![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
562 Cards in this Set
- Front
- Back
|
Levothyroxine |
-Hypothryoid drug -T4 drug that gets deiodinized to Liothyronine (T3), the active form -Activated nuclear receptors, leading to gene expression with RNA formation and protein synthesis -Max effect seen after 6-8 WEEKS of therapy -Drug of choice for thyroid hormone replacement therapy -Stable and low cost -Long t1/2 (7days) |
|
|
What are the drugs used for hypothyroidism? |
-Levothyroxine (T4): hypothrydoism, lowers TSH -Liothyronine (T3): Used for MYXEDEMA COMA & PRE-COMA (injection) 'hypothyroidism' bc it is more potent and since the person is comatose, their MBR is decreased, drug will last longer. Concomitant artificial rewarming contraindicated. -Dessicated thyroid (pork): Not FDA-approved, lowers TSH |
|
|
What are some adverse effects of supplying thyroid hormone? |
-Overdose leads to thyrotoxicosis -Angina or MI usually in older patients |
|
|
Liothyronine (T3) |
-Drug used for hypothryoidism -Best used for short-term suppression of TSH -Higher cost, relatively shorter t1/2 (24hours) -Can lead to cardiotoxicity |
|
|
What are the drugs that belong to the thiamide class? |
-All anti-thryoid drugs -Methimazole (MMI), Propylthiouracil (PTU, preferred drug in pregnancy and thyrotoxicosis) & Carbimazole (not available in USA) -Block de novo thyroid hormone synthesis within 1-2 hours after administration -Have no effect on release of preformed hormone from the thyroid gland |
|
|
What are the 3 classes of drugs we use to treat hyperthyroidism? |
Thioamides (Mehimazole (MMI), Propylthiouracil (PTU), and Carbimazole) Iodides (KI, NaI) Radioactive Iodine (131 I) |
|
|
Propylthiouracil (PTU) |
Preferred in 1st trimester of pregnancy and thyroid crisis (high doses) -Prevents hormone synthesis by inhibiting thyroid peroxidase-catalyzed reactions and blocking iodine organification -Blocks coupling of iodotyrosines -Inhibits peripheral deiodination (deiodinase D1) of T4 to T3 |
|
|
Methimazole (MMI) |
-Preferred drug for hyperthyroidism, once daily oral dosing -10X more potent than PTU, similar mechanism of action as PTU but DOES NOT EFFECTIVELY BLOCK DEIODINASE D1 (does not decr. synthesis) -Decreases the degree of hyperthyroidism in prep for subtotal thyroidectomy or radioactive iodine therapy -Used when thyroidectomy is contraindicated |
|
|
What are the pharmacokinetics of PTU and MMI? |
Slow onset of observable effects, 3-4 weeks before stores of T4 are depleted
|
|
|
What are the side effects of PTU and MMI? |
-Pruritic maculopapular rash (common);edema -Hepatitis (PTU-black box warning) -Agranulocytosis (rare, but serious), usually reversible upon drug withdrawal -Incr. chances of thyroid hyperplasia with long-term use |
|
|
Iodides (NaI, KI): Pharmacological action and clinical use |
-Inhibits synthesis and release of T3 and T4 -Decrease size and vascularity of thyroid gland -Clinical use: before thyroid surgery, decr. vascularity of gland -Treatment of hyperthyroidism --> thyroid storm (short term) --> improvement quite rapid (2-5 days)
|
|
|
What was used to prevent thyroid gland destruction by radioactive iodine in nuclear war/accident? |
Iodides (NaI, KI) |
|
|
Adverse reactions to Iodides? |
-Acneiform rash -Swollen salivary glands, mucous membrane ulcerations -Chronic use in pregnancy can cause fetal goiter |
|
|
Radioactive Iodine (131 I) mechanism of action |
-Administered as a single dose, orally -Produces ionizing radiation that damages thyroid gland (131 I is concentrated in thyroid cells) -Therapeutic effect depends on emission of beta rays w/ a short penetration range of 0.4-2mm and an effective half-life of 5 days -beta rays destroys the thyroid gland with little damage to surrounding tissue -Used to treat thyrotoxicosis |
|
|
Radioactive Iodine: indications |
-Radioactive iodide uptake test to evaluate thyroid function -Thyrotoxicosis: multinodular hyperthyroidism and toxic adenomas -Therapeutic effects take about 1-3 months |
|
|
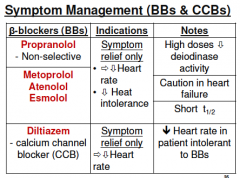
Symptom management of hyperthyroid effects with beta blockers and calcium channel blockers |
|
|
|
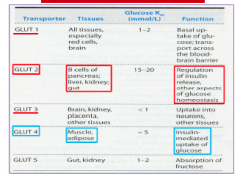
Where do you find the specific Glucose transporters? |
|
|
|
Which GLUT transporter do you find on beta cells of the pancreas? |
GLUT2
|
|
|
Which GLUT transporters do you find in almost all tissues? |
GLUT1: Regulate basal uptake of glucose; transport across the BBB -Found in all tissues, esp. red cells and brain -Necessary to sustain tissues at low energy |
|
|
Which glucose transporters are insulin-mediated for uptake into muscle and adipose tissue? |
GLUT4 |
|
|
Pharmacokinetics of insulin |
-Half life is 5 minutes -Degraded by Hepatic glutathione insulin dehydrogenase ***(805) and kidneys |
|
|
What are adverse effects of insulin? |
-Hypoglycemia (too much insulin): hunger, sweating, tachycardia, confusion, coma, ad convulsions can occur -Hypersensitivity with local reactions may occur; anaphylaxis is rare (glycosylation is protection against the immune system) -Lipodystrophy may occur at site of injection |
|
|
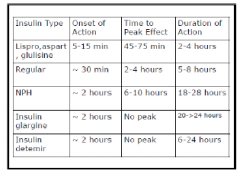
What are the short-acting regular insulin used? |
Insulin R --> Humulin R -Given BEFORE they eat (around 30 minutes before, lasts 5-8 hours) |
|
|
What are the rapid acting insulin analogs? |
Aspart, lispro, Glulisine -Given if eating <30 minutes, has an onset of 5-15 minutes and lasts 3-4 hours -It is rapidly metabolized and excreted |
|
|
Are the the intermediate acting insulins? |
NPH or Lente insulin -Onset is 60-180 minutes (1-3 hours) and lasts about 16-24 hours
Can also give a mixture of NPH and regular insulin which has an onset of ~30 minutes and lasts 16-24 hours |
|
|
What is the long-acting insulin? |
Ultralente insulin (basal, no peak) -Onset is 240 to 360 minutes (4-6 hours) and lasts 24-48 hours |
|
|
What are the basal insulins? |
Glargine and Detemir -Onset is 60 to 120 minutes (1-2 hours), lasts around 24 hours with NO PEAK |
|
|
Insulin types and duration of action |
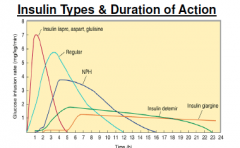
Note: Regular insulin has a slower onset, decr. peak and increased area under the curve (hence, greater length of effect) -Insuulin detemir and insulin glargine have no real peak |
|
|
Insulin and Synthetic Analogues |
|
|
|
Oral Hypoglycemic agents for DM2 |
-Insulin secretagogues (insulinotropics): sulfonylureas, meglitinides, DPP-IV -Insulin sensitizers: biguanides (metformin), Thiazolidinediones -Drugs that slows the absorption of starches: A-glucosidase inhibitors (Acarbose) |
|
|
Insulin secretagogues (insulinotropics) |
-Act directly or indirectly to stimulate pancreas to produce more insulin -Useful for patients with DM2 who cannot be managed on diet alone |
|
|
Insulin sensitizers |
Decrease blood glucose without increased insulin release -i.e. improve target cell response to insulin -Biguanides (decr. hepatic glucose production) -Thiazolidinediones (bind PPAR in muscle) |
|
|
Sulfonylureas mechanism of action |
Stimulates the release of insulin from pancreatic beta cells by binding to SUR and blocking the ATP-dependent K+ channels. Reduces K+ efflux leading to beta cell depolarization, calcium influx and secretion of insulin -May also incr. the Sn of peripheral tissues (muscle and fat) to insulin -Sulfonamide antibiotics can cause hypoglycemia **Person must have functional beta cells |
|
|
1st and 2nd generation sulfonylureas |
1st generation: Tolbutamide, Tolazamide, Acetohexamide 2nd generation: Glyburide, Glimepiride, Glipizide, Gliclazide |
|
|
Tolbutamide |
-1st gen. sulfonylurea -Dose duration 6-10 hrs -Inactived by LIVER through oxidation to carboxytolbutamide, excreted by the kidney -*** May give FP test for proteinuria |
|
|
Acetohexamide |
-1st gen. sulfonylurea -Dose duration 10-20 hrs -Metabolites formed by hydroxylation in liver (L-hydroxyhexamide is most active) |
|
|
Tolazamide |
-1st gen. sulfonylurea -Metabolized by the liver to 6 compounds, 3 of which have hypoglycaemic activity and are excreted by the kidney |
|
|
Glyburide and Glipizide |
-2nd gen. sulfonylurea -Dose duration 12-24 hours -These compounds are metabolized by the liver, partially excreted into bile, and the remainder excreted by the kidney |
|
|
Which drugs have opposite effects to sulfonylureas? |
Diazoxide and Milodoxil - Open K+ channels
|
|
|
Which drugs antagonize sulfonylurea actions?
