![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
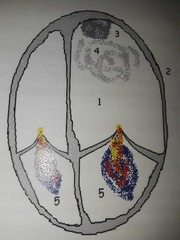
Dialated cardiomyopathy also known as congestive cardiomyopathy |
Most common of all CMOs, gross dilatation of the heart, multi chamber enlargement, decreased systolic and diastolic function. |
|
|
Causes of dialated CMO |
Idiopathic, genetic, infectious, ischemic heart disease, coronary artery disease, metabolic, peri-partum, post-partum, long standing systemic hypertension, endocrine disease agents used for chemotherapy, toxic levels from alcohol, lead or cocaine. |
|
|
Complications of dialated CMO |
Heart failure, decreased cardiac output, dysrythmias, regurgitant valves, ischemia, thrombus, infective endocarditis, pulmonary hypertension due to increased LA pressure, MR secondary to the annulus due to dilation. |
|
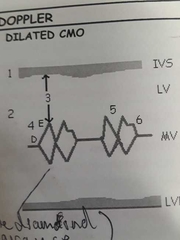
M mode for dialated CMO |
Thin walls and decreased function, increased chamber size, increased E point to septal separation, decreased D-E excursion, decreased excursion of mitral valve (double diamond), B notch due to increased LVEDP, decreased excursion of aortic root representing decreased cardiac output (not visible). |
|
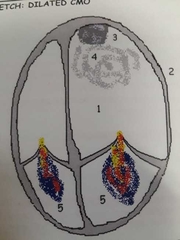
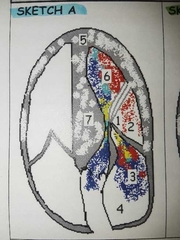
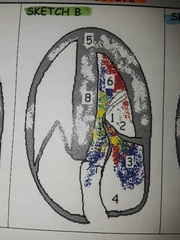
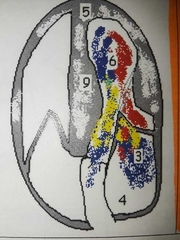
Dialated CMO Echo |
Thin walls, global decreased systolic function, decreased diastolic function, increased LV volume and mass, possible pericardial effusion, possible smoke and thrombus. Evaluate LV size, wall thickness, LV diastolic function, LV and RV systolic function, pulmonary artery systolic pressure by the RVSP or RAP, Volumes |
|
|
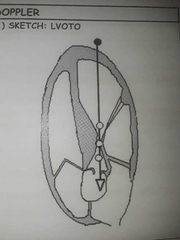
Dialated CMO doppler |
Regurgitation probable, evaluate diastolic function, reduced aortic ejection velocity, decreased stroke volume and cardiac output |
|
|
Hypertrophic CMO |
The leading cause of heart related sudden death in people under 30. Known for its hypertrophic, hyperdynamic, non-dialated LV. Sometimes, but not always associated with LVOTO. |
|
|
Etiology of Hypertrophic CMO |
Idiopathic, genetics, microscopic disorganization of myocardial fibers |
|
|
Symptoms of Hypertrophic CMO |
Dyspnea on exertion (difficulty breathing on exertion), Orthopnea (shortness of breath while lying down, paroxysmal nocturnal dyspnea (intermittent SOB at night), Chest pain especially during exercise, dysrythmias, fatigue, syncope (fainting), pulmonary edema. All of these are symptoms of decreased cardiac output. Patients with non-obstructive CMO may be asymptomatic. |
|
|
Complications of Hypertrophic CMO |
Endocarditis, Embolus due to LA thrombus, Heart failure, sudden death especially with exertion. |
|
|
Treatment for HCMO |
Beta blockers, calcium channel blockers, Anti-arythmics, septal myectomy, pacemaker controls AV node delay and contraction of the LV to decrease the LVOTO, ablation (injection of alcohol into coronary artery that feeds the IVS creating area of infarct) decreases LVOTO, Implantable defibrillator for high risk of cardiac death due to dysrythmias (electrical shock). |
|
|
Hypertrophic Non Obstructive Cardiomyopathy |
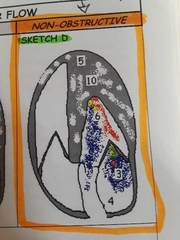
