![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
93 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Name 3 causes of pharangitis |
Viral: EBV Bacteria: Group A streptococci, gonorrhoeae |
|
|
|
Is it ever OK to have a selfie stick? |
No! Jesus, how many times have we been through this!!? |
|
|
|
WHO Screening Guidelines PPH Question |
1. The condition being screened for should be an important health problem 2. The natural history of the condition should be well understood. 3. There should be a detectable early stage. 4. Treatment at an early stage should be of more benefit than at a later stage. 5. A suitable test should be devised for the early stage. 6. The test should be acceptable. 7. Adequate health service provision should be made for the extra clinical workload resulting from screening. 8. The risks, both physical & psychological, should be less than the benefits. 9. The costs should be balanced against the benefits. |
9 |
|
|
Name the structures in the ear that are likely to be damaged by: a. excessively loud sounds: b. large sustained changes in atmospheric pressure, like diving |
a. excessively loud sounds: hair cells of the cochlea, which are the actual mechanotransducers. b. large sustained changes in atmospheric pressure, like diving: tympanic membrane |
|
|
|
The natural History of glue ear (serous otitis media with effusion) is that of spontaneously remitting/relapsing disease (ie can resolve then relapse). What effect does this have on the PPV of a hearing test for detection of glue ear? (PPH QUESTION) |
The PPV will vary depending on whether the disease is in relapse or remission at the time of testing. This is why it may be necessary to test more than once if parents/teachers suspect a problem with the child's hearing. |
|
|
|
Which hearing tests indicate conductive deafness & nerve deafness respectively? |
Audiometry tests air conduction & bone conduction separately; the latter bypasses the middle ear. Clinically, the Rinne test using a tuning fork gives a rough and ready indication of a conduction problem. |
|
|
|
Name 3 common viruses associated with otitis media? |
RSV - Respiratory Syncytial Virus Parainfluenza Influenza |
|
|
|
What parts of the ear does a sound wave travel through until it stimulates a nervous response? |
External Auditory Meatus >Tympanic membrane >malleus > incus >stapes>oval window >scala vestibuli - vestibular membrane >vibrates into scala media/cochlear duct - >vibration of basilar membrane >stimulation Organ of Corti hair cells >action potential in cochlear branch of the vestibulocochlear nerve. |
|
|
|
Name 3 bacteria associated with upper respiratory tract infections (URTIs). |
25-50% Streptococcus pneumoniae <10% Penicillin R in Australia 15-30% Haemophilus influenzae mostly untypeable strains beta-lactamase positive~20% 3-20% Moraxella catarrhalis >90% beta-lactamase positive |
SMH ++- |
|
|
What are the common organisms (bacteria) causing otitis media? |
OM is usually from a viral infection, and a bacteria infection can follow. commonly: Haemophilus influenzae, Streptococcus pneumoniae
Less commonly: Streptococcus pyogenes, Staphlococcus aureus |
|
|
|
How do middle ear infections interfere with hearing? |
Fluid accumulation in the middle ear in association with infection impedes the normal movement of the tympanic membrane, the ossicles & the oval window in response to sound. All these structures vibrate less vigorously in the presence of fluid, causing hearing impairment. |
|
|
|
How does the surgical implantation of grommets in the eardrums of patients with a history of recurrent middle ear infections accompanied by chronic fluid accumulation relieve the problem? |
Chronic fluid accumulation in the middle ear is sometimes relieved by the insertion of grommets, which allow drainage of the fluid to the exterior. Usually, the grommet is pushed out as the eardrum heals. |
|
|
|
List 5 population-based strategies that are being used in Australia to prevent smoking. |