|
Thiazide diuretics, estrogens, or any agents that inhibit insulin release or antagonize peripheral action
|
|
|
Which drugs potentiate the hypoglycaemic effect caused by sulfonylureas? |
-Sulfonamides -Beta-blockers -Alcohol -MAO inhbitors -Phenylbutazone -Bishydroxycoumarin -All lower blood sugar, enhance effects |
|
|
What do we use to treat gestational diabetes? |
Regular insulin |
|
|
Side effects of Tolbutamide? |
-Minimal anti-diuretic effect (the other agents have mild diuretic effects) -Reported incr. in cardiovascular mortality** (skin disorders, hypothyroid) |
|
|
Which insulinotropic is a non-sulfonylurea oral hypoglycaemic agent? |
Meglitinides |
|
|
What kind of drug is Repaglinide? |
Insulinotropic: stimulates insulin secretion by pancreatic beta cells -Fast acting, short duration and may be administered before meals from 30 min. right up to meal time (sulfonylureas take 30 min.) -Same mechanism as sulfonylureas Side effects: generally minimal (hyperglycaemia, and hypoglycaemia) -Recently contra-indicated in patients taking GEMFIBROZIL due to risk of severe/prolonged hypoglycemia -Can also occur with clarithromycin, itraconazole, ketoconazole, MAOis -Due to CYP2C8 and CYP3A4 interactions |
|
|
Metformin |
Biguanide -Indicated for use in DM2 -Several proposed mechanism of action: incr liver, muscle and fat cell sensitivity to insulin, incr. peripheral glucose uptake and utilization, incr. muscle glycogen synthesis, decr. hepatic glucose output -Particularly useful in ppl with REFRACTORY OBESITY -Dec. a number of cardiac RFs (Phenformin: association with lactic acidosis & no longer available) |
|
|
Side effects of metformin |
-Common: GI disturbances (nausea, diarrhea, flatulence) -LACTIC ACIDOSIS (rare): where clearance is reduced, i.e. renal or hepatic impairment -No sig risk of hypoglycaemia (does not stimulate insulin secretion) -Avoid in patients with alcohol base, severe hepatic impairment, and severe CHF -Co-administered with sulfonylurea (decr. HB1Ac values by 1-2%) |
|
|
What are the 2 thiazolidinediones? |
Rosiglitazone and pioglitazone ("glitazones" are the 1st drugs developed to target insulin resistance) |
|
|
Rosiglitazone and Pioglitazone mechanism of action |
Affect FA metabolism by binding to PPAR -Ligand-activated TFs (rosiglitazone - GLUT4) -Decr. blood glucose levels by improving target cell response to insulin Rosiglitazone: alters the FA metabolism so that they do not compete with glucose for oxidative metabolism -Leads to incr. sensitivity of TISSUES to insulin by recruiting GLUT4 to the cell surface (incr. uptake and suppressed hepatic glucose output) |
|
|
Therapeutic uses of Thiazolidinediones |
-DM2 treatment with inadequate control of hyperglycemia -NOT USED FOR DM1 -Use of Troglitazone in UK and USA was stopped due to potential hepatotoxicity |
|
|
What is required for prescribing Rosiglitazone and Pioglitazone? |
Has strong warnings and requires hepatic function tests before initiating therapy and continuing every 2-6 months |
|
|
What are the incretin hormones? |
GLP1(glucagon-like peptide 1) and GIP (glucose-dependent insulinotropic polypeptide) -Major incretin peptides that affect glucose metabolism |
|
|
What is a major advantage of GLP1? |
Restores beta cell function and promotes beta cell differentiation -Also increases insulin biosynthesis |
|
|
What are the GLP-1 analogs? |
Exenatide (synthetic) and exendin-4
|
|
|
Exendin-4 |
GLP1 analog -39AA peptide in the salivary secretions of Gila monster, PROTEASE RESISTANT -Incr. glucose dependent insulin secretion -Decr. elevated glucagon secretion and slows gastric emptying -Improve glycemic control by decr. fasting and postprandial glucose concentrations in DM2
|
|
|
Side effects of Exenatide or Exendin4 |
Can be administered twice daily, alone or with metformin, a sulfonylurea, or both --> significantly decreases HbA1c -Can cause GI disturbances: nausea, vomiting, diarrhea -Can also cause hypoglycaemia, when taken in conjunction with a sulfonylurea |
|
|
Liraglutide |
Injectable, long-acting synthetic GLP-1 analog with 97% homology to GLP-1 -Has a prolonged half life, once daily dosing -Acts by binding to the GLP1 receptor and increasing insulin secretion and decr. glucagon release -Results in reduced HbA1c (from 0.8 to 1.5%) and weight loss (nominal to 3.2kg) |
|
|
DDP4 inhibitors |
Sitagliptin -Blocks DDP4, a cell surface peptidase that cleaves a wide range of proteins and peptides -Incr. endogenous GLP1 and GIP --> Incr. insulin and decr. glucagon secretion --> better glycemic control -Adjunct to monotherapy to diet and exercise -May be used in combo with metformin or a Thiazolidinedione (TZD) -Not used in those with DM1 |
|
|
What are the side effects of Sitagliptin? |
Respiratory tract infection, nasopharyngitis (cold symptoms) and headache |
|
|
What is the intestinal disaccharide inhibitor? |
Acarbose: -Alpha-glucosidase inhibitor -Taken before meals, low dose delays and high dose inhibits carb absorption -Effective adjunct to sulfonylurea or insulin treatment
|
|
|
What are some examples of combined treatments for DM2? |
-Sulfonylurea+biguanide (glyburide and metformin = Glucovanec) -Sulfonylurea+insulin augmentation (at HS) -Sulfonylurea with Acarbose |
|
|
Which drug prevents renal glucose reabsorption? |
Canagliflozin: -Modest HbA1c reduction, weight loss, decr. BP (long term CVD risk reduction?) -Adverse effects: Hypotension, hyperkalemia, impaired renal function, UTI, incr. bone loss and incr LDL-C -May cause hypoglycaemia with concomitant use of insulin or insulin secretagoguges |
|
|
Which injectable synthetic anti-hyperglycemic drug is an analog of amylin? |
Pramlintide -Modulates postprandial glucose levels and is approved for preprandial use in person with DM1 AND DM2 -Adjunct to insulin in patients not achieving target postprandial blood sugar levels -Suppresses glucagon release via undetermined mechanisms, delays gastric emptying, and has CNS-mediated anorectic effect |
|
|
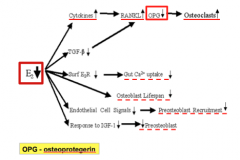
Over-expression of what drives increased expression, survival and function of osteoclasts? What does this lead to? |
RANKL --> Osteoporosis |
|
|
What are the anti-resorptive agents for osteoporosis? |
-Bisphosphonates -Calcitonin -Estrogen/HRT -Selective estrogen receptor modulators : Raloxifene -Tibolone (not available in USA) |
|
|
What are the bone building agents used for osteoporosis? |
PTH and Teriparatide |
|
|
What are the drugs with complex mechanisms used to treat osteoporosis? |
VitD+analogs, Denosumab, Strontium ranelate |
|
|
What are the bisphophonates? |
Anti-resorptive agents: (-DRONATES) -Alendronate -Clodronate -Etidronate -Ibandronate -Risedronate -Pamidronate -Zoledronic acid |
|
|
What is the mechanism of action of bisphosphonates? |
Inhibit bone resorption by attaching to bony surfaces undergoing ACTIVE resorption --> inhibit osteoclastic recruitment onto bone surface --> inhibit action of osteoclasts +induce apoptosis of osteoclasts -Leads to incr. BMD and reduced fracture risk (may incr. BMD by 2-8%) -Interfere w/ osteoclastic intracellular biochemical pathways --> inhibit farnesyl diphosphate synthase -Non-nitrogen containing bisphosphonates are metabolized to toxic analogues of ATP |
|
|
When are bisphosphonates indicated? |
-Prevention and treatment of osteoporosis in postmenopausal women -incr. bone mass in men w/ osteoporosis -Tx glucocorticoid-induced osteoporosis in men and women receiving glucocorticoids -Treatment of Paget's disease of bone in men and women |
|
|
What are some important adverse effects of bisphosphonates? |
-Most common: Acid reflux -Hypocalcemia and hypophosphatemia -Osteonecrosis of the jaw * (Others: abdominal pain, dyspepsia, musculoskeletal pain, cramps (recent FDA warning), esophageal ulcer, IV BP may induce visual disturbances) |
|
|
What is the mechanism of action of Calcitonin? |
-Released when calcium levels in blood are high -Binds to osteoclastis and inhibits bone resorption -Promotes renal excretion of Ca, Na, Phosphate, Mg, and K by decr. tubular reabsorption --> acts on osteoclasts |
|
|
What are some adverse effects of nasal spray calcitonin? |
-Rhinitis -Irritation of nasal mucosa (withdraw if ulceration occurs) -Epistaxis, sinusitis, back pain, arthralgia, and headache |
|
|
What are some adverse effects of injection (IM/SQ) calcitonin? |
-Nausea (10%), flushing (2-5%), headache -Skin test prior to initiating therapy -Supplement Ca2+ and Vit D if dietary intake not enough |
|
|
Osteoclastic apoptosis is regulated by what? What effects would deficiency of this have? |
