![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
categorise the types of breathing circuits? |
open: no boundary b/w circuit and atmosphere. e.g. wafting sevo near a child/old ether masks. non rebreathing: must have a one way valve separating reservoir from mask. e.g. air viva. (not air Viva is NOT a mapleson circuit. rebreathing: 2 types... absorption system: circle non absorption system: mapleson circuits. |
|
|
Draw a non rebreathing system - i.e. air viva system? |
2 one way valves. may have another reservoir on other side of bag. |
|
|
what are the mapleson circuits? what effects do they have on CO2 re breathing and PaCO2. |
they are all rebreathing system without Co2 absorbers. rate of FGF vs tidal volume will dictate if CO2 rebreathed. NOTE: just because pt rebreathes CO2 does NOT mean they will retain CO2/increase PaCO2. They all contain FGF, reservoir and adjustable pressure limitation (all except Mapleson E). |
|
|
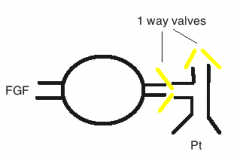
Draw the Mapleson A? what is code to remember this? |
A=APL valve at the Pt end. |
|
|
what is the FGF required in SV to prevent CO2 rebreathing? what is the key to this that makes it different to IPPV with mapleson A? |
SV FGF = 0.7 to 1 x MV. Key is that APL is OPEN in SV normal MV/kg = 100ml/kg roughly expi: first 30% is dead space (no CO2). towards end expi the bag fills, P > atmosphere and rest of expiratory gas in vented off. Expira pause the tubing is cleared of expired gas by FGF. inspiration the tube is filled of either FGF or expired dead space with no CO2. only need to replace MV or MV - the dead space (30%) so it 0.7 x MV. |
|
|
what is the FGF required in IPPV with mapleson A to prevent rebreathing CO2? why? |
IPPV FGF = 3 x MV. KEY is APL is CLOSED so that can provide +ve press vent. so on expiration expired gas is not vented off but is retained in tubing and reservoir bag, therefore need > FGF to clear it/dilute it in expiratory pause. |
|
|
draw the Mapleson B: what is its efficacy with FGF in SV and IPPV? What is it used for? |
B= both are at the pt end. very inefficient as FGF not at end where it can flush the circuit out, can only dilute it. FGF = 2-3 x MV for SV and IPPV. in past was resus circuit but is bad design for it as need high flow, O2 bottle empty quick. no use now |
|
|
Draw the Mapleson C? what is its FGF requirements and uses? |
C = CUT down B no difference to B except shorter limb. no advantage/no use. this is NOT a air viva as websites say as no 1 way valve. same FGF as B. |
|
|
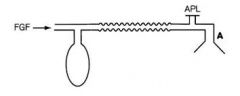
Draw the Mapleson D: how does the bain circuit compare to this? |
D is exactly same function as bain. Bain just has co-axial limb that delivers FGF to pt end. |
|
|
what FGF is required for bain circuit in SV? |
SV = 2 x MV. expiration all the expired gas goes past FGF outlet and as bag fills it is vented out open APL. expi pause: FGF flushes out the expired gas in tube. even if it doesn't flush it all, the majority of tidal vol will be new FGF, the last part of TV may contain CO2 but will be make up the dead space and not participate in respiration. |
|
|
what is FGF required in bain in IPPV? |
0.8-1 x MV - i.e. very efficient.. inspiration: at the start its all FGF and low pressure. as lungs reach end TV, pressure increases and the rest of reservoir bag is emptied out of the APL valve...as reservoir bag is mainly expired gas, most of the expired gas is vented off. so this relies on you over pressuring the bag and blowing it off... |
|
|
draw mapleson F: what is the the Ayre T piece? What is the Jackson reece modification? |
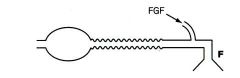
this is a mapleson F: ayres T piece (aka mapleson E) is exactly the same without the bag. adding the variable outlet bag is called jackson reece medication of ayre T piece and becomes a mapleson F..what is used for small kids at RCH... |
|
|
what is the FGF required of Mapleson F/jackson reece modification of ayres T piece. what important factor does the circuit have to have? |
SV is 2-3 x MV IPPV has many complex formula. in practice adjust FGF for bag feeling and capno trace. it must have expiratory limb with > volume than the TV |
|
|
what is the functional difference between the T piece and Bain circuit? what ages can they be used on? |
NOTHING! they are functionally the exact same thing. Can use either circuit on any age...just have to adjust the size of the bag and size of the tubing. in practice RCH use bain >30kg, T piece < 30kg. |
|
|
what are the advantages of the bain / T piece over circle circuit? |
Pros: light weight, easy to handle, adjustable APL in one hand (T piece), small dead space as small limb on T piece. minimal resistance as no valves, short tubing (esp good for neonates etc). can scavenge bain CONS: need high FGF. waste inhaltional agent, %, environment, can't scavenge T piece. no humidification (except HME) |
|
|
draw all the mapleson circuits: what is the memory aid for these? |
A to C = letter corresponds to what is at the Pt end: A = APL valve B = Both APL + FGF C = cut down B D = bain E/F = T piece |
|
|
Draw the standard circle system: why is the APL valve where it is? where is the vaporiser in this circuit? |
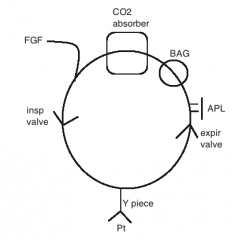
APL: after Pt and before FGF. don't want FGF coming into circuit and then blow off before getting to pt. ideally B4 CO2 so don't filter gas, use up soda lime and then discard the gas. Vapouriser: out of circuit = in the FGF. In circuit = after FGF before Pt. |
|
|
what is the difference b/w in circuit vaporiser (ICV) and out of circuit vaporiser (OCV)? |
OCV (normal type): calibrated (so exact % in gas leaving vaporiser no matter what gas flow through it), temp regulated, high resistance. ICV (old type): not calibrated (so % in gas leaving inversely proportional to gas flow), not temp regulated, low resistance. |
|
|
which type of ventilator will self titrate the patients depth of anaesthesia in spent vent mode? |
only the ICV can as its not calibrated...OCV does NOT. ICV: > MV as pt lightens = > movement of gas through circle => gas through vaporiser and gas returning to vaporiser already has volatile in it, so it gets more and more % in it with each pass. OCV: > flow through circle doesn't help, it just dilutes the set FGF with set % so pt will actually lighten up more... |