1. Smoke-free public places & workplaces 2. Public education 3. Tobacco taxes to increase price 4. Absence of tobacco promotion on TV, radio, & of tobacco sponsorship of sporting/arts/cultural events 5. Prohibition of tobacco sales to people<18 years 6. Compulsory information re: health effects of tobacco on tobacco packages & in any advertising material. |
|
|
|
What can medical practitioners do as individuals, that has been shown to be effective in getting their patients to stop smoking? |
Ascertain the smoking status of every patient routinely & tell all patients who smoke that giving up smoking is one of the most important things they can do for their health. |
|
|
|
What are the health benefits of quitting smoking? |
Immediate benefits 1. Former smokers live longer than continuing smokers regardless of the age they quit 2. Quitting results in a small increase in lung function & reverses the effect of the subsequent rate of decline which reverts to that of non-smokers. Long-term benefits 1. Excess mortality from heart disease due to smoking halves within 1 year of quitting 2. Excess risk of oral & oesophageal cancer halves within 5 years of quitting |
|
|
|
What role can doctors play to reduce smoking rates in Australia? |
Provide an exemplar role; Brief Intervention is effective; Support the individual wanting to quit; Use/seek opportunities - it's never too late; Advocacy within the medical profession & with patients; External advocacy in wider community; Support organisations - participate as a member Never be afraid to: ASK: about smoking status ADVISE: about quitting & helpful resources ASSIST: patients wishing to quit ARRANGE: appropriate referrals if required |
AAAA |
|
|
Where does the major airway narrowing in asthma occur? |
In the bronchioles. Other contributors = inflammation, congestion, oedema, hypertrophy of mucus glands & excessive mucus secretion. |
|
|
|
What structure collects acoustic sounds & funnels it to the eardrum? |
The outer ear. |
|
|
|
Explain the progressive reduction in airflow rate during expiration. Why is part of the flow-volume loop "Effort-independent"? |
During the 1st part of forced expiration, flow is effort-dependent because the airway resistance is 'relatively' constant so flow is dependent on force (m. effort). The resistance is 'relatively' constant because the EPP (Equal Pressure Point) is outside the chest. Flow becomes effort-independent (during expiration) when the EPP moves up-stream & enters the compliant part of the conducting airway - the airway will collapse if the pressure in the airway lumen is less than the surrounding pressure (intra-pleural pressure). Therefore - the greater the effort to generate flow, the greater the resistance to flow (due to airway compression) so there is no net increase in flow. |
|
|
|
What are: - FEV1 - FVC - TLC? |
FEV1 - Forced expiratory volume in 1 second - the max amount of air you can forcefully exhale in 1 second. FVC - Forced vital capacity - the max volume of gas that can be exhaled from full inhalation by exhaling as forcefully and rapidly as possible TLC - Total lung capacity - the volume in the lungs at maximum inflation |
|
|
|
Which changes in FEV1, FVC & TLC are typical of moderate asthma? |
Major effect = increased resistance which results in reduced airflow (reduced FEV1). Mild/moderate asthma - air trapping is relatively small compared to reduced flow (so FVC is reduced). NOTE: relatively wide range for 'N' in standard tables, so measured values are often within the N range. The TLC is N because the lung compliance is N (or slightly elevated due to 'stress relaxation). |
|
|
|
Which changes in FEV1, FVC & TLC are typical of restrictive disease? |
FEV1 = N because the airway resistance is N or reduced because compliant airways within the lung become smaller as the lung becomes smaller. FVC & TLC = reduced because the subject can't inflate the lung against the reduced lung compliance (increased elastance). |
|
|
|
Which changes in FEV1, FVC & TLC are typical of emphysema? |