Estrogen -Estrogen def. leads to longer-living osteoclats and incr. bone resorption -In resp. to increased bone resorption, there is incr. bone formation and a high-turnover state develops which leads to bone loss, and perforation of the trabecular plates
|
|
|
Pathophysiology of estrogen deficiency |
|
|
|
FDA has approved estrogen/hormone replacement therapy for: |
-Prevention of osteoporosis -Treatment of moderate/severe vasomotor symptoms of menopause -Treatment of moderate/severe symptoms of vulvar and vaginal atrophy associated with menopause -Consider TOPICAL preps to treat vaginal probs rather than oral (+bisphosphonates for the osteoporosis of menopause) |
|
|
Which selective estrogen receptor modulators (SERMs) do we use for osteoporosis? |
-Raloxifen (tissue-selective activity that acts as an estrogen agonist on bone, and antagonist on breast and uterus) -Tamoxifen -Bazedoxifene (not approved in USA, stops growth of breast cancer cells) |
|
|
When is Raloxifene used? |
-Prevention and treatment of osteoporosis in POSTmenopausal women -Adverse effects: Hot flashes, DVT, leg cramps, sm. incr. in risk of fatal stroke |
|
|
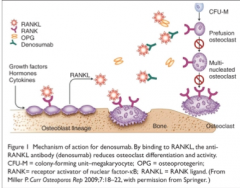
Which RANKL inhibitor has been approved for the treatment of post-menopausal osteoporosis? |
Denosumab -Suppresses bone resorption+secondarily, bone formation --> reduces the risk of vertebral and non-vertebral fractures w/ comparable effectiveness to the potent bisphosphonates |
|
|
Denosumab mechanism of action |
|
|
|
What are the adverse effects and disadvantages of Denosumab? |
-Immunosuppression (UTI+URIs), cataracts, constipation, rashes, joint pain -May be implicated in incr. risk of osteonecrosis of the jaw following tooth extraction or oral surgical procedures (similar to Bps) -Expensive! ($2000/yr+other fees - more expensive than BP) |
|
|
What are the VitD metabolite analogs used for osteoporosis? |
Cholecalciferol, ergocalciferol, calcitrol (+ doxercalciferol, paricalcitrol, calcipotriene) -Acts by incr. gene transcription at the VitD Receptor -Incr. Ca+ intestinal absorption, bone mineralization, renal Ca2+ and phosphate reabsorption -Decr. PTH promotes innate immunity and inhibits adaptive immunity |
|
|
Cholecalciferol (VitD3) mechanism of action and effects |
-Osteoblasts have receptors for Calcitrol (1,25 dihydro-VitD3) -Incr. activity of both osteoblasts and clasts -Incr. osteocytic osteolysis (remodelling) -Incr. mineralization through incr intestinal Ca2+ absorption -Feedback action of 1,25-OH2-D represses gene for PTH synthesis |
|
|
What are adverse effects of Vit D toxicity? |
-Hypercalcemia -Kidney stones -Excessive renal Ca2+ excretion -Calcification of soft tissues -Incr. risk of prostate cancer -Growth restriction |
|
|
What is Calcipotriene and when is it used? |
-VitD analog -Used for osteoporosis, osteomalacia, renal failure, malabsorption, and psoriasis Adverse effects: -Hypercalcemia, hypercalciuria -VitD preps have much longer half-life than the metabolites and analogs |
|
|
What are the anabolic agents administered as drugs for osteoporosis? |
PTH and Teriparatide Mech of action: PTH receptors are present on osteoblasts and osteoclasts -With hyperparathyroidism: chronically high PTH incr. Ca2+ resorption from the bones and incr. Ca2+ levels in the blood & calciuria Pulsatile dosing: incr. GI absorption of Ca2+ and incr. renal tubular reabs. or Ca2+ and sitmulates osteoblastic function, leading to bone mineralization |
|
|
When is PTH used? |
Protact (PTH 1-84) and Teriparatide (PTH 1-34) -Used for osteoporotic postmenopausal women at high risk of fracture, previous osteoporotic fracture, multiple RFs for fracture, extremely low BMD (<2.5) or failed/intolerant to previous treatment -Also primary or hypogonadal osteoporosis in men at high risk of fracture(dec. risk of new vertebral fractures of non-vertebral fractures) |
|
|
What are the averse effects of Teriparatide |
-Dizziness, rash, nausea, headache, leg cramps, arthralgia, rhinitis, transient hypercalcemia (s/s: nausea, vomiting, constipation, low energy, muscle weakness) -Black box warning: Osteosarcoma risk in animals |
|
|
When is PTH and Teriparatide contra-indicated? |
Paget's disease of bone Prior radiation therapy to skeleton Bone mets Hypercalcemia History of skeletal malignancy Pregnant/nursing |
|
|
What are the bacterial cell walls synthesis inhibitors? |
Penicillins Cephalosporins Carabapenems Monobactam Vancomycin Bacitracin Fosfomycin |
|
|
What are the bacterial protein synthesis inhibitors (ribosomally active antibiotics)? |
Aminoglycoside Chloramphenicol Macrolides Tetracyclines Streptogramins Linezolid |
|
|
What are the nucleic acid synthesis inhibitors? |
Fluoroquiniolones Rifampin
|
|
|
What are the folic acid synthesis inhibitors? |
Sulfonamides Trimethoprim Pyrimethamine |
|
|
What are bacteriostatic drugs? |
Inhibit the bacterial growth at drug serum levels achievable at in patients. Intact cellular immunity is required to get rid of the static bacteria -Not preferred in immunocompromised patients as bacteria will resurface Ex: Sulfonamides, tetracyclines, erythromycin |
|
|
What are bactericidal drugs? |
Kill bacteria at drug serum levels achieved in patient -Preferred for QUICK action (in seriously ill patients) and in immunocompromised patients Ex: Penicillin, cephalosporin, aminoglycosides, fluoroquinolones |
|
|
What are narrow spectrum antimicrobials? |
Penicillin G Isonazid |
|
|
What are extended spectrum antimicrobials? |
Ampicillin |
|
|
What are broad spectrum antimicrobials? |
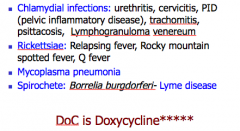
Tetracyclines and chloramphenicol These can cause super/supra-infections by an organism, such as CANDIDA whose growth is normally kept in check by the presence of other organisms (normal flora) |
|
|
Which drugs exhibit Concentration-dependent killing rates? Which do not? |
CDKR: Aminoglycosides (such as tobramycin) and Fluroquinolones (such as ciprofloxacin) exhibit CDKR against a large group of gram negative bacteria (incl. Pseudomonas aeruginosa, members of enterobacteriaceae) -In contrast, penicillins and other beta lactam antibiotics usually do not exhibit CDKR |
|
|
What is the post-antibiotic effect (PAE)? |
After an antibacterial drug is removed from bacterial culture, if the antibacterial effect still persists on bacterial growth --> PAE -Most BACTERICIDAL antibiotics show PAE against susceptible pathogens, e.g penicillins show PAE against Gram + cocci, and AGs show PAE against Gram - bacilli -Prevents any remaining bacteria from replicating for several hours after the drug has been eliminated from the body |
|
|
For which diseases must we give empiric therapy? |
Neutropenia and Meningitis |
|
|
What is empiric therapy? |
The treatment that is initiated after specimens for lab analysis have been obtained but before the results of the culture are available. -Broad spectrum antibiotic is given in case of a life threatening serious infection, before the culture/sensitivity report is available |
|
|
How is microbial sensitivity measured? |
1. Broth dilution method 2. Disc diffusion method (Kirby-Bauer test) 3. Etest method |
|
|
What is the minimum inhibitory concentration (MIC)? |
Lowest concentration of antibiotic that inhibits bacterial growth |
|
|
What is the minimum bactericidal concentration (MBC)? |
Lowest concentration of antibacterial that results in 99.9% decline in colony count after overnight incubation. |
|
|
Accessibility of antimicrobials to a particular organ depends upon what? |
1. Lipid solubility of the drug (Metronidazole can easily penetrate and reach the CNS, whereas Penicillins can not under normal circumstances) 2. Molecular weight of the drug 3. Protein-binding of the drug |
|
|
What are the sites of infection that all antibiotics cannot reach easily? |
Prostate Vitreous body of the eye CNS (BBB) |
|
|
What is specific treatment? |
Started after getting the culture and sensitivity (C/S) report of the sample from the infection site |
|
|
What is prophylactic therapy ? |
Indiscriminate use can result in bacterial resistance and superinfection, so should be restricted to certain clinical situations in which benefits outweigh the risks. |
|
|
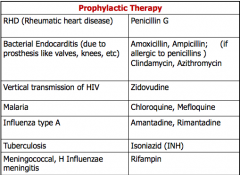
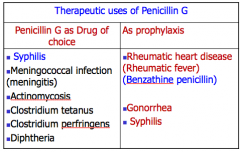
What are the 7 situations in which prophylactic therapy is advised? |
