Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
95 Cards in this Set
- Front
- Back
|
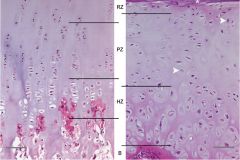
Bone anatomy
|

Diaphysis: parallel edges
Metaphysis: Fluted edges Epiphysis: between growth plate & articular surface |
|
|
Where is cancellous bone seen?
|
Epiphysis and Metaphysis ONLY
NOT in diaphysis |
|
|
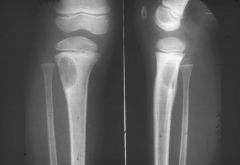
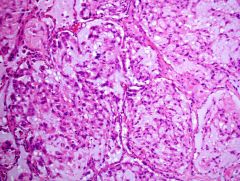
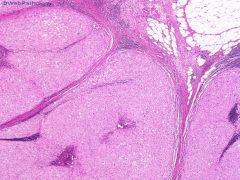
Tumor metaphysis of long bone of extremity (KNEE), in skeletally immature patient
|
Osteosarcoma
|
|
|
Osteosarcoma
age distribution? |
Bimodal
10-20 & 50+ |
|
|
20y.o. Caucasian with diaphyseal tumor
|
Ewing sarcoma
exclusively in whites |
|
|
Ewing sarcoma
Age distribution? |
Most < 20
But can occur at any age |
|
|
Age distribution for chondrosarcoma?
|
Steadily increases with age
|
|
|
Most common epiphyseal tumor in childhood?
|
Chondroblastoma
|
|
|
Malignant bone tumor by age:
<5? 5-15? >40? |
Metastatic neuroblastoma
OS or ES Met or myeloma |
|
|
T/F: Most bone tumors less than 6 cm are benign.
|
True
|
|
|
Radiologic calcifications suggest what type of tumor?
|
Cartilagenous
|
|
Firm bony lesion distal femur 20M
|

Osteochondroma
3 layersL perichondrium, cartilage, bone |
|
|
Osteochondroma imaging?
|

Sessile or pedunculated
Calcifications Continuity of marrow space to lesion |
|
|
Syndrome with multiple osteochondromas?
|
Multiple hereditary exostosis
AD Increased risk of chondrosarcoma (40% or 1% per year). |
|
|
Px in MHE patients that do develop chondrosarcoma?
|
Same as general population
|
|

|
Enchondroma
Hands & feet most common Benign cartilage, islands Radiolucent or mineralized |
|

Syndrome of multiple enchondromas?
|
Ollier disease
Usually unilateral Failure of enchondral ossification |
|

Syndrome of multiple enchondromas AND hemangiomas?
|
Maffucci Syndrome
Severe skeletal malformations High risk of other malignanies (ov, CNS, panc...) |
|