Increased lung compliance (loss of elastance = inc TLC). Elastic recoil is important in generating the intra-luminal pressure. Airflow is reduced during a forced expiration (dec FEV1) because the increased compliance allows dynamic airway compression (intra-pleural pressure > intra-luminal pressure). The compression results in increased resistance & airway closure, trapping air in the lungs & increasing the residual volume. The increase in lung compliance results in an increased TLC. |
|
|
|
Which changes in FEV1, FVC & TLC are typical of upper airway obstruction such as tracheal stenosis? |
Increases airway resistance & reduces flow (FEV1). There is no early airway closure & the residual volume doesn't encroach on the FVC. The lung compliance is N so the TLC = N |
|
|
|
Tympanometry measures the effects on a low frequency tone as the pressure in the ear canal is varied. Which area/s of the ear does it provide information about? |
Outer & middle ear. |
|
|
|
Tympanogram with Eustachian tube dysfunction resulting in a negative middle ear pressure |
Tympanogram looks a normal shape, but is shifted on x axis with -200daPa middle ear pressure. See hint for picture. |
|
|
|
How many turns does a cochlea have? |
2 and a half. |
|
|
|
What are the 3 functions of the external ear? |
Protection Amplification Localisation |
|
|
|
Outline the physiological principles underpinning tympanometry. What information can be deduced from the results? |
Tympanometry measures compliance of the tympanic membrane. Liquid in the middle ear is incompressible & results in reduced compliance. Changes in pressure in the middle ear from blocked auditory tubes can be demonstrated, as the compliance peak occurs at an offset from atmospheric pressure. Increased compliance is found if the middle ear ossicles are dislocated. |
|
|
|
What are the 3 functions of the middle ear? |
Protection Impedance matching Pressure equalisation |
|
|
|
Where are the ossicles found? What are the ossicles? |
Middle ear Ossicles = three bones in the middle ear that are among the smallest bones in the human body. They serve to transmit sounds from the air to the fluid-filled labyrinth. Lateral to Medial (Outer to inner) Malleus Incus Stapes |
|
|
|
Name the elastic cartilage flap, attached to the entrance of the larynx that guards the opening between the vocal folds. |
Epiglottis |
|
|
|
Name the connection between the middle ear & nasopharynx which aerates & drains the middle ear. |
Eustachian tube. |
|
|
|
Which of the following V/Q ratios would result in a significant drop in arterial O2 saturation? a. V/Q = 20 b. V/Q = 20 and V/Q = 0.5 c. V/Q = 1.0 d. V/Q = 0.5 e. V/Q = 1.0 and V/Q = 20 |
c. V/Q = 0.5 |
|
|
|
During exercise, an increase in ventilation results in the removal of CO2 from the blood. This increase in ventilation will drive the bi-carbonate reaction: H+ + HCO₃- -> H₂CO₃ -> H₂O + CO₂ |
To the right - H₂O + CO₂ |
|
|
|
Describe atopy. |
Eczema, allergic rhinitis & asthma are all manifestations of atopy. A family history of the problem is common. Atopic symptoms have a higher incidence in childhood when compared to adulthood. |
|
|
|
When compared to eosinophilic asthma, neutrophilic asthma is: |
less responsive to steroids, its also less common. |
|
|
|
What are the characteristics of airways in asthma? |
Increased airway wall inflammation Increased predisposition to bronchospasm Increased mucous secretion NOT Increased smooth muscle hyperplasia |
|
|
|
What receptors do salbutamol act on to cause bronchodilation or bronchial smooth muscle? |
Beta 2 |
|
|
|
Name some drugs that cause bronchodilation. |
Ipratropium Terbutaline Salmeterol Salbutamol Note: ipratropium and other anticholinergics bind to Muscarinic (M3 subtype) receptors & cause bronchodilation. |
|
|
|
Name some drugs that may worsen asthma. |
Celecoxib Atenolol Ibuprofen Aspirin |
|
|
|
Within the alveoli, the partial pressure of O₂ (PaO₂) is reduced from that measured in the outside air (160mmHg) to approximately 105mmHg. List 3 events that contribute to the reduction in PaO₂. |
1. Early diffusion of O2 2. Humidification of air (water vapour pressure) 3. Increased presence of CO₂ |
|
|
|