1. Rheumatic heart disease: Prevention of Strep infection; patients may require years of treatment (in prevention of cardiomyopathy) 2. Pretreatment in patients with artificial heart valves who are at high risk for endocarditis (undergoing dental extraction) 3. Treatment of mother with Zidovudine to protect the fetus in case of an HIV-infected pregnant woman 4. Antibacterial treatment prior to some surgical procedures to prevent infection 5. To prevent Influenza type A: Amantadine or Rimantadine 6. To prevent Malaria: Chloroquine, Mefloquine 7. Prevention of TB (INH) or Meningitis (Rifampin) among individuals who are in close contact with infected patients |
|
|
Prophylactic therapy table |
|
|
|
What is an example of synergistic combo antimicrobial therapy? |
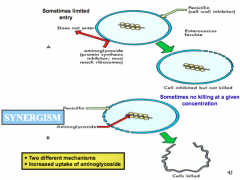
Penicillin + aminoglycoside (ex: Gentamycin) |
|
|
What are indications for the clinical use of combo antimicrobial agents? |
1. For empiric therapy of an infection in which the cause is unknown 2. For treatment of polymicrobial infection 3. To enhance antimicrobial activity for a specific infection 4. To prevent emergence of resistance, e.g. multi drug therapy for TB infection |
|
|
What are disadvantages of antimicrobial combos? |
Many antibiotics act only when the organisms are multiplying Coadministration of bactericidal and bacteriostatic drug may result in interference of bactericidal effect. |
|
|
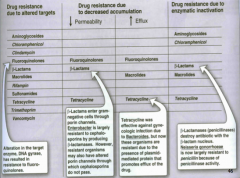
What are the consequences of drug resistance? |
1. Inactivation of the drug by the microbial enzymes 2. Decreased accumulation of the antimicrobial drug by the microbes (decr. uptake, incr. efflux) 3. Reduced affinity of the target macromolecule for the drug 4. Altered metabolic pathways |
|
|
Antimicrobial resistance examples |
|
|
|
What is a superinfection? |
Defined as the appearance of bacteriological and clinical evidence of a NEW infection during the chemotherapy of a primary infection. Use of broad-spectrum antibiotics or combo agents can lead to alterations of normal microbial flora of the URT, intestinal, and GIT. Permits the overgrowth of opportunistic organisms, esp. fungi or resistant bacteria. -Diff to treat -Broad spec antibiotics: Tetracyclines, Chloramphenicol -*Pseudomembrane colitis (C. diff), candida infection
|
|
|
What are the cell wall synthesis inhibitors? |
-Beta lactam antibiotics: Penicillin, cephalosporins, Carbapenems (Doripenem, Ertapenem, Imipenem, Meropenem, Ertapenem), Monobactam (Acteronam) -Vancomycin -Teicoplanin -Bacitracin -Fosfomycin -Cycloserine (used for TB as 2nd line therapy) -Daptomycin |
|
|
Which class of antibiotics inhibit cell wall synthesis? |
Beta lactams (most important class of antibiotics) -All cell wall synthesis inhibitors are bacteriCIDAL -Possess 4 member nitrogen containing beta lactam rings -The integrity of the beta lactam ring is required for antibacterial activity |
|
|
Penicillin structure |
Consists of a 5 member SULFUR-containing thiazolidine ring fused to a beta-lactam ring -Modifications of the R-group side chain (attached to the beta lactam ring) alter the pharmacological properties and resistance to beta-lactamase |
|
|
Penicillin mechanism of action |
-Bacterial cell wall is a cross-linked polymer of polysaccharides and pentapeptides -Penicillins interfere with cell wall synthesis (peptidoglycan) by binding to Penicillin Binding Protein (PBP)***, thus inhibiting cross linking of peptide chains (transpeptidation) of the bacterial cell wall - --> Cell wall-deficient bacteria that are lysed easily -Cell wall is unique to bacteria, thus non-toxic to humans |
|
|
Which 2 types of antibiotics activate autolysins? |
Penicillins and Cephalosporins -Autolysins are bacterial enzymes that remodel and breakdown the cell wall, and are involved in bacterial cell death |
|
|
Other than both being autolysins, what other property do penicillins and cephalosporins share? |
BACTERICIDAL -More effective when the cells are actively dividing/growing and synthesizing cell wall -Activity depends on maintaining the concentration above MIC for the entire dosing interval |
|
|
What are the methods by which organisms have either natural or acquired resistance to beta lactam antibiotics? |
-Natural resistance: To penicillins occurs in organisms that either lack a peptidoglycan cell wall (e.g. mycoplasma) or have cell walls that are impermeable to the drugs -Acquired resistance: To penicillins occurs by PLASMID transfer (sig. clinical problem) |
|
|
What are the mechanisms of resistance development against penicillins and other beta-lactam antibiotics? |
1. Enzymatic hydrolysis of beta-lactam ring by beta-lactamase enzyme (e.g. Staph), results in loss of bactericidal activity (most common mechanism of resistance) 2. Structural changes in PBPs (e.g. MRSA, penicillin-resistant pneumococci, and enterococci) 3. Change in porin structure (reduced permeability in gram - organisms, e.g. pseudomonas) 4. Efflux: Gram- organism may also produce an efflux pump, which efficiently transport some beta lactam antibiotics from the periplasm back across the outer membrane |
|
|
What are the 4 classes of penicillins? |
1. Standard (natural) penicillins 2. Antistaphylococcal penicillins 3. Aminopenicillins 4. Antipseudomonal pencillins
3&4 are extended spectrum penicillins |
|
|
What are standard/natural penicillins? |
Narrow spectrum, beta lactamase/penicillinase sensitive -Penicillin G (Benzyl penicillin): Acid-labile, parenteral, highly water soluble, stable in dry state, solutions are freshly prepared -Procaine and Benzathine Penicillin G are repository (depot) form of IM injection* -Phenoxymethal pencillin (Pen V) are acid RESISTANT, thus oral |
|
|
What is the spectrum of standard/natural penicillins? |
Have the greatest activity against Gram+ and Gram- cocci (streptococci, pneumococci, meningococci), and non-beta lactamase producing anaerobes; not active against gram- rods -Good activity against Treponema Pallidum |
|
|
Anti-staphylococcal penicillins |
Very narrow spectrum, beta lactamase/penicillinase resistant penicillin -Methicillin, Nafcillin, Oxacillin, Cloxacillin, Dicloxacillin
|
|
|
What is the spectrum of anti-staph penicillins? |
Known or suspected staph (NOT MRSA); also against streptococci, but NOT against enterococci, anaerobic bacteria, and gram- cocci and rods |
|
|
Aminopenicillins |
Extended spectrum, beta-lactamase sensitive -Ampicillin, amoxicillin
|
|
|
Aminopenicillin spectrum |
Gram+ cocci (NOT staph) and greater activity than penicillins (Pen G) against Gram- bacteria E.coli, H.influenza, Listeria monocytogenes (Ampicillin), Borrelia burgdorferi (Amoxicillin), and H.pylori (Amoxicillin) |
|
|
Antipseudomonal penicillins |
Extended spectrum, beta lactamase SENSITIVE -Carboxypenicillins: Carbenicillin, Ticarcillin -Ureidopenicillins: Piperacillin, Azlocillin, Mezlocillin |
|
|
Crystalline benzyl benicilline is measured in which units? |
International units (IUs) 1IU of crystalline benzyl penicillin = 0.6ug of standard prep |
|
|
Pharmacokinetics of natural penicillins (PenG) |
Destroyed by the gastric acid, hence given parenterally (preferred IV than IM because of irritation and local pain from IM inj) -Except for oral amoxicillins, penicillins should be given 1-2 hours before or after a meal -Distributed widely, mainly extracellularly (although it does not cross the BBB, during inflammation (meningitis), entry is facilitated) -Very little metabolized |
|
|
What can increase the concentration of PenG in the plasma by inhibiting tubular secretion? |
Probenecid (competitor for active secretion) -Most PenG is excreted unchanged in the urine (via active tubular secretion) -Probenecid inhibits the tubular secretion of PenG (90% of PenG is eliminated by tubular secretion and 10% by glomerular filtration). -Blood levels of all penicillins can be raised by simultaneous administration of Probenecid -Half life of PenG is 30 min |
|
|
What can increase the concentration of PenG in the plasma by delaying absorption? |
Benzathine and Procaine: results in prolonged blood and tissue concentration -A single IM inj. of 1.2 million units of Benzathine Pencillin would be suff. for 3 weeks -A 600 unit of procaine penicillin is suff. for 12-24 hours |
|
|
What is the main adverse effect of penicillins? |
Allergic reactions: pruritic rash, anaphylaxis -High therapeutic index, generally well tolerated -Safe to use in pregnancy as long as patient is not allergic |
|
|
What are the therapeutic uses of PenG Benzyl pen and Pen V? |
Limited use (esp. Gram+ bacteria) due to high incidence of resistant strains -Strep, N. gonorrhea, N. Meningitidis, C. Diphtheria, C. tetani, C. Perfringens, Actinomyces, Treponema (Syphilis) (no resistance reported to Treponema) |