|

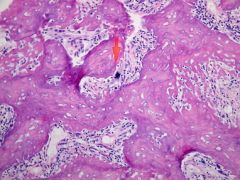
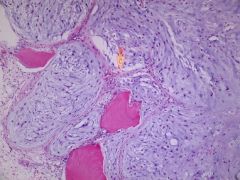
Periosteal chondroma
Prox humerus & femur most common ** SHARPLY MARGINATED from cortex (vs osteochondroma). See the cortex without infiltration by the lesion. Can look very ugly = need radiology not to call chondrosarc. |
|
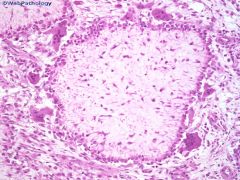
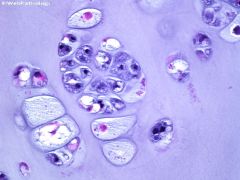
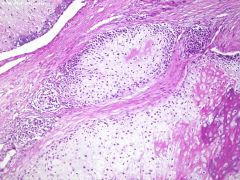
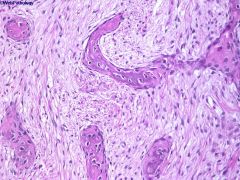
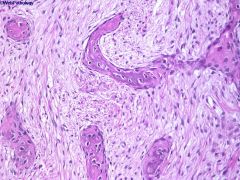
What is this called?
Imaging? |
CHICKEN WIRE CALCIFICATION
Chondroblastoma Imaging: small lytic lesions +- sclerotic rim ** Often has osteoclast-like giant cells. |
|
|
How to ID CB vs. GCT of bone?
|
Giant cell tumor of bone usually occurs in >20y.o. and does NOT have a sclerotic rim on imaging
|
|
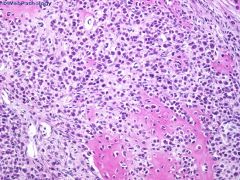
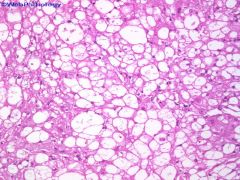
Epiphyseal lesion 20M
histologic features? treatment? |
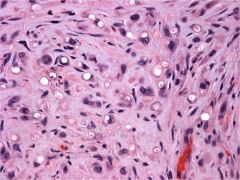
Chondroblastoma
-Epiphyseal - 10-30 year olds, m>f Biphasic lesion (cellular & matrix) Round nuclei with fine chromatin. LINEAR GROOVES COMMON. Abundant pink cytoplasm with retraction = fried egg. CHICKEN WIRE CALCIFICATION Osteoclast-like giant cells 25% recur > curettage |
|
|
What is the pink stuff in CB?
|
CHONDROID! NOT osteoid.
(Osteosarcomas DO NOT occur in the epiphysis) |
|
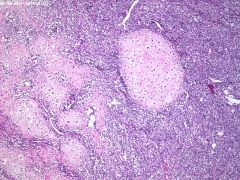
tibia or foot lesion in patient <30y
Radiology? Site? |
Chondromyxoid fibroma
METAPHYSEAL LESION Sharply marginated oval zone of rarefaction (looks grossly like yellow custard) |
|
|
Chondromyxoid fibroma
Treatment? px? |
Currettage
25% recur |
|

|
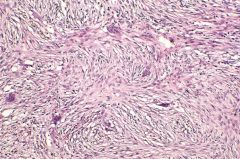
Chondromyxoid fibroma
MONOPHASIC lesion Spindled cells may see focal atypia osteoclast-like giant cells at edge CHUNKY calcification zonation (hypocellular in center, more cellular at periphery) Lobules of myxoid cartilage ZONATION |
|
|
How is the myxoid cartilage diff from hyaline cart?
|
Hyaline cartilage has LACUNAE; myxoid cartilage does not, the cells are just swimming in matrix
|
|
Knee lesion
|
Synovial chrondromatosis
mature cartilage with fibrous or synovial lining joints (hip, knee, TMJ...) |
|
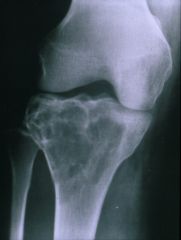
50M
Site? Imaging? |