Peripheral chemo-receptors are important in the control of ventilation. A decrease in PaO₂ < ___mmHg, or an increase in PaCO₂ > ___mmHg will be sensed by the peripheral chemo-receptors resulting in an increase in ventilation. |
A decrease in PaO₂ < 75mmHg, or an increase in PaCO₂ > 45mmHg will be sensed by the peripheral chemo-receptors resulting in an increase in ventilation. |
|
|
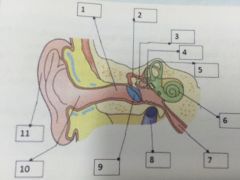
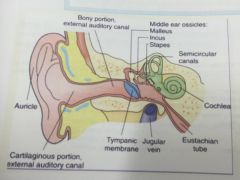
Name the parts of the ear in the diagram. |
|
|
|
|
A patient complains of left sided hearing loss. What do these results show? Rinne test: Left: Bone > Air (negative) Right: Air > Bone (positive) Weber test: Lateralises to left |
Patient suffers from Left conductive hearing loss. |
|
|
|
A patient complains of right sided hearing loss. What do these test results show? Rinne test: Left: Air > Bone (positive) Right: Air > Bone (positive) Weber test: Lateralises to left |
Patient suffers from right sensorineural hearing loss. |
|
|
|
List the types of added abnormal sounds that might be heard with a stethoscope when listening to the lungs. |
Crackles (or crepitations) Wheeze Rubs Squeaks Stridor |
|
|
|
Describe what whispering pecteriliquy is and what it might indicate if heard in a patient. |
Musical resonant sound heard when patient whispers; usually implies that the patient has consolidation of lung tissue. |
|
|
|
What is the pharmacokinetic difference between salbutamol & salmeterol? |
Both are beta 2 agonists. Pharmacokinetically: - Salbutamol is a fast onset agonist with a short half-life of around 3 hours. Used as a 'reliever' medication with rapid effect - Salmeterol is slow in onset with a half-life of 8-12 hours. Used as a 'preventer' medication, reducing the amount of salbutamol required in between times. |
|
|
|
What are the side effects experienced with salbutamol (SABA), especially when given by repeated nebuliser or intravenous infusion? |
As the systemic concentration of the drug increases, it has more potent beta receptor effects, including some beta 1 agonism. Thus it is similar to a sympathetic stimulation & results in tachycardia, ectopic beats & arrhythmias, flushing, tremor & anxiety. |
|
|
|
Where are the receptors for glucocorticoids located in cells? |
Like all steroid receptors, the receptors are located intracellularly. The fat soluble steroids enter the cell by passive diffusion through the cell membrane & binding of the steroid to the receptor results in a slow effect mediated by changes to DNA transcription & translation to make or inhibit new proteins. |
|
|
|
A patient complains of left sided hearing loss. What do these test results show? Rinne test: Left: Nil air or bone conducted sound Right: Air > Bone (positive) Weber test: Lateralises to right |
"Dead left ear" with profound left sensorineural hearing loss. |
|
|
|
What are the effects of glucocorticoids in treating asthma? |
In the case of glucocorticoids in the respiratory tract, their anti-inflammatory effects are mainly mediated by: - Inhibition of cytokines in the inflammatory cascade, particularly Th2 cytokines like IL-2 & IL-4 which promote IgE production - Inhibition of COX-2 up-regulation - Inhibition of histamine release from basophils |
|
|
|
Why do patients on inhaled steroids get oral thrush? |
Oral thrush is due to the local deposition of steroids in the back of the throat which causes local immune cell suppression & allows ubiquitous fungi like Candida to proliferate over a suppressed local immune response. |
|
|
|
What are the common side effects of prolonged oral glucocorticoid therapy? |
CVS: hypertension, accelerated atherosclerosis Neurological: insomnia, hyperphagia, agitation, euphoria, cataracts, benign intracranial hypertension GIT: gastric ulceration Endocrine: suppression of HPA axis, impaired glucose tolerance, Cushing's syndrome, polycystic ovarian syndrome, infertility Haematological: immune suppression, raise WBC count, poor wound healing Musculoskeletal: osteoporosis, impaired collagen synthesis, thin skin, proximal myopathy, easy bruising Metabolic: obesity & central fat deposition "buffalo hump", hyperlipidaemia, hypercholesterolaemia |
|
|
|
What is the MOA of aminophylline / theophylline? |