|
|
What is used to treat beta-hemolytic strep and syphilis? |
Benzathine penicillin -A single inj. every 3-4 weeks for beta-hemol. strep pharyngitis -2.4 units IM once a week for 1-3 weeks effective for syphilis |
|
|
What is used to treat uncomplicated pneumococcal pneumonia or gonorrhoea? |
Procaine Penicillin -Formerly the mainstay med. , rarely used now because of resistance |
|
|
Therapeutic uses of PenG |
|
|
|
What are the penicillinase resistant penicillins? |
Methicillin,Nafcillin, Isoxazolyl Penicillins (Cloxacillin, Oxacillin, Dicloxacillin) -Used only against the beta-lactamase/penicinillase producing staph
|
|
|
Which penicillinase resistant penicillin is lipid soluble, crosses BBB, and primarily excreted in BILE**, hence can be given with renal impairment? |
Nafcillin |
|
|
Which penicillinase resistant penicillin causes nephrotoxicity (interstitial nephritis, tubular necrosis) and no longer used? |
Methicillin |
|
|
What is the mechanism of resistant development (MRSA) used by staph? |
Alter the PBPs (structure of the PBPs altered) which do not bind with penicillins**** |
|
|
What are the anti-staph penicillins that are the drugs of choice for treatment? |
Methicillin****, Nafcillin, and Cloxacillin |
|
|
Isoxazolyl penicillins |
Cloxacillin, oxacillin, dicloxacillin -Food interferes with their absorption, hence the drugs should be administered 1 hour before or after meals |
|
|
What do you give to somebody who is infected by methicillin-resistant staph aureus? |
Vancomycin***** |
|
|
What do you give to somebody who is infected by Vancomycin-resistant staph? |
Linezolid, Quinupristin/Dalfopristin |
|
|
Aminopencillins (extended spectrum penicillins) |
-Have greater activity than Penicillin against Gram- bacteria (bc of their limited enhanced ability to penetrate the Gram- outer membrane) -Inactivated by many beta-lactamases -Include Ampicillin and Amoxicillin - Both have nearly identical spectrum of activity (enhanced activity against aerobic gram+ and gram- bacilli) -Better oral efficacy
|
|
|
What do we combine with aminopenicillins and anti-pseudomonals to protect them from hydrolysis by bacterial lactamase enzymes? |
Beta-lactamase inhibitors: Clavulanic acid, Sulbactam, and Tazobactam |
|
|
Ampicillin |
-Extended spectrum amino penicillin used against anaerobes, enterococci, L monocytogenes, Beta-lactamase negative strains of E.coli and Salmonella -Not degraded by gastric acid, but food interferes with absorption -Excreted in the bile partly - undergoes enterohepatic circulation
|
|
|
What is the drug of choice against Listeria monocytogenes? |
Ampicillin -L. monocyto causes meningitis in immunocompromised patients -Used along with amino glycosides |
|
|
What is the most common side effect of Ampicillin? |
Diarrhea -Can also cause pseudomembrane colitis |
|
|
Amoxicillin |
-Aminopenicillin -Completely absorbed -Food DOES NOT interfere with its absorption -NO diarrhea -NO pseudomembrane colitis (Absorption of most oral penicillins (except Amoxicillin) is impaired by food, and the drugs should be administered at least 1-2 hours before or after a meal) |
|
|
Which drug is most commonly used against URT infections? (Pharyngitis, sinusitis, S. Pneumoniae, H. influenza) |
Amoxicillin -Addition of beta lactamase inhibitors (Amoxicillin+clavulanic acid or ampicillin+sulbactam) can extend the spectrum to beta-lactamase producing strains |
|
|
What can be used as empiric treatment of suspected bacterial meningitis? |
Ampicillin+Vancomycin+third generation cephalosporins |
|
|
Which drug is preferred for UTIs? |
Amoxicillin -Uncomplicated UTI caused by enterobacteriaceae and E.coli |
|
|
What drug is used against salmonella infections? |
Ampicillin: good for typhoid carrier state in patients without gall bladder disease and also used for salmonella gastroenteritis |
|
|
What drug is used for Shigellosis? |
Ampicillin |
|
|
What drug is used as prophylaxis by dentists for patient with abnormal heart valves who are to undergo extensive oral surgery? |
Amoxicillin, oral |
|
|
Resistance to aminopenicillins |
A major clinical problem because of inactivation by plasmid-mediated penicillinase (E.coli and H. influenza are frequently resistant) -Formulation with a beta-lactamase inhibitor, such as clavulanic acid or sulbactam, protects amoxicillin of ampicillin, resp. from enzymatic hydrolysis and extends their antimicrobial spectrum |
|
|
Carboxypenicillins |
Carbenicillin, Ticarcillin -Part. active against Pseudomonas aeruginosa -Preferably used in nosocomial infections by gram- organisms (such as pseudomonal infections in burn patients, CF) - life threatening conditions - |
|
|
What does a high dose of carboxypenicillins causes? |
Bleeding by interfering with platelet function
|
|
|
What are the 2 classes and subclasses of antipseudomonal penicillins? |
Carboxypenicillins: Carbenicillin, Ticarcillin Ureidopenicillin: Piperacillin, Azlocillin, Mezlocillin |
|
|
Ureidopenicillins |
Piperacillin, Aziocillin, Mezlocillin -Similar to ticarcillin -Active agent against Pseudomonas, enterobacter, and many klebsiella -Combined with amino glycosides or fluroquinolones for pseudomonal infections outside the urinary tract (because of their propensity of the P aeruginosa to develop resistance if used anti-pseudomonal penicillins alone) |
|
|
What is the major adverse effect of all penicillins? |
Hypersensitivity (Type I and 4): with wide range of reactions ranging from urticarial rashes (common), angioedema (marked swelling of lips, tongue and periorbital areas), and anaphylaxis -However, if necessary (e.g. treatment of enterococcal endocarditis or neurosyphilis in a patient with serious penicillin allergy), desensitization can be accomplished with gradually increasing doses of penicillin. -The major antigenic determinant - Penicilloic acid (degradation products of penicillins and products of alkaline hydrolysis bound to host protein) -Cross-allergic reactions (cross-sensitizing and cross-reacting) |
|
|
What are other adverse effects of penicillins? |
1. Nephrotoxicity: Methicillin causes interstitial nephritis, tubular necrosis; hence no longer avail. 2. Neurotoxicity: In response to HIGH doses causing seizures and convulsions if given intrathecally or in patients with renal failure 3. Platelet dysfunction: Carbenillin, Ticarcillin 4. GI distress: nausea, vomiting, and diarrhea (Ampicillin) due to disruption of the normal balance of intestinal microorganisms 5. Cation toxicity: sodium/potassium 6. Jarisch-Herheimer reaction: Penicillin injected in a syphilitic patient (part. 2ndary syphilis) produce fever, malaise, joint pain exacerbation of lesions, hypo tensions, etc. Does not need interruption of therapy |
|
|
What are the beta-lactamase inhibitors? |
Clavulanic acid, sulbactam, tazobactam -Lactamases are enzymes produced by gram+ and gram- organisms. They inactivate beta-lactam antibiotics by opening the beta-lactam ring. -Beta lactamase inhibitors resemble a beta-lactam molecule, but, by themselves do not have sig. antibacterial activity -They are imp. inhibitors of many but not all bacterial beta lactamases and can protect hydrolyzable penicillins from inactivation by these enzymes. |
|
|
Examples of beta-lactamase inhibitors |
1. Amoxicillin+Clavulanic acid (oral) 2. Ticarcillin+Clavulanic acid (parenteral) 3. Ampicillin+Sulbactam (parenteral) : Active against beta-lactamase-producing S.aureus and H.influenzae but not against serratia, which produces a beta lactamase that is not inhibited by sulbactam 4. Piperacillin+Tazobactam (parenteral): if a strain of p.aeruginosa is resistant to peiperacilin, it is also resistant against it+beta lactamase inhib. because tazobactam doe not inhibit the chromosomal beta lactamase produced by P.aeruginosa. |
|
|
Cephalosporins |
Are beta lactam antibiotics, closely related to penicillins, but more stable to many bacterial beta-lactamases and therefore have a broader spectrum of activity. -Most are produced semisynthetically by the chemical attachment of side chains to 7-aminocephalosporanic acid (obtained from fungus cephalosporin) |
|
|
Cephalosporins are NOT active against what? |
LAME: -Listeria monocytogenes -Atypical (e.g. chlamydia, mycoplasma) -MRSA -Enterococci Another clinical concern is growing resistance by strains of E.coli and Klebsiella (M/A: identical to pens as is M/R) |
|
|
First generation cephalosporins |
