (L3-hindgut) |
|
|
Umbilical arteries become? |
Retained: proximal umbilical arteries --> 1. distal segments of internal iliac arteries (because it fused with the proximal segments of internal iliac arteries) and 2. superior vesicle arteries Obliterated: distal umbilical arteries --> 3. medial umbilical ligaments (when we cut the cord) **umbilical veins obliterate after arteries |
|
|
Which veins drain into sinus venosus into the primitive R atrium? What kind of oxygenation do they provide? Origins? |
1. vitelline veins (yolk sac- deoxygentated) 2. umbilical veins (placenta - highly oxygenated) 3. cardinal veins (embryo body- deoxygenated) |
|
|
Ductus arteriosus becomes? |
Ligamentum arteriosus |
|
|
Cranial LEFT vitelline vein becomes? |
Hepatocardiac channel - Left Hepatic Vein |
|
|
Cranial RIGHT vitelline vein becomes? |
Hepatocardiac channel: 1. Right Hepatic vein 2. Hepatic portion of Inferior vena cava*** |
|
|
Central vitelline veins become? |
1. Hepatic sinusoids 2. Ductus venosus--> "ligamentum venosum" |
|
|
Caudal vitelline veins become? |
1. Portal vein (plexus around duodenum) 2. Splenic vein 3. Superior mesenteric vein 4. Inferior mesenteric vein |
|
|
Umbilical vein drains into? R or L? |
R umbilical vein obliterates by 2nd month
LEFT umbilical vein PERSISTS and drains into Ductus venosus (formed from central vitelline v) highest oxygenated blood |
|
|
Umbilical veins become? |
Left umb. v's closes shortly after umb. aa's close L umbilical vein obliterates--> ligamentum teres hepatic "round ligament of liver" |
|
|
Left Brachiocephalic vein formed how? When? |
How: Anastomoses between Left Anterior Cardinal vein and Right Anterior Cardinal vein When: Caudal part of Left Anterior Cardinal vein degenerates!! |
|
|
What happens to posterior cardinal veins? |
Majority degenerate!!!
Remaining portions= 1. Root of Azygos 2. Common iliac veins
5th Intersegmental artery becomes common iliac artery* |
|
|
What happens from the anastomoses of supra cardinal veins and sub cardinal veins? |
1. azygos and hemizygos veins 2. renal inferior vena cava |
|
|
Inferior vena cava formation |
1. hepatic- RIGHT vitelline v 2. prerenal- RIGHT subcardinal v 3. renal- anastomoses of sub and supra 4. postrenal- RIGHT supracardinal vein (left goes away) |
|
|
Absence of hepatic segment of IVC |
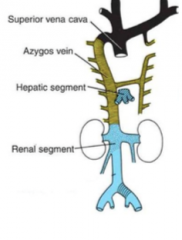
Failure of hepatic segment to form Blood from caudal parts of body drains via collateral circulation of azygos and hemiazygos to R atrium You won't die |
|
|
Double Inferior Vena Cava |
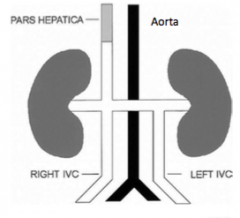
Inferior portion of left supra cardinal persists
Left IVC ends at left renal vein, and joins right IVC |
|
|
Superior Vena Cava formation |
Forms from anastomoses of RIGHT anterior cardinal vein and RIGHT COMMON cardinal vein |
|
|
Double SVC |
1. Persistence of Left Anterior Cardinal vein (which is supposed to degenerate for brachiocephalic vein to form!!) 2. Failure of brachiocephalic vein to form Result: left SVC drains blood from L side and dilates to accommodate the increased blood flow |
|
|
Left SVC in isolation |
1. Anastomoses of LEFT Anterior Cardinal v & LEFT COMMON cardinal vein 2. Obliteration of RIGHT common cardinal and RIGHT anterior cardinal vein ::: no R SVC is formed (this anastomosis is what normally makes the normal SVC)
Result: blood from R side drained by L SVC into R atrium via coronary sinus which enlargens due to increased blood flow |
|
|
Patent Ductus Arteriosus |
Occurs commonly in preterm infants. Can close spontaneously (by Day 3 in 60% of normal term neonates). Remainder are usually ligated and with little risk. Medications: NSAID's (ibuprofen) helps close PDA in premature babies only. NSAIDS block prostaglandin which keeps PDA open **rmr tx for transposition of great vessels |