Phosphodiesterase inhibitors Phosphodiesterase (PDE) is an intracellular enzyme, inactivation leading to increased bronchodilation. |
|
|
|
What are the side effects of phosphodiesterase (PDE) inhibitors? E.g. aminophylline / theophylline |
Important PDE is in many organ's cells so it effects many systems & can cause tachycardia & arrhythmias, increased anxiety, tremor & hyperventilation & are a diuretic. |
|
|
|
What is seretide? |
Seretide is an inhaler that is a combination of 2 drugs. 1. The beta 2 salmeterol "Serevent" 2. The glucocorticoid fluticasone "Flixotide" They were originally 2 separate inhalers but have been combined as a single inhaler "Seretide" to improve compliance. It comes as an Acculhaler or a Metered Dose Inhaler (MDI) & there are various combinations of dosages available, depending on the patient age & asthma severity. It is taken twice daily as a 'preventer'. |
|
|
|
The laurinx is composed of 9 carlitiages. Where to these go from and too? |
C4-C6 |
|
|
|
What is the pravalnce of hearing loss? (I.e that it affects your life) |
Approx 1 in 5 people have a hearing loss that affects their life |
|
|
|
Where does the vagus nerve supply motor Para sympathetic innervation |
All organs from neck down to transverse colon Not the adrenal glands |
|
|
|
what are the definitions for the following: Otalgia Otorrhea Tinnitus |
Otalgia=pain Otorrhea=discharge Tinnitus=ringing |
|
|
|
What is prespecusis? |
The hearing loss assosiated with ageing (typically high frequency sensory hearing less) |
|
|
|
Why does carbon dioxide difuse faster than oxygen? |
(at atmospheric pressure) Carbon dioxide diffuses faster because CO₂ has much greater solubility than O₂ (carbon monoxide has even greater solubility) |
|
|
|
Name 3 consequences of lung surfactant? (DPPC is the chemical component of surfactant) |
1: reducation in colapse of smaller or underinflated alveoli (atelectasis) 2:more even distribution of ventilation amoing alveoli 3: increase in lung compliance (I.e greater pressure => inflation |
|
|
|
what is lung compliance |
how much the volume of lungs responds to change in pressures. So a compliant lung with have a greater volume even with a small change in pressure. Compliance goes down with fibrosis & goes up in the elderly. |
|
|
|
True or False: Surfactant INCREASES lung compliance meaning there is a REDUCTION in the work a patient or ventilation machine has to do to inflate the lungs |
true |
|
|
|
List 5 factors other than smoking that may increase the risk for a respiratory disease. |
Atopy / Rhinitis - Personal or family history Family history Birds GERD Alcohol, fits & aspiration pneumonitis Drug exposure - Amiodarone, methotrexate, nitrofurantoin, appetite suppressants TB exposure - personal or family history US travel - Phoenix Valley Fever Vaccinations or lack thereof Connective tissue disease Sleep related breathing disorders |
|
|
|
When is surfactant reliably produced in gestation? |
34 weeks |
|
|
|
What is the general term for fluid accumulation in the plural space (between the visceral and parietal pleura) |
plueral effusion |
|
|
|
How can the risk of oral thrush be reduced when taking inhaled steroids? |
Using a spacer reduces this complication as the particles are shot into a canister & then inhaled over several breaths, rather than being forcibly shot into the back of the mouth & accumulating on the mucosa. Washing out the mouth after dosing is also recommended. |
|
|
|
What level does the trachea biforcate? What is this called? |
Biforcarion at Carina, T7 (middle of sternum. The mucosa of the carina is highly sensitive & violent coughing is triggered when a foreign object makes contact |
|
|
|
what is the difference & clinical significance between the left and right primary bronchus |
The left is longer less vertical. The Right is wider, shorter, & more vertical and is more susceptible to lodgment of an inhaled foreign objec |
|
|
|
Bronchioles (air passages <1mm diam) have no mucus producing cells, so how are airbound debris cleared from here? |
respiratory macrophages (resisdent) |
|
|
|