Parenteral: Cefazolin Oral: Cephalexin, cefadroxil, cephradine -Resistant to staph penicillase and are v. active against pneumococci, streptococci, and staph. -Highly active against GRAM+ cocci (not MRSA) but also have weak activity against some gram- organisms (poor activity against pseudomonas) -Active against gram- bacteria such as proteus mirabilis, E.coli, Klebsiella (PEcK) |
|
|
Uses of first generation cephalosporins |
-Surgical prophylaxis against Gram+ bacteria (Cefazolin used due to longer half-life and its activity against penicillinase producing S.aureus) -Cefazolin: orthopedic surgery bc able to penetrate bone -Cephalexin: URT infection (ex: pharyngitis) -Used in penicillin and sulfonamide-resistant UTI |
|
|
First generation cephalosporin pharmacokinetics |
-None enter CNS (cannot treat meningitis) -Water soluble, eliminated through KIDNEY (glomerular filtration and tubular secretion); dose must be reduced in patient w/ impaired kidney -Probenezid increases serum level substantially |
|
|
Second generation cephalosporins |
Parenteral: Cefuroxime, Ceforanice, Cefoxitin, Cefamandole, Cefotetan*** Oral: Cefaclor, cefurozime axetil, cefprozil -More activity against GRAM- organisms, incl. some anaerobes (B.fragilis, it can cause life-threatening intra-abdominal infections, esp. after bowel rupture/perforation); however, weaker gram+ coverage -Gram-: H.influenzae, enterobacter aerogenes, N.meningitidis+PeCK (HENPEcK)**
|
|
|
Which 2nd generation cephalosporins are active against H.influenzae but no activity against B fragilis? |
Cefamandole, Cefuroxime, Cefactor |
|
|
Which 2nd generation cephalosporins have weak activity against H.influenzae, but are more active against B.fragilis |
Cefotetan and cefoxitin |
|
|
Which 2nd generation cephalosporins are active against enterococci or pseudomonas (like 1st gen.)? |
NONE -Note: although Cefuroxime crosses the BBB, it is less effective in treatment of meningitis than ceftriaxone or cefotaxime and should NOT be use. |
|
|
What are the therapeutic uses for 2nd generation cephalosporins? |
-Upper+lower RTIs (oral prep) -Anaerobic infections : Cefoxitin, Cefotetan, Cefmetazole -Community-acquired pneumonia: Cefuroxime |
|
|
What are the 3rd generation cephalosporins? |
-Parenteral: Cefotaxime, ceftriaxone, Ceftazidime, Cefoperazone, Ceftizomine -Oral: Cefixime, Cefdinir, Cefitoren pivoxil, Cefibuten, Cefpodoxime proxetil |
|
|
Compared to 2nd generation agents, what do 3rd gen. cephalosporins offer? |
Expanded gram- coverage -Highly active against gram+ cocci (<1st gen.) +gram-, plus enhanced activity against Gram- bacilli (incl. HENPEcK), enterobacteriacae, pseudmonas, and serrate marcescens. -RESISTANT TO MOST LACTAMASES |
|
|
What are the 3rd generation cephalosporins? |
-Parenteral: cefotaxime, ceftriazone, ceftazidime, Cefoperazone, Ceftizoxime -Oral: Cefixime, Cefdinir, Cefitoren pivoxil, cefibuten, cefpodomine proxetil |
|
|
What is an important therapeutic use of 3rd gen. cephalosporin? |
Empiric management of sepsis of unknown cause in both immunocompromised and immunocompetent patients -In neutropenic or immunocompromised patients, Ceftazidime is often used in combo with other antibiotics |
|
|
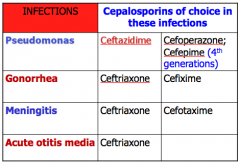
What is the agent of choice in the treatment of meningitis (caused by pneumococci, meningococci, h.influenzae, and susceptible gram- rods, but NOT L.monocytogenes)?
|
Ceftriaxone or Cefotazmine***
|
|
|
What 3rd gen. cephalosporin is active against P.aeruginosa? |
Ceftazidime and Cefoperazone |
|
|
What is used to treat uncomplicated gonococcal urethritis, cervicitis? |
3rd gen. cephalosporin- Cefixime (oral) |
|
|
What is used to treat typhoid fever? |
DoC is fluoroquinolones (ciprofloxacin), or can use 3rd gen. cephalosporin because equally effective. |
|
|
What is the only generation of cephalosporin to enter the CNS? |
3rd gen. - except cefoperazone
|
|
|
How is cefoperazone and ceftriazone mainly excreted? |
Biliary tract - no adjustment required for renal insuff. (others are excreted by kidney and require dosage adjustments) |
|
|
What are the parenteral 4th gen. cephalosporins? |
Cefepime, Cefpirome (enter the CNS) -More resistant to beta lactamase -Combines with gram+ activity of 1st gen. (including strep and staph, but not against MRSA) with the wider gram- spectrum of 3rd gen. -Cefepime: good activity against pseudomonas, enterobacteriaceae, S. aureus, and S.pneumoniae. Highly active against Hemophilus and Neisseria spp. |
|
|
Which cephalosporin is active against Methicillin-resistant staph (MRSA)? |
Ceftaroline fosamil*** -A pro-drug of an active metabolite Ceftaroline -Treats community acquired bacterial pneumonia and acute bacterial skin infections |
|
|
Table of cephalosporin per infection |
|
|
|
Pharmacokinetics of cephalosporins |
-Majority given by IV or IM (except those mentioned) due to poor oral absorption -Distribute well in the body fluids. However, adequate therapeutic levels in the CSF regardless of inflammation are achieved only with 3rd gen. cephalosporins **** -Hence, Ceftriazone are effective in the treatment of neonatal and childhood meningitis, caused by Strep agalactiae, E.coli, H.influenza, N.meningitidis, Strep pneumo) -Renal clearance similar to penicillin, with active tubular secretion blocked by Probenecid (dose must be adjusted in renal dysfunction) -Cefoperazone and ceftriaxone are largely eliminated via bile (can be given to those with renal insuff.) |
|
|
What is a major adverse effect of cephalosporins? |
Hypersensitivity reactions (identical to those of Penicillin) -Complete cross-allerginicity b/w individual cephalosporins and partial cross-allergenicity with penicillins (so if allergic to one, can't treat with other) -Patients with a history of anaphylaxis to penicillins should NOT receive cephalosporins |
|
|
If a person is allergic to penicillins, we do not give cephalosporins. So, what do we give to kill a gram+ organism? gram-? |
Gram+: Macrolides Gram- rod: Aztreonam **** |
|
|
Which drug causes bleeding due to hypoprothrombinemia? |
Cephalosporins: cefoperazone, cefamandole, cefotetan, cefmetazole -Due to MTT: methylthiotetrazole side-chain*** -Administration of VitK corrects the problem
|
|
|
Which drugs cause a disulfiram-like reaction? |
Cefoperazone, cefamandole, cefotetan, cefmetazole -Due to MTT side-chain -* causes build-up to aldehyde metabolites by blocking aldehyde dehydrogenase (causes aversion to alcohol in alcoholics) |
|
|
Other side effects of cephalosporins |
-Pain @ site of injection -Diarrhea due to alteration of gut ecology -Nephrotoxicity (esp. cephaloridine, hence withdrawn) |
|
|
What are the carbapenems? |
Doripenem Ertapenem Imipenem Meropenem -Are structurally related to beta lactam antibiotics |
|
|
Carbapenem features |
-M/A same as penicillin and cephalosporin -Resistant to most beta-lactamases (but not carpapenemases and metallo-beta-lactamases)
|
|
|
Carbapenem spectrum |
-Most potent and widest spectrum lactams -Active against penicillinase producing Gram+ cocci, gram- rods (e.g. enterobacter and pseudomonas aeruginosa) and anaerobe -Among them, Ertapenem is insuff. active against P.aeruginosa and should NOT be used for pseudomonal infections -Overall, very potent! |
|
|
Uses of carbapenems- doripenem, imipenem, meropenem |
-Imp. in in-hospital agents for empiric use in severe life-threatening infections (due to pseudomonas infections, mixed aerobic and anaerobic infections) --> currently DoC for infections due to enterobacter -Active against many penicillin-resistant strains of pneumococci -Used in febrile neutropenic patients in ICU, +/- aminoglycosides -Cannot be used against MRSA |
|
|
What is imipenems limiting feature? |
Hydrolysis by dehydropeptidase by brush border tubular cells of the kidney -Cilastatin is an inhibitor of the renal dehydropeptidase and is used clinically along with imipenem -Other carbapenems (doripenem, ertapenem, and meropenem) are NOT sig. degraded by dehydropeptidases |
|
|
Pharmacokinetics of Doripenem, Ertapenem, Imipenem, and Meropenem |
-Administered by IV and IM injection (IM injection of Ertapenem is irritating, hence formulated with 1% lidocaine) -Imipenem is given with cilastatin -Metabolites formed by dehydropeptidase are inactive, but potentially nephrotoxic -All carbapenems undergo renal elimination-hence dose should be decreased in renal dysfunction
|
|
|
What are the adverse effects of carbapenems (doripenem, ertapenem, imipenem, meropenem)? |
-GI distress: nausea, vomiting, diarrhea -Drug fever: partial cross-allergenicity with penicillin -CNS effects: Imipenem causes SEIZURES * (in 50% of patients) in overdose and renal dysfunction (like penG) -Doripenem, ertapenem, meropenem are much less likely to cause seizures than imipenem |
