Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
|
Blunt force injuries
|
-Injuries from impact with blunt object that tears, shears, and/or crushes tissue
-Most common type of trauma |
|
|
Examples of blunt force injuries
|
-Falls
-Blows/impacts with a blunt instrument such as a hammer, bat, fist, or pipe -Traffic related injuries |
|
|
Abrasion
|
-Scraped skin surface
-Loss of overlying epidermis -Produced by impact and friction with another surface -Look for patterns (ligature impression, belt buckle, bite mark) -Frequently accompanied with contusion (ex. bite mark) |
|
|
Contusion
|
-Bruise
-Hemorrhage in underlying soft tissue and organs -Overlying skin is intact -Color changes with time from resorption -Microscopic analysis best for aging injury -Can show a pattern (e.g., tire impression) |
|
|
Laceration
|
-Tear or disruption of tissue
-Incomplete separation of tissue (bridging tissue) across wound edges -Sharp force injury separates tissue between wound edges -Irregular wound edge |
|
|
Fracture
|
Break in bone continuity
|
|
|
Severity, extent, and appearance of the injury produced by blunt trauma is determined by...
|
-Nature of the weapon
-Amount of body surface over which the force is delivered -Amount of force delivered -Time over which the force is delivered -Region of body impacted |
|
|
How does the forensic pathologist addresses questions such as:
-How much force did the injury require? -What activities could be performed after sustaining the injury? -Age of injury? |
-FP characterizes the injury through description, notes/report, photos, histologic samples, and x-rays
-Radiology and neuropathology consultation to assist and medical record review |
|
|
Bite marks
|
-Contused abrasion
-Patterned injury -Abraded (scraped) skin with underlying hemorrhage -Swab for evidence |
|
|
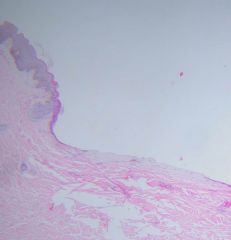
-Histopathology of bite mark
-Abraded epidermis with indentation of tissue -Hemorrhage in dermis |
|
|
Direction of force in a laceration
|
Undermining will be in direction of force
|
|
|
Basilar skull fractures
|
-Orbital plate fractures
-Battle's sign -Transverse ("Hinge") fracture -Ring fracture |
|
|
Orbital plate fractures
|
-Basilar skull fracture
-Dark discoloration of eyelids |
|
|
Battle's sign
|
Blood in ear canal or bruising behind ear
|
|
|
Transverse (hinge) fracture
|
-Where impact is from side to side from impact to chin where force was transmitted to base of skull via temporomandibular joints
-Or longitudinal fracture where impact is from front and/or back -Called "hinge" fracture because you can separate the two halves of the skull |
|
|
Epidural hemorrhage
|
-Blood collection between inner surface of skull and dura mater (membrane that covers the brain)
-"epi" means above (above dura mater but beneath skull) -Generally results from tear in middle meningeal artery |
|
|
Ring fracture
|
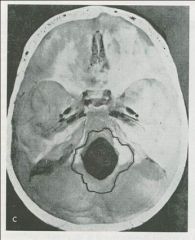
-Where force is being applied via the vertebral column
-Consistent with jumpers who land on their feet and the force break the base of their skull |
|
|
Motorcycle operator injuries
|
-Sternal and rib fractures
-Lacerations of pericardium and heart -Contusions and lacerations possible for all organs |
|
|
Aviation injuries
|

-Due to extremity applying pressure when impact occurs
-Will be significant to determine who the pilot was |
|
|
Injuries to organs
|
-Include contusions, hematomas, lacerations, and avulsions
-Cellular response is similar to skin, bone and soft tissue -Vital reaction or healing process is the same but there is variability in organ system response temporarily |
|
|
Stages of healing in abrasions
|
-Scab formation: occurs 2-18 hours post injury
-Epithelial regeneration: 30-72 hours -Subepidermal granulation: days 5-12 -Regression: begins at 12 days |
|
|
PMNs
|
-Polymorphonuclear leukocytes
-Inflammatory cells -Acute inflammation respond to injury -Followed by chronic inflammation |
|
|
Cells required for healing
|
-Blood vessels
-Glia -Fibrocytes |
|
|
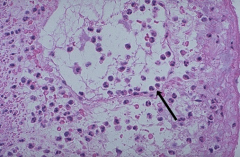
-Margination of PMNs
-Inflammatory cells move toward an injury (arrow) -Does not happen immediately, takes hours |
|
|
Age of injury will help you interpret...