What is atalectasis? |
Failure of part of the lungs to expand. The transpulmonary pressure keeps the lungs from atalectasis. As does the surfactant |
|
|
|
Name the volumes, yellow, pink, blue, & brown and the approximate ml in a normal male |
upload pic |
|
|
|
Define Vital Capacity. VC is the sum of which lung volumes? can you measure it with spirometry? |
VC= maximum expired after a maximum inspiratory effort VC= TV + IRV +ERV the only thing spirometry cant measure is residual volume (and thus total lung capacity also) |
|
|
|
Functional residual capacity is the volume of air left in lungs after normal tidal expirationFRC=RV+ERV. What would an average male & Female FRC be? |
FRC (av male)=2400 ml FRC (av female) = 1800 ml Remember expiratory reserve volume and residual volume are both the same In males (1200 each) |
|
|
|
what is inspiratory capacity? |
Inspiratory Capacity= max inspired air possible after normal expiration IC=TV+iRV |
|
|
|
with respect to lung function tests, obstructing lung disease will result in what? |
someone with Obstructive pulmonary disease will have a reduction in FEV1 |
|
|
|
name 4 hallmarks of asthma |
1. Intermittent & reversible airway obstruction 2. Chronic bronchial inflammation (w eosinophils) 3. Bronchial smooth muscle cell hypertrophy & hyperactivity 4. Increased mucus secretion |
|
|
|
The maximum expired volume, after maximum inspiration is called what? |
vital capacity |
|
|
|
What is the V/Q at the apex (top) of the lung, compared to the V/Q at the base? |
V/Q will be higher at the top (>0) and lower at the bottom (<0)."PCO₂ is to the base of the lung, as PO₂ at the apex" |
|
|
|
The affinity of oxygen to Hb is increased by reducing CO₂ in blood. what is this effect called? |
The Bohr effect refers to the CO₂ in blood effecting the oxygen affinity to Hb. |
|
|
|
what is carbonmonoxide (CO) so dangerous? |
its has a MUCH higher affinity to Hb than oxygen, so will quickly bind to and saturate Hb, and it shifts the O₂ disassociation curve to the left, making it harder to unload oxygen in the periphery. |
|
|
|
the lower the oxygen saturation, the more CO₂ can get taken up in the blood |
The haldine effect |
|
|
|
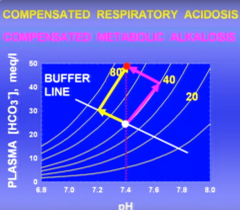
What are the two main causes of RESPIRATORY acidosis? |
Respiratory acidosis is caused by an increase in PCO₂; and the two main causes of this are alveolar hypoventilation and ventilation perfusion inequality |
|
|
|
why could someone at high altitude experience respiratory alkalosis? |
The lower O₂ stimulates the chemoreceptors to increase ventilation rate (hyperventilation), which inturn causes them to blow off CO₂ |
|
|
|
give a practical example of the inverse relationship between alveolar ventilation & PCO₂? |
if you double alveolar ventilation ,then PCO₂ falls from 40 (normal) to 20, |
|
|
|
Repiratory alkalosis/acidosis is caused by a decrese/increase in PCO₂. What is metabolic alkalosis/acidosis caused by? |
metabolic alkalosis/acidosis is caused by an increase/decrease in bicarbonate HCO₃. An decrease in HCO₃ could be casued by an increase in Ketoacids (i.e in DM) or an increase in Lactic acid (e.g following hypoxia, perhaps from a surgery) |
|
|
|
how does the body compensate for metabolic acidosis? |
increased H+ concentration in blood stimulates the periferal chemoreceptors which increase ventilation rate |
|
|
|
What will be the result of: loss of gastric acid, such as pyloric stenosis (baby has a block at end of stomach and vomit all the time). or too many Alkalotic drugs (i.e tums). |
Metabolic Alkalosis. This this case the chemo receptors dont really react much to the high pH, |
|
|
|
what is the relevance of ficks law to respiratory? V (gas)=(A/T)·D·∆P V= vol of gas going thru a slice A=area of slice T=thickness D=diffusion constant ∆P=partial pressure gradient |
ficks law states that the diffusion through a sheet is inversely proportional to a thickness of a sheet. So diffusion into tissues is effected by the increase in the thickness! also the D for CO₂ is vastly greater than for O₂, so it deals with the increased thickness better! |
|