|
|
What is the only monobactam we learned? |
Aztreonam -M/A: similar as penicillins and cephalosporins -Resistant to beta lactamases, given IV or IM -Only used in IV form for aerobic gram- rods** (Such as H.Influ, pseudomonas, and enterobacteriacease) -NO activity against Gram+ anaerobes -Penicillin-allergic patients tolerate it (no cross-allergenicity with penicillins or cephalosporins): if allergic to penicillin, given for gram-rods |
|
|
What is the main indication for aztreonam use? |
Hospital acquired infection and also useful in patients with pseudomonal infection who are allergic to penicillins*** -If history of penicillin anaphylaxis, treats serious infections such as pneumonia, meningitis and sepsis by susceptible gram- pathogens |
|
|
What are 2 glycopeptide antibiotics which inhibit synthesis of peptidoglycan bacterial cell wall (bactericidal ultimate effect)? |
Vancomycin, Teicoplanin -Binds to D-Ala-D-Ala terminus of the nascent peptidoglycan pentapeptide side chain and inhibits transglycosylation. Prevents elongation of the peptidoglycan chain and interferes with cross-linking. -Does NOT depend upon binding with PBPs to produce effect (hence active against MRSA)** |
|
|
What is the antibacterial spectrum of vancomycin? |
Active only against gram+ bacteria -Enterococci: synergistic action with amino glycosides (streptomycin and gentamicin) -MRSA |
|
|
Resistance to Vancomycin |
Rare- however, Vancomycin-resistant staph aureus (VRSA) and vancomycin-resistant enterococcal (VRE) strains are emerging (in surgical and burn wards) -Resistance involved decreased affinity for the binding site due to replacement of terminal D-Ala by D-Lactate |
|
|
Vancomycin pharmacokinetics |
"Red man" or "Red neck" syndrome -Type I HSR -Characterized by flushing, pruritis, erythema of the head and upper body and hypotension resulting from histamine release after rapid IV injection-due to HISTAMINE release -Can largely be prevented by prolonging the infusion period (1-2 hours) or pretreatment with anti-histamines
-Ototoxicity (usually permanent, additive with other drugs such as amino glycosides, furosemide, ethacrynic acid) -Nephrotoxicity (mild, but additive)
|
|
|
What is the drug of choice for infections due to MRSA? (bloodstream infections and endocarditis) |
Vancomycin -In combo with gentamicin, it is an alternative regimen for treatment of enterococcal endocarditis in a patient with serious penicillin allergy -In combo with cefotaxime, ceftriaxone, or rifampin - also recommended for treatment of meningitis due to penicillin-resistant strains of pneumococcus -Back up drugs for C.diff enterocolitis (given orally) (Metronidazole is DoC) |
|
|
What do we give for vancomycin-resistance? |
Linezolid Quinupristin/daflopristin -2 protein inhibitors are used for the treatment of vancomycin resistant organisms |
|
|
What is the analog of phosphoenolpyruvate and inhibits bacterial wall synthesis? |
Fosfomycin -Active against both gram+ and gram- -Oral and parenteral preps are also available -SAFE IN PREGNANCY -Used for treatment of uncomplicated lower UTI in women |
|
|
What is a mixture of polypeptides that inhibit bacterial cell wall synthesis? |
Bacitratcin -Active against Gram+ bacteria -Restricted to topical application because of its potential nephrotoxicity -One of the components of "triple antibiotic" (along w/ polymixin or neomycin) used as a topical antibiotic (ointment, dusting powder) for the suppression of mixed bacterial flora in surface lesions of the skin, in wounds, or on mucous membranes) |
|
|
What is a structural analog of D-alanine and inhibits incorporation of D-alanine into peptidoglycan pentapeptide (bound to NAM) by inhibiting alanine racemes and D-alanyl-D-alanine ligase? |
Cycloserine -Used to treat TB caused by strains resistant to first-line agents -Causes dose-related CNS toxicity (headache, tremors, acute psychosis, and convulsions) |
|
|
Daptomycin |
-Spectrum of activity similar to Vancomycin (may be active against vancomycin-resistant strains of enterococci and S.aureus) -M/A not fully understood -However, it binds to the cell-membrane via calcium-dependent insertion of its lipid tail, resulting in depolarization of the cell membrane with potassium efflux and rapid cell death -Used for skin and soft tissue infections, bacteria, and endocarditis (effective alternative to vancomycin) -Adverse effect: myopathy and allergic pneumonitis -Should not be used to treat pneumonia as pulmonary surfactant antagonizes its action |
|
|
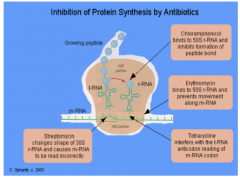
Inhibition of protein synthesis by antibiotics |
|
|
|
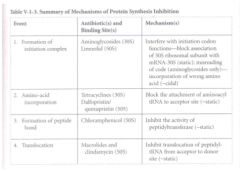
Summary of mechanisms of protein synthesis inhibitors |
|
|
|
Bacterial protein synthesis inhibitors |
-Aminglycosides, spectinomycin -Tetracyclines -Chloramphenicol -Macrolides, clindamycin -Linezolid -Quinupristine/Dalfopristine (Streptogramins) |
|
|
Drugs that affect 30s ribosomes |
-Aminoglyocosides (Gentamicin, Streptomycin) -Tetracylcins (Tetracycline, Doxycycline) -Spectinomycin |
|
|
Drugs that affect 50s ribosomes |
-Chloramphenicol -Macrolides (erythromycin, azithromycin) -Clindamycin -Quinupristin-Dalfopristin (Streptogramins) -Linezolid |
|
|
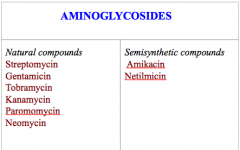
Aminoglycosides |
|
|
|
Aminoglycoside mechanism of action |
Aminoglycosides "irreversibly" bind to the 30s subunit 1. interfere with the initiation complex of peptide formation -interfere with initiation codon functions by blocking association of 50s ribosomal subunit with mRNA 30s (-STATIC) 2. Misreading of mRNA-incorporation of incorrect amino acids into the peptide, resulting in non-functional or toxic protein *** (-CIDAL) |
|
|
Aminglycosides are bactericidal against what? |
Gram- aerobic bacteria (bacilli)
|
|
|
Transport of amino glycosides inside the bacteria depends on what?
|
-O2-dependent process: amino glycosides are actively transported across the cytoplasmic membrane of aerobic gram- bacteria into the cytoplasm (anaerobes are innately resistant)
-Transport may be enhanced by the cell wall-active drugs such as penicillin or vancomycin --> Synergism -They exhibit concentration dependent killing ** and post antibiotic effect** |
|
|
Resistant to aminoglycosides |
1. inactivation by acetylation, adenylation, and phosphorylation -Plasmid-mediated synthesis of enzymes (e.g. acetyl transferases, nucleotidyltransferases, and phosphotransferases) that modify and inactivate aminoglycoside antibiotics 2. Impaired entry into the cell resulting from mutations or deletion of a porin protein or the proteins involved in the O2 dependent transport 3. Mutation of receptor protein on the 30s |
|
|
Which 2 amino glycosides are less vulnerable to the resistance enzymes? |
Netilmicin and Amikacin*** |
|
|
Aminoglycoside pharmacokinetics |
-Water soluble, poor absorption from the intact intestine, almost the entire oral dose is excreted in feces after oral administration; necessitates their parenteral admin (IM or IV) -Highly polar compounds, do not enter cells readily -CSF concentration is poor -Cleared by the kidney, attain a high concentration in urine and excretion is directly proportional to creatinine clearance -SINGLE daily dose is just as effect (less toxic-ototoxic and nephrotoxic) than multiple smaller doses -Exhibits CDK and PAE |
|
|
Streptomycin is active against what? |
-Yerisinia pestis (plague) -DoC -Francisella tularensis (tularemia) -DoC -Mycobacterium tuberculosis (less active against P.aeruginosa) Many bacteria have developed resistant to streptomycin, severely limiting the usefulness of the drug -Also used in TB and endocarditis (enterococcal and viridans strep): streptomycin and penicillin
|
|
|
What happens if streptomycin is given during pregnancy? |
Deafness in the newborn --> contraindicated |
|
|
Gentamicin is active against which organisms? |
P.aeruginosa***, Klebsiella, proteus, Serratia, E.coli -Used in combo with penicillin (of Vancomycin) for treatment of serious enterococcal, staphylococcal, or viridian group strep infections -Strep and enterococci are relatively resistant to gentamicin due to failure of the drug to penetrate into the cell--> give with Vancomycin or penicillin -Given IV, IM, or topical, ocular or intrathecal administration -Single dose scheme better |
|
|
Amikacin |
