Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
Patient's responsibility in control of asthma.
|
ADHERENCE
-medication must be taken as directed to be effective |
|
|
Asthma
|
Chronic inflammatory disorder of the airways
(Nuetrophils, Eosinophils, Lymphocytes infiltation) Epithelial cell injury and mass cell activation |
|
|
Mechanisms of Allergy in Asthma
|
Allergen exposure, lympocyte IL-4 production signals b cells to product IgE, activate mass cells, mass cells degranulation release mediators (Histamine, LTs, PGs, bradykinin), leads to inflammation in late phase.
|
|
|
Early Allergic Reaction
|
Decease FEV1 in minutes (lasts 1.5-2 hours)
Acute airway obstruction. |
|
|
Late Allergic Reaction
|
Another decrease in FEV1 about 2-8 h after exposure
Cytokines released from mast cells Lasts days to weeks. |
|
|
MOA of Beta2 agonists
|
Bind receptor, active adenylate cyclase increasing cAMP. Actives protein kinases affecting myosin light chain kinase and Ca++ dependent K+ channels... Bronchodilation
May also enhance mucociliary clearance, reduce mucosal edema, decrease mediator release, weak antiinflammatory NO effect on late response or on airway hyperresponsiveness. |
|
|
Beta2 agonists
|
Albuterol (onset within 5 min) last 3-6 hours
Salmeterol (onset 10-15 min) last 12 hours. Formoterol (onset 2-3 min) last 12 hours. All inhaled. |
|
|
SABA Indications
|
Best agent for exercise-induced asthma
Treatment of choice for mild intermittent asthma and acute exacerbation of asthma with systemic steroids COPD maintenace and exacerbations (often combined with anticholinergic agents) |
|
|
LOBA Indications
|
(Salmeterol, Formoterol)
Maintenace treatment of asthma, COPD, and EIA. Never use as monotherapy (add to ICS theapy) |
|
|
B2 Agoinists Adverse effects
|
CNS
Nervousness, irritability, insomnia Skeletal muscle tremor – ß2 manifestation Tolerance develops Heart – ß1 manifestation Palpitations, tachycardia, arrhythmias Paradoxical bronchospasm Regular or too frequent dosing |
|
|
Parasympathetic effect on bronchioles
|
Parasympathetic stimulation of muscarinic receptors – airway mostly M3 receptor
Increased cholinergic tone Increased bronial smooth muscle tone and mucus secretion |
|
|
Anticholinergics for Asthma
|
Ipratropium (Atrovent)
Tiotropium -once daily doing (Atrovent 4x/day) Combination albuterol/ipratropium. |
|
|
Anticholinergics Indications
|
FDA-approved for COPD
-may be better than B2 agonists. Non-FDA approved for asthma |
|
|
Methylxanthines
|
Theophyllin (caffeine, theobromine are natural alkaloids)
Low therapeutic index |
|
|
Methylxanthine effects
|
Pulmonary – theophylline > caffeine
Nonspecific phosphodiesterase inhibitor that increases intracellular cAMP Airway smooth muscle relaxation – Bronchodilation CNS effect – caffeine > theophylline Increased alertness, reduced fatigue Respiratory stimulant Nervousness, insomnia Cardiovascular effect Positive inotropic & chronotropic GI effects Increased gastric acid secretion Decreased LES pressure Renal effect – Weak diuretic Increased GFR Decreased tubular Na+ reabsorption Tolerance develops Improvement of diaphragmatic contractility May be important in COPD patients |
|
|
Theophylline Why not used
|
Less effective than B2 agonists
Metabolized by CYP450. Significant does-related side effects. >30 mcg/mL CNS stimulation & seizures |
|
|
Anti-Inflammatory Agents for Asthma
|
Corticosteroids
Mass cell stabilizers Leukotriene modifiers |
|
|
Effects of corticosteroids in asthma
|
Block late-phase reation
Reduce mucus secretion Increases B receptors |
|
|
Corticosteroids for Asthma
|
Fluticason (Flovent)
Triamcinole |
|
|
Combination drugs for Asthma
|
Fluticasone/Salmeterol (Advair) 1 inhal q12h
Budesonide/Formoterol (Symbicort) 2 inhal q12h. |
|
|
Cromolyn
|
Mast Cell Inhibitors
Not used very often mild potency anti-inflammatory agent, NOT a bronchodilator. |
|
|
Leukotrienes Overview
|
CYSTEINYL LTs – LT C4, D4 & E4
Formerly known as slow reacting substance of anaphylaxis (SRS-A) Very potent bronchoconstrictors & inflammatory mediators 1000 x > bronchospasm potency as histamine ACTIONS OF LTS Contract airway smooth muscle Increase vascular permeability (edema) Increase mucus secretions Decrease mucociliary clearance Recruit & activate eosinophils and basophils into airway Proliferation of smooth muscle |
|
|
Zileuton
|
5-lipooxygenase inhibitor
|
|
|
Montelukast and Zafirlukast
|
Cysteinyl LT receptor antagonists)
Montelukast (Singulair) Alternative, not preferred, treatment. Modest improvement in lung function as monotherapy. |
|
|
Omalizumab
|
Monoclonal Ab that binds IgE
-decrease free IgE in serum Allergy should be established by skin or blood test. Consider for severe persistent asthma (very expensive) |
|
|
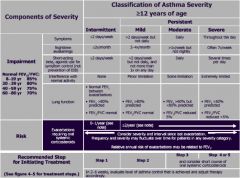
Asthma Classification
|
|
|
|
COPD
|
4th leading cause of death in US
Pharmacotherapy has not improved mortality, but does reduce symptoms and complications Smoking cessation and O2 most helpful to improve mortality. |
|
|
Therapy for COPD
|
Smoking cessation
Bronchodilator therapy Inhaled are preferred Methylxanthines Corticosteroids Treatment of Alpha-1 antitrypsin deficiency Influenza and pneumonia vaccination Oxygen supplementation Pulmonary rehabilitation Lung volume reduction surgery |
|
|
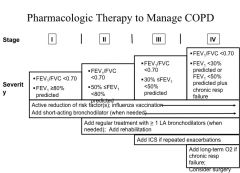
COPD Management
|
|