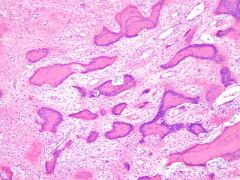
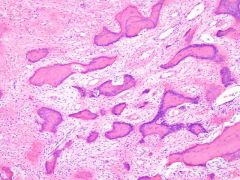
Chondrosarcoma
Axial skeleton; Pelvis (ileum), prox femus & humerus Metaphysis or diaphysis Imaging: Geographic lesion (geographic lesions usually benign except here); Fusiform expansion with cortical thickening and erosion; mineralization (non-homogeneous, ring&fleck) |
|
|
#1 px indicator in chondrosarcoma?
|
Histologic grade
|
|
|
Types of chondrosarcoma
|
Primary (arising in previously normal bone) (90%)
Secondary (arising in previous enchondroma / etc) Dedifferentiated (well-diff cartilagenous lesion, usu well-diff CS, + high grade noncartilagenous sarcoma, usu MFH) Periosteal Clear Cell (rare, low grade) Mesenchymal (rare, small round blue cell tumor + cartilage matrix) |
|
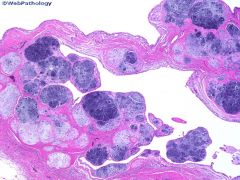
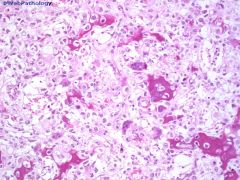
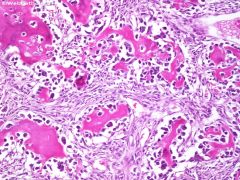
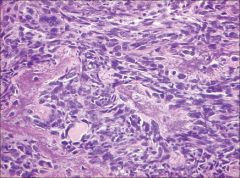
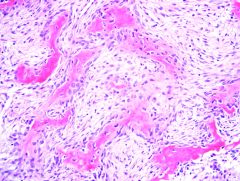
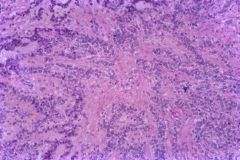
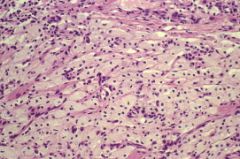
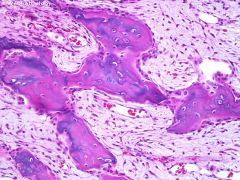
Tumor?
Histologic features? Treatment? |
Chondrosarcoma, grade 2.
Abundant hyaline cartilage Atypical chondrocytes (may be subtle) with binucleation Irregular lobules PERMEATION of bony trabeculae Can have osteoblasts build bone onto surface (reactive phenomenon, NOT osteosarc) TM: Surgery |
|
|
How to tell well-diff CS from enchondroma?
|
SITE!
CS rarely involves hands & feet, and enchondromas there can have atypical features CS is more cellular & permeates bone. More CYTOLOGIC atypia **Enchondromas (& OC) should STOP growing at bone maturity |
|
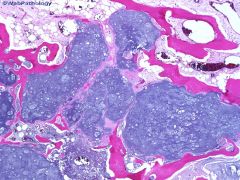
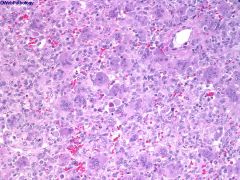
30y.o. spine lesion
|
Mesenchymal chondrosarcoma
small round blue cells + cartilage Poor long-term px |
|
|
#1 site of mesenchymal CS?
|
H&N (JAW!!!!)
spine, rib, ileum |
|
75M pelvis lesion
|
Dedifferentiated chondrosarcoma
BIPHASIC tumor Low-grade hyaline cartilage + high grade sarcoma (usu MFH) |
|
|
Dediff chondrosarc vs. chrondroblastic osteosarcoma
& why is this impt? |
The cheese analogy!
Dediff CS: swiss cheese. cheese + holes, no mixing. cartilage & high grade sarcoma do not mix; abrupt transition CB-OS: blue cheese. All mixed together. high grade cartilage & osteoid... Importance: Px Dediff CS 0% long term survival CB-OS: 80% |
|
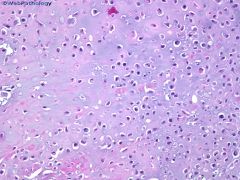
30M femur
tumor? bone site? |
Clear cell chondrosarcoma
EPIPHYSIS clear cells can have GIANT CELLS within tumor (only CS to do this) Good px |
|
|
Classic epiphyseal lesions?
|
giant cell tumor of bone
chondroblastoma clear cell chondrosarcoma Clear cell chondrosarcoma |
|
Teenage boy with severe nocturnal pain relieved by aspirin
Dx? Therapy? |
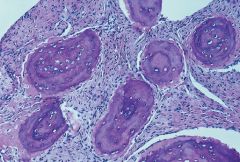
Osteoid osteoma
within cortex Imaging: discrete well-defined Mature bone, osteoblasts. Random anastomosis. fibrovascular stroma but no cartilage or elements <1cm Therapy = Ablation (RFA) |
|
20M... site?
|
SPINE! (transverse & spinous processes (not the vertebrae))
Osteoblastoma >1cm Mature bone, osteoid, lined by osteoblasts, "soldiers in a row", monomorphous |
|

