![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
50 Cards in this Set
- Front
- Back
|
When was the 1st cardiopulmonary bypass done |
1953 |
|
|
Wht is the usual route for surgery of heart |
Median sternotomy |
|
|
Wht drug is the pt supposed to receive before CPB |
Heparin |
|
|
Wht is commonly used for arterial cannulation for CPB? Wht are the alternatives |
Femoral and axillary Axillary artery has less chance of thromboembolic phenomenon |
|
|
Wht is cannulated for venous drainage. Where is the cathether |
|
|
|
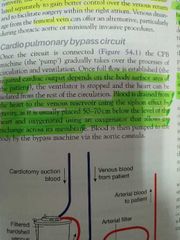
How is blood drained to the CPB |
|
|
|
Wht are myocardial protection methods, since coronary blood supply is cut off |
|
|
|
Wht is the arrest agent in cardioplegic solutions |
Potassium |
|
|
Advantages of cold and warm cardioplegics |

|
|
|
How long of ischaemia can the heart tolerate |
15 to 20 mins |
|
|
By how much does the metabolic rate of organ drops for every 7 degree drop in body temperature |
50 % |
|
|
what are the complications that can occur during CPB |
Difficulties can occur during
cannulation (aortic dissection or atrial injury), at the start of CPB (oxygenator failure) and at the end of CPB (coagulopathy) |
|
|
which surgeries can be done on a beating heart |
restricted to coronory artery bypass grafting (CABG) |
|
|
Which of the following is NOT a potential complication of cardiopulmonary bypass? A Pulmonary embolism. B Intestinal ischemia or infarction C Post-cardiotomy syndrome. D Neurological dysfunction. E Bleeding disorders |
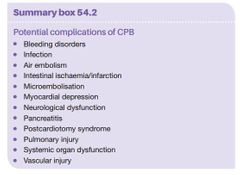
pulmonary embolism as pts are usually under the cover of heparin |
|
|
where do the coronary arteries arise from |
The coronary arteries are branches of the ascending aorta,arising from ostia in the aortic sinuses above the aortic valve,the right from the anterior sinus and the left from the left posterior sinus
|
|
|
to wt is the graft of the left coronary artery anastomosed to and why? which arteries are used for anastomosis |
The artery is inaccessible at its origin and therefore grafts are anastomosed to its branches, the left anterior descending artery (LAD) or anterior interventricular artery and obtuse/marginal (OM) branches of the circumflexartery.
|
|
|
what decides dominance |
The question of anatomical dominance is determined by the artery that supplies the posterior descending artery.
90% is the RCA |
|
|
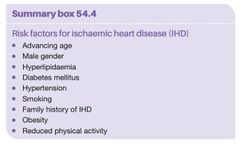
wht are the risk factors for ischaemic heart disease |
|
|
|
wht is the 1st stage of atherosclerosis |
The fatty streak. The first evidence of atherosclerosis can be found in children 10–14 years of age The streak consists of smooth muscle cells, which are filled with cholesterol, and foam cells. |
|
|
wht are the other stages of atherosclerosis |
● Fibrous plaque. A fbrous plaque consists of large numbers of smooth muscle cells, foam cells, and leukocytes. , it projects into vessels leading tolumen narrowing that
.● Complicated lesion. This occurs when the fibrous plaque ruptures provoking the formation of thrombus |
|
|
how is previous MI diagnosed in ECG |
Evidence of previous myocardial infarction (MI) is seen commonly, as Q waves and/or non-specific ST and T-wave changes |
|
|
what are the cariac enzymes used for diagnosis of ACS |
Standard enzyme measurement such as troponin, creatine kinase MB(CKMB) and lactate dehydrogenase (LDH) can aid diagnosis,as well as having prognostic implications
|
|
|
wht test is used for dx myocardial ischemia |
Exercise tolerance testing (ETT) is a valuable technique for assessing myocardial ischaemia
physiological response to exercise as measured by the percentage of the maximum predicted heart rate achieved |
|
|
what radionuclide studies are used for cardiac perfusion |
The main type of radionuclide study used is myocardial perfusion scanning using specific radioisotopes (such as thallium201) to assess the significance of coronary disease and the viability of the myocardium.