|
-How old the injury is
-What time frame can be established -What does the investigation reveal and what is the reliability of that information? |
|
|
Blunt force injury - fatal child abuse
|
-Shaking baby syndrome
-Contusions are from subdural hemorrhage, since there should be no signs of external trauma -Age of injury and limitations on age determination is important in these deaths -If there is additional trauma such as fracture lines, trauma is not explained by shaking alone (head may have struck something) -Can also have trauma in the abdomen |
|
|
What to do during postmortem examination of transportation deaths
|
-Conduct examination of the occupant to determine if they were the driver or the passenger
-During postmortem examination, note injury patterns that need to be explained by scene reconstruction |
|
|
Seat belt injuries
|
-Abrasion on shoulder
-Contusion on abdomen from lap belt |
|
|
Injury patterns consistent with driver
|
-Scalp contusion on left side of head
-Rib fractures on left lateral aspect of chest |
|
|
Passenger injuries
|

-Angulated cuts "dicing" injuries to right side of face
-Shoulder belt abrasion on right side |
|
|
Motor vehicle glass injuries
|
-Minor vertical cuts on forehead from laminated glass on front windshield that prevents fragmentation
-Tempered glass on side and rear windows will fragment into small rectangular or cube shaped fragments and create dicing injuries -Correlate with position in vehicle |
|
|
Examination of the car occupant
|
-Pedal imprints on shoes may be helpful to determine the driver
-Will give insight into activity of driver just prior to collision: braking? -Black box (property of driver) will indicate speed, braking |
|
|
Manner of death in road traffic victims
|
-Accident is the convention
-Non-accidental deaths are unusual but do occur |
|
|
Characteristics of pedestrian deaths
|
-Should examine patterned injuries and location of impact sites
-Upright pedestrians usually have impact sites on legs, thighs, or buttocks -Victims lying in the road will not have impact sites, but fractured legs and broken skin |
|
|
Pattern injuries of the pedestrian
|
-Help determine direction of force
-Fracture points are measured to base of foot and compared to suspected vehicle -Proper reconstruction requires examination of shoes and their thickness as well -Fracture at primary impact site -Secondary impacts from impacts of windshields as well as other vehicles |
|
|
Brain injuries in a vehicle accident
|
-Diffuses axonal injury
-Intraparenchymal punctate hemorrhages -May occur with and without skull fractures -Acceleration/deceleration injuries |
|
|
Aortic injuries in vehicle accidents
|
Deceleration injuries produces a tear in the aorta. This usually happens just distal to the great vessels.
|
|
|
Summary
|
-Injury patterns from beatings, falls & traffic collisions provide insight into scene reconstruction and need to be correlated with scene findings
-Investigators and medical examiners need to work closely together for appropriate conclusions with regard to scene reconstruction |
|
|
Aging of contusions
|
-Color changes in resolution of a contusion
-Not always reliable as indicator of age of bruise -General color progression: red, purple, dark blue > green, dark yellow -Length of time for resolution may vary from several days to months -Consistent, reliable microscopic examination of contusions is not possible. Occasionally, microscopic examinations of contusions may lead to false assumptions |
|
|
Aging of lacerations
|
Difficult, unless there are clear signs of healing
|