Proximal humerus 17M.
buzzword? classic sites? |
Codman's triangle of Osteosarcoma
Due to periosteal elevation from expansion of intramedullary osteosarcoma. Usually a mixed osteoblastic and osteolytic lesion, with cortical destruction and extension into soft tissue Distal femur, prox humerus & tibia METAPHYSEAL lesion! |
|
|
presentation of osteosarcoma?
|
usually <30y.o. (if >40, suspect predisposing condition i.e. Paget's)
weeks to months of worsening pain, with or without palpable mass. 10% have fracture |
|
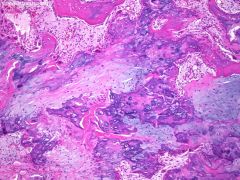
Type?
What is the thinnest osteoid called? |
Osteoblastic osteosarcoma
50% of conventional osteosarcoma MAKES OSTEOID Can be difficult to ID but is dense, pink, amorphous, curvilinear Thinnest osteoid is called FILIGREE. Looks like tendrils |
|
Dx?
matrix? |
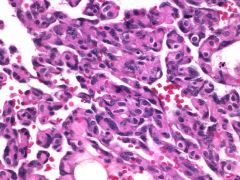
Chondroblastic osteosarcoma (25% of conventional OS)
Makes high-grade hyaline cartilage |
|
|
how to ID chondroblastic osteosarcoma vs. chondrosarcoma?
|
LOCATION
CS - EPIPHYSIS OS - METAPHYSIS Histology Dediff CS: usually low-grade cartilage with high-grade sarcoma. Separate. CB-OS: HG cart & HG osteoid; all mixed together. |
|
Type?
|
Fibroblastic osteosarcoma (25%)
High-grade spindle cells with minimal osseous formation and some cartilage. (looks like MFH but with some osteoid. can be subtle!) |
|
|
#1 px indicator in conventional osteosarcoma?
|
Response to pre-op chemo.
the histologic subtypes do NOT have differences in prognosis |
|
|
#1 metastatic site for conventional osteosarcoma?
|
LUNGS
..then bone. |
|
|
Genetic susceptibility to conventional osteosarcoma?
|
Hereditary retinoblastoma
(gene?) Li Fraumeni Syndrome (gene?) |
|
|
Gene for hered retinoblastoma?
Li Fraumeni? |
LOH @ 13q
TP53 mutations |
|
|
Clinical variants of osteosarcoma?
Morphologic variants? |
Jaw
Post-radiation Paget's Multifocal Morphologic: Well-diff intraosseous OS Telangiectatic Small cell OS |
|
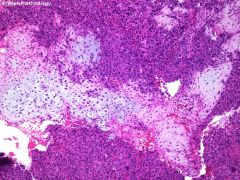
Variant of osteosarcoma?
|
Telangiectatic osteosarcoma
<4% OS Cystic spaces lined with benign appearing giant cells Malignant cells within cellular septa 2nd decade. Purely lytic lesion on imaging (convtroversy about this entity) |
|
Variant of osteosarcoma?
|
Small cell osteosarcoma
Small round blue cells with osteoid production. |
|
|
Major DDx of small cell osteosarcoma?
|
EWINGS!
Both small round blue cells Both can be CD99+ OS has osteoid but Ewings can have similar looking fibrin OS will NOT have t(11;22) |
|
|
What to think about in 60y.o. patient with osteosarcoma in the skull?
|
Paget's disease
poor px long bones, skull, vertebrae, pelvis |
|