|
|
|
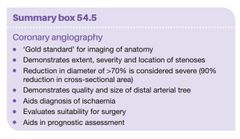
what is considered severe stenosis |
Any stenosis in an artery of >70% of the diameter (90% reduction of cross-sectional area) is considered ‘severe’
|
|
|
how do we predict who will benefit from revascularization |
flow measurement across a stenotic area, using techniques such as fractional flow reserve (FFR), has been effective in predicting patients who are likely to benefit from revascularization
|
|
|
coronary angiography summary |
|
|
|
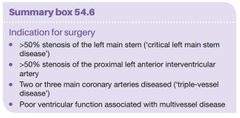
indications for surgery |
|
|
|
Wht is done to body temperature during heart surgery |
|
|
|
what is the difference in the way of timing PCI and CABG in treatment |
While the benefit from PCI in patients with non-ST segment elevation acute coronary syndrome(NSTE-ACS) is related to its early performance, the benefit from CABG is greatest when patients can undergo surgery after several days of medical stabilisation.
|
|
|
complications of MI |
Ventricular septal rupture Mitral valve papillary muscle necrosis causes acute mitral regurgitation Ventricular aneurysm |
|
|
how is ventricular septal rupture presented and treated |
Ventricular septal rupture typically presents3–7 days after infarction with pulmonary oedema, a pansystolic murmur and hemodynamic instability.
The diagnosis is usually confirmed with echocardiography. Repair is with a pericardial or artificial Dacron patch. |
|
|
how is Mitral valve papillary muscle necrosis treated |
Mitral valve papillary muscle necrosis causes acute mitral regurgitation, a pansystolic murmur and pulmonary oedema.
Diagnosis is made by echocardiography and right heart catheterization (showing large V waves). Mitral valve replacement is usually necessary, |
|
|
wht are the two scores used for cardiac risk assessment |
the EuroSCORE II and STS score
|
|
|
which graft is used most commonly and why? how do we increase the patency of the graft |
The long saphenous vein is the most common vein used as a conduit as it is straightforward to harvest, provides good length and is easy to handle lipid-lowering agents and antiplatelet agentssuch as low-dose aspirin can improve vein graft long-term |
|
|
wht is the conduit of choice for LAD |
The left internal mammary artery (LIMA), or internal thoracic artery, has become the conduit of choice for the LAD.
long-term patency rates of >98% have been reported, with improved long-term survival and fewer reoperations |
|
|
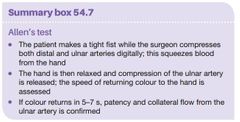
wht test should be performed for harvesting radial artery wht are the alternatives |
In assessing a patient in whom a radial artery harvest is planned, an Allen’s test should be performed.
Alternative arterial bypass grafts include the gastroepiploic artery and the inferior epigastric artery. |
|
|
how do we perform allen test |
|
|
|
wht is the most common arrhythmia post op? wht is the treatment |
The most common postoperative arrhythmia is sinus tachycardia, closely followed by atrial fibrillation (AF)
Treatment includes correction of potassium (>4.5 mmol/L), the use of β-blockers, amiodarone or digoxin and, if necessary, cardioversion. |
|
|
what is the treatment of Bradycardia |
temporary pacing via epicardial pacing wires inserted intraoperatively |
|
|
wht is the cause of poor cardiac output state post op |
depressed myocardial contractility
reduced preload increased afterload and a disturbance in heart rate or rhythm. Treatment is aimed at the underlying cause |
|
|
wht is to be done If low cardiac output persists despite inotropic support, |
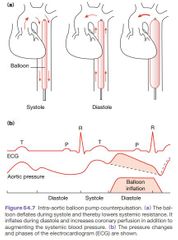
Mechanical support can be achieved using intra-aortic balloon pump (IABP), ventricular assist device(VAD) or extracorporeal membrane oxygenation (ECMO) |
|
|
how does IABP works |
|
|
|
wht is the difference between CPB and ECMO |
ECMO is another circulatory support device that is similar to CPB; however, ECMO can be established using venous-access only (called VV-ECMO) or venous and arterial access(VA-ECMO). |
|
|
incidence of wound infection in CABG |
0.5-2% |
|
|
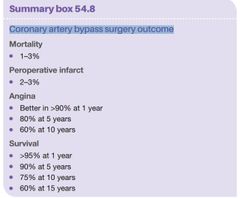
mortality from CABG |
1-3% |
|
|
Coronary artery bypass surgery outcome |
|
|
|
wht is Off-pump coronary artery surgery? advantages |
CABG without the use of CPB It offers the advantages that it avoids the physiological stress associated with CPB and, to some extent, the aortic manipulation that can lead to neurological injury through atherosclerotic embolization. |
|
|
wht devise is used to perform off pump coronary artery surgery disadvantage of OPCAB |
octopus the quality of anastomosis carried out on a beating heart and bloody field that can limit the surgeons vision |
|
|
wht incision is used for Minimally invasive direct coronary artery bypass (MIDCAB) surgery |
Through an anterior submammary incision
|