Apical hypertrophy (spade shape) or another form of hypertrophy that doesn't obstruct the LVOT. Common findings include MR, LA enlargement, brightened myocardium, small hyperdynamic LV. |
|
|
Hypertrophic obstructive CMO |
Hypertrophy that contributes to a LVOTO. (IHSS with asymmetric hypertrophy, HOCM with concentric hypertrophy, HOCM with midventricular hypertrophy) |
|
|
Provocabale Hypertrophic Obstructive Cardiomyopathy |
Involves LVOTO that is obvious only with exercise, drugs (amylnitrate) , or valsalva maneuver. |
|
IHSS or idiopathic hypertrophic subaortic stenosis |
a type of hypertrophic obstructive CMO, LVOTO due to Asymmetric Septal Hypertrophy (ASH) + Systolic Anterior Motion (SAM) of the mitral valve. Possible mitral valve Thickening, MACS, or prolapse. |
|
Hypertrophic obstructive cardiomyopathy with concentric hypertrophy |
LVOTO obstruction due to LV hypertrophy and Systolic Anterior Motion of the mitral valve. Possible mitral valve Thickening, MACS, or prolapse |
|
Hypertrophic obstructive cardiomyopathy with mid ventricular hypertrophy of the LV |
Typically SAM is not present, but a LVOTO is present |
|
|
Hypertrophic CMO M-mode |
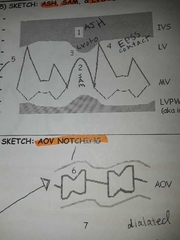
Small LV, hyperkinetic walls with abnormal thickness, SAM, possible MV prolapse, MV Thickening, LVOTO, Mitral EPSS contact, Aortic valve notching (partial Mid-systolic closure) due to sudden decrease in Cardiac output, LA enlargement |
|
|
Hypertrophic CMO doppler |
If LVOTO is present obtain peak velocity and pressure gradient by tracing waveform. Tracing will give peak velocity, max pg, mean pg. For quick PG use Bernoulli 4V squared. |
|
|
LVOTO versus MR doppler |
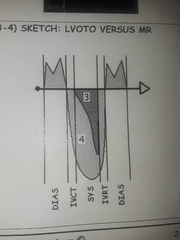
Parallel to flow is best, LVOTO is a late peaking dagger shaped jet during systole, while MR is wider with a greater peak velocity and encompasses the IVCT and IVRT. |
|
Restrictive/ Infiltrative Cardiomyopathy |
Least common CMO. Stiff rigid ventricular walls that impede diastolic filling. Heart failure is common. Resembles constrictive pericarditis (surrounds entire heart) however, this only affects the ventricles resulting in bi-atrial enlargement and bi ventricular hypertrophy |
|
|
Restrictive/Infiltrative CMO symptoms |
Excessive fatigue, swelling of lower extremities or abdomen, cough (with sarciodosis), SOB especially with exertion at night or supine. |
|
|
Restrictive/Infiltrative Treatment |
Biopsy, control symptoms for quality of life (diuretics, steroids, chemo), heart transplant possible. |
|
|
Types of restrictive/ Infiltrative cmo |
Amyloidosis: most common, multisystem disease deposits of amyloid protein, stiffening of the heart Sarcoidosis: inflammatory masses infiltrate organs Glycogen storage (Pompes): excessive Glycogen, enlarged heart. Hemochromatosis: iron overload, deposits in the myocytes Myocardial fibrosis: fibrotic tissue lines myocardium, local areas of necrosis
|
|
|
M-mode and Doppler for restrictive/Infiltrative |
Evaluate hypertrophy, function and chamber size. Evaluate diastolic function. Mitral inflow pattern big E small A , without respiratory changes |
|
|
Aortic PG and HCMO |
Non-obstructive: PG less than 30 at rest Obstructive: PG greater than or equal to 30 Provacable: PG less than 30 but obstruction occurs with exercise, maneuvers or drugs. |