25F limited knee flexion
|
Parosteal osteosarcoma
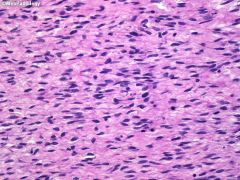
70% POSTERIOR distal femur WRAPAROUND pattern with time well-formed bony trabeculae in hypocellular stroma. looks like normal bone. stroma has minimal atypia. 50% have cartilage formation... Great px |
|
What it called when parosteal osteosarcoma recurs as high-grade sarcoma?
|
de-differentiated parosteal osteosarcoma
|
|

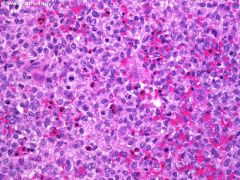
10y.o. M diaphyseal lesion, pain.
gross? |
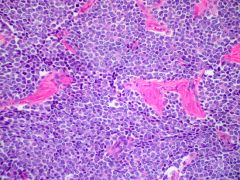
Ewing sarcoma
xray: moth-eaten appearance and ONION skinning of periosteum gross: fish flesh <20y small round blue cell tumor Homer Wright rosettes |
|
Ewing Sarcoma
IHC? genetics? what translocation imparts a more favorable px? |
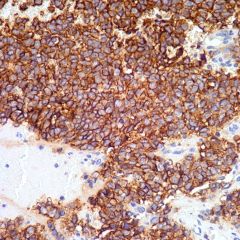
CD99 membranous staining (not specific)
can be cytokeratin+ cytoplasm with PAS+ granules t(11;22) EWS/FLI1 exon6-exon7 translocation is favorable |
|
|
DDx small round blue cell tumor in bone?
Xray appearance? |
Ewings/PNET
Primary lymphoma of bone Met rhabdomyosarcoma Met neuroblastoma Also: Osteomyelitis Small cell osteosarcoma Mesenchymal chondrosarcoma Multiple myeloma Histiocytosis X / LCH xray: moth-eaten appearance, permeative pattern Ewings may have soft tissue mass |
|
Asymptomatic metaphyseal lesion in a teenager
Dx? Imaging? Px? |

Non-ossifying fibroma (large), aka
Metaphyseal fibrous defect (when small), aka Fibroxanthoma Spindle cell proliferation STORIFORM pattern Benign giant cells, foamy histiocytes Increased mitotic figures No atypia Prob due to faulty ossification, not a true neoplasm Imaging: SOAP BUBBLE. metaphyseal lesion, eccentric, lytic, periph sclerosis Excellent px, with curettage |
|
|
Same as previous, except older age and in diaphysis or epiphysis?
|
Benign fibrous histiocytoma
|
|
Knee lesion with moth-eaten appearance on imaging, involving both the proximal tibia and distal femur
|
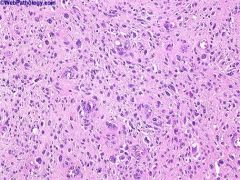
MFH
Marked pleomorphism, atypical mitoses. Spindled cells with storiform pattern. MNGCs. |
|
|
#1 site of mets in MFH?
|
Lungs
|
|
variant of osteosarcoma?
Clinical importance? |
Low-grade central OS, aka well-diff intraosseous OS
-Low-grade spindle cells with osteoid production -SUBTLE ATYPIA (enlarged, dark, some mits) these can DEDIFFERENTIATE (20%) to a higher grade, and then metastasize. |
|
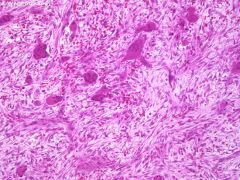
Destructive lesion distal femur
|
Fibrosarcoma
LOTS OF MITS HERRINGBONE pattern ~ to MFH (what is the difference??....) |
|
|
Name the fibrous, fibro-histiocytic, and fibro-osseous bone lesions.
|
FIBROUS
-Desmoplastic fibroma of bone -Fibrosarcoma FIBRO-HISTIOCYTIC -Metaphyseal fibrous defect -Non-ossifying fibroma -Benign fibrous histiocytoma -MFH FIBRO-OSSEOUS -Fibrous dysplasia -Osteo-fibrous dysplasia -FIbrous osteosarcoma |
|
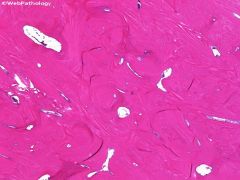
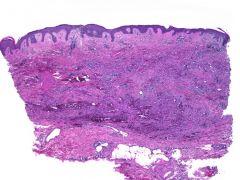
Jaw lesion, fibrous and osseous components WITHOUT osteoblastic rimming
VERY hard lesion Dx? Radiology? Forms? |
Fibrous dysplasia
Ground glass, non-destructive Monostotic vs polyostotic histology: Classic "C"shaped bony spicules in bland spindled stroma. See spindled cells dissecting the bone. NO OSTEOBLASTIC RIMMING |
|
Fibrous dysplasia
px? gene? |
Good px
GNAS1 gene (turns woven bone into lamellar bone) |
|
|
Name the syndrome:
polyostotic fibrous dysplasia skin pigmentation endocrine abnormalities |
McCune Albright Syndrome
|
|
|
Name the syndrome:
Polyostotic fibrous dysplasia Soft tissue myxomas |
Mazzabrand's syndrome
|
|
|
What are the other names for osteofibrous dysplasia?
|
Ossifying fibroma
Campanacci's disease |
|
5 year old boy
ANTERIOR TIBIA CORTICAL LESION |
Osteofibrous dysplasia
= ossifying fibroma = Campanacci's disease |
|
|
Osteofibrous dysplasia usually resolves but can progress to what tumor?
|
Adamantinoma
|
|
Anterior tibial lesion 30y M.
|
Adamantinoma
mostly in anterior tibia BIPHASIC turmor: epithelioid + spindled osteofibrous Some arise from osteofibrous dysplasia Can recur. 10% metastasize. |
|
Blue nodular plaques on HIV+ patient
Dx? IHC? |
Kaposi sarcoma.
-vascular prolif w/ jagged outlines -extrav RBCs IHC: HHV8+ |
|
Painful leg mass
|
Epithelioid hemangioendothelioma
rare Cords & nests of pink endothelial cells Don't make vessels, unlike hemangiomas Usually bland. CAN METASTASIZE |
|
Epithelioid hemangioendothelioma
IHC? Genetics? |
CD34, CD31
t(1;3) |
|
Leg mass
|
Angiosarcoma
|
|
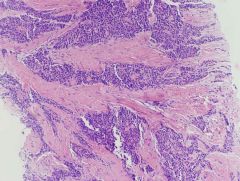
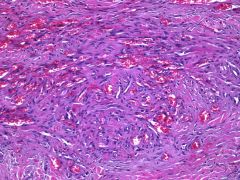
Sacral mass x 1 year in adult
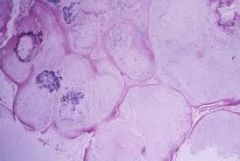
Histologic features? Buzzword for cell type? |
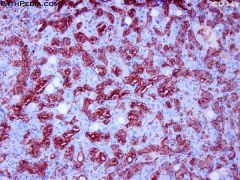
Chordoma
This is a malignant tumor! USUALLY WITH LARGE SOFT TISSUE EXTENSION Lobules of cells separated by fibrous septae Myxoid matrix Mild to moderate atypia PHYSALIFEROUS CELLS! (bubbly cytoplasm) |
|
What is important to know about the sampling of chordoma?
How can we differentiate between chondrosarcoma and adenocarcinoma based on IHC? |
Tranrectal biopsy is CONTRAINDICATED! Tumor is easily spread. Biopsy tract goes through peritoneum!! can seed (like ov ca!)
Chordoma: S100+/ck+/EMA+ CS: + / - / - Ad: - / + / + |
|
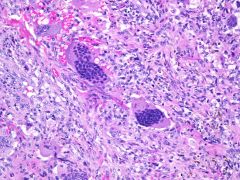
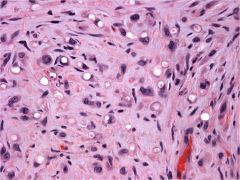
20F distal demur
Gross appearance? |
Giant cell tumor of bone
Usu 20-50y Benign but very locally aggressive & fast growing Mononuclear cells & giant cells (NUCLEI OF BOTH ARE THE SAME) Mononuclear cells have SCANT cytoplasm Grossly, red-black with hemorrhage |
|
GCT bone
Site? DDx? |
Ends of long bones (Epiphysis)
(Distal femur, prox tibia & humerus) DDx: Chondroblastoma (mononuclear cells have abundant eosinophilic cytoplasm; sclerotic rim; usu younger age <20) |
|
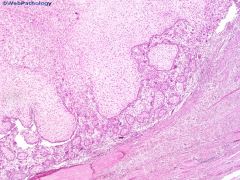
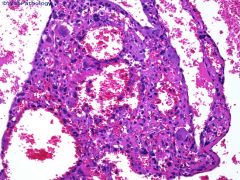
17Y with eccentric lytic lesion distal femur. Multiple fluid levels on imaging.
|
Aneurysmal bone cyst
Benign cystic lesion of bone usually <20y Primary: 70%. Bland fibroblasts and MNGCs, multilocular Secondary: occurs in GCT, OB, CB, FD Can look like telangiectatic OS |
|
|
Genetics of ABC?
|
Chrom 17
|
|
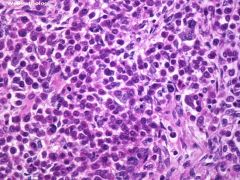
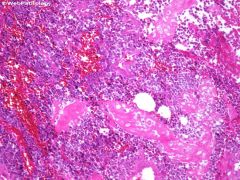
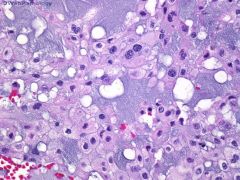
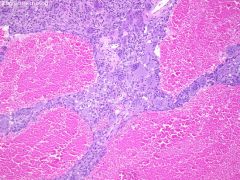
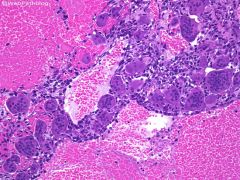
Skull lesion 20y.o.
|
Langerhans cell histiocytosis
Reniform nuclei Nuclear GROOVES Abundant eos Giant cells Mitoses |
|
|
LCH
IHC? EM? |
CD1a, S100, Langerin
Birbeck granules on EM |
|
Radiology: Bilateral symmetric sclerosis of the medullary cavity with epiphyseal SPARING
|
Erdheim Chester Disease
Infiltration of the skeleton and viscera by lipid-laden histiocytes Very rare Poor px |
|
|
Syndrome: Multifocal lytic bone lesions, exophthalmos, diabetes insipidus
|
Hand-Schuller-Christian Disease
Infants Multifocal LCH DI from infilt of pituitary |
|
|
often fatal disease of young children that is marked by proliferation of Langerhans cells and is characterized especially by fever, anemia, hepatosplenomegaly, and eczematous skin rash
|
Letterer-Siwe Disease
|
|
Radiolucent bone lesion in patient with hyperparathyroidism
|
Brown tumor of bone
NOT a neoplasm Osteoclastic giant cells and fibrogenic stroma (GCT of bone lacks fibrogenic stroma) |
|
|
Syndrome of multiple Brown tumors?
|
Osteitis fibrosa cystica
aka von recklinghausen disease of bone |
|
|
Causes of osteitis fibrosa cystica?
|
Advanced hyperparathyroidism
-PTH adenoma (80%) - Hereditary (10%) (MEN1) - PTH carcinoma - Renal osteodystrophy First affects bones of fingers, face, ribs, pelvis |
|
Finger lesion in 15y.o.
Dx? DDx? |
BPOP
aka Nora's lesion Rare. Hands & feet. Rapid growth. Often misdiagnosed. Cellular cartilage, bizarre fibroblasts, disorganized bone formation. LACK of atypia. DDx: Chondrosarcoma Fibrosarcoma LG Parosteal osteosarcoma Conventional Osteosarcoma |