-Same spectrum as gentamicin (more potent against P. aeruginosa) -Second line drug for MDR TB** -Resistant to many of the aminoglycoside-resistant enzymes (gentamicin, tobramycin) -Most expensive --> reserved for use against organisms that are resistant to other AGs (MDR-TB) -Nephrotoxic and ototoxic (auditory part of CN8) |
|
|
Which drugs are best for treating P.aeruginosa? |
Tobramycin > Amikacin > Gentamicin TAG |
|
|
Tobramycin |
-Almost the same antimicrobial spectrum as gentamicin, greater activity against most strains of P.aeruginosa -Ototoxic and nephrotoxic -IM, IV, and inhalation |
|
|
Paramomycin |
-Only amino glycoside which is active against Entamoeba histolytic, cryptosporidium parvum and various tapeworms (taenia solium) |
|
|
Uses of neomycin and kanamycin |
-Limited topical use (for minor soft-tissue infection often in combo with bacitracin and polymyxin) and oral use (neomycin) for hepatic encephalopathy (must kill ammonia-producing bacteria) and in prep for elective bowel surgery (along with erythromycin) -Limited use bc toxic (nephrotoxic +deafness) -Neomycin part of triple antibiotics (neomycin+bacitracin+polymyxin), ointments, dusting powders -Can be given topically as solutions on infected surfaces or injected into joints, pleural cavity, tissue spaces, or abscess cavities |
|
|
Aminoglycoside adverse effects |
-Narrow TI (monitor serum concentrations and individualize the dose depending on the creatinine clearance - renal function) -Nephrotoxic and ototoxic (more likely if given>5 days, in elderly or with renal insuff) -Neuromuscular blockade (curare-like effect) with respiration paralysis --> Caution with MG patient (decr. ACh release), enhances muscle relaxant effect -Contact dermatitis (esp. Neomycin**, topical) |
|
|
Which drugs can be used as antidotes against the neuromuscular blocking effect of amino glycosides? |
Neostigmine and calcium gluconates |
|
|
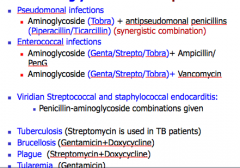
Aminoglycoside therapeutic uses |
|
|
|
What is used as an alternative treatment of GONORRHEA in patients who are either allergic to penicillins/cephalosporins or those who are infected with gonococci resistant to other drugs like penicillins, cephalosporins, fluoroquinolones (cipro)? |
SPECTINOMYCIN -Aminocyclitol antibiotic that is structurally related to aminoglycosides -Single dose of 2g, IM -Not available in USA |
|
|
Tetracyclins |
-Doxycycline -Tetracycline -Chlortetracycline -Demeclocycline -Minocycline -Oxytetracycline |
|
|
Tetracycline mechanism of action |
-Bacteriostatic antibiotics, inhibits protein synthesis -Reversible binds to the 30s subunit of the bacterial ribosome -Prevent the binding of aminoacyl-tRNA to the acceptor site (A) of the 30s ribosomal subunit, prevents addition of AAs to the grown peptide, thereby inhibiting bacterial protein synthesis |
|
|
Summary of protein synthesis inhibitors |

|
|
|
Tetracycline general info (spectrum+use)
|
BROAD spectrum - active against gram+ and gram- organisms (but due to incr. resistance and development of safer drugs, decline in use) |
|
|
Tetracyclines are used against what? |
|
|
|
Tetracyclines and macrolides |
-Macrolides mimic antimicrobial spectrum with tetracyclines -But sensitivity test is important before using one in place of another |
|
|
Tetracyclin pharmacokinetics |
-Different preps of tetracyclines differ in their absorption after oral admin and in their elimination (Minocycline and doxycycline are completely absorbed) -Oral absorption is impaired by chelation with cations (Ca, Mg, Fe, Al) and dairy foods+antacids -Excreted mainly in bile and urine
|
|
|
What is the effect of tetracycline crossing the placenta? |
Bone deformities and tooth dysplasia |
|
|
Which tetracyclines are mostly eliminated by the liver and hence require no dose reduction in renal dysfunction? |
Doxycycline and Tigecycline
|
|
|
All tetracyclines enter the CSF, but levels are insuff for therapeutic efficacy except for? |
MINOCYCLINE -Enters the brain in absence of inflammation and appears in tears and saliva -Useful in eradicating meningococcal carrier state (RIFAMPIN is preferred) |
|
|
Which oral tetracycline of choice is given twice daily band its absorption is not significantly affected by food> |
Doxycycline |
|
|
Tetracyclines are the first choice drugs for which infections? |
|
|
|
2nd uses for Tetracyclines |
|
|
|
3rd uses for Tetracyclines |
|
|
|
Which drug can be used to treat SIADH by blocking the ADH receptor in collecting ducts? |
Demeclocyclin -In the same way, a side effect of this drug is Diabetes insipidus |
|
|
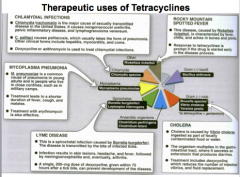
Therapeutic uses of Tetracyclines picture |
|
|
|
Adverse effects of tetracyclines |
-Most common: GI upset -Tooth enamel dysplasia and possible decr. in bone growth in children (Avoid) - chelates with Ca in tooth and bone --> brown discolouration --> enamel dysplasia (if given during pregnancy or young children), growth inhibition, deformity -Renal: Fanconi syndrome (with outdated preps-affects proximal tubule) or Diabetes insipidus (Demeclocycline) -Phototoxicity (Tetracycline, demeclocycline, doxycycline) |
|
|
Which drugs cause photo toxicity? |
Tetracycline Demeclocycline Doxycycline Sulfonamides Fluroquinolones |
|
|
Tetracycline adverse effects part 2 |
-Vestibular toxicity: reversible (Minocyclone and Doxycycline) -Hepatotoxicity (dose dependent, esp. during pregnancy and in ppl w/ pre-existing hepatic insuff and if given in high dose) |
|
|
Which tetracyclines are least hepatotoxic? |
Oxytetracycline and tetracycline |
|
|
What is the effect of tetracyclines on microflora? |
Superinfection (C.diff, P.aeruginosa, Proteus, Yeasts) is HIGHER with tetracycline that with other antibiotics -Pseudomembranous colitis |
|
|
When are tetracyclines contraindicated? |
-Pregnancy -Prepubertal children (<8YO) -Serious hepatic or renal diseases (Doxycycline can be administered in renal disease bc excreted into bile)
-Preps: oral and IV inj. , NOT IM inj (pain+inflam) |
|
|
How is resistance to tetracyclines conferred? |
Plasmid-mediated decreased intracellular accumulation of drug -EFFLUX PUMP (P-glycoprotein) -Decr. activity of uptake system |
|
|
What is the mode of action of Glycylcyclines (Tigecycline)? |
-BacterioSTATIC -Binds to the 30s ribosomal subunit and inhibit protein translocation (by blocking the entry of that aminoacyl-tRNA into the "A" site of the ribosome)
-Pharmacokinetics: Slow IV (over 30-60min), primarily eliminated by biliary/fecal excretion |
|
|
What is the antimicrobial spectrum of tigecycline? |
-MRSA -MDR S. pneumoniae -Vancomycin-resistant enterococcus -Beta-lactamase producing gram- bacteria -Actinobacter and anaerobes
Clinical uses: treatment of skin- and skin-structure infection, intra-abdominal infections, and CAP |
|
|
What is the mechanism of action of Chloramphenicol? |
Binds reversibly to the 50s ribosomal subunit and prevents peptidyltransferase enzyme from transferring the growing chain from the "P" (or"D"-donor) site to the bound charged tRNA at the "A" site. This stops protein synthesis. -Broad spectrum, bacterioSTATIC antibiotic |
|
|
What are the pharmacokinetics of chloramphenicol? |
-After oral administration, it is rapidly and completely absorbed -Chloramphenicol palmitate: prodrug, oral -Chloramphenicol succinate: prodrug, parenteral** -Distributes in most tissues and secretions; crosses BBB -Metabolized to glucuronide conjugate by the liver and excreted in urine (less dose required in liver dysfunction and neonates) -Can ANTAGONIZE bacteriCIDAL drugs such as penicillins or amino glycosides |
|
|
What are the adverse effects of chloramphenicol? |
-GI upset -Bone marrow suppression: dose dependent bone marrow suppression: APLASTIC ANEMIA, leukopenia, thrombocytopenia -Oral or vaginal candidiasis |
|
|
What causes "Grey baby syndrome"? |
Chloramphenicol -Mainly in premature neonates -Newborns lack an effective glucuronide conjugation and detox mechanism -Dose>50mg/kg/day causes vomiting, flaccidity, hypothermia, grey colour, shock, and vascular collapse |
|
|
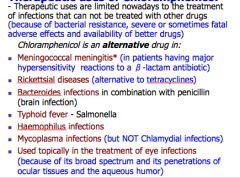
Therapeutic uses of chloramphenicol |
|
|
|
How is resistance to chloramphenicol conferred? |
-Production of an acetyltransferase capable of inactivating the drugs
|
|
|
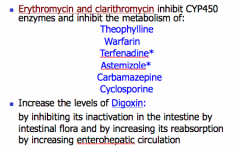
Which drug inhibits CYP450 enzymes in the liver, and prolongs the half-life of several drugs? Which drugs? |
-Chloramphenicol Prolongs half life of: -Phenytoin -Coumarins (warfarins) -Tolbutamide (causing hypoglycemia) Must decr. their dose |
|
|
What are the macrolides?
|
-Erythromycin
-Clarithromycin -Azithromycin -Roxithromycin -THROMYCINs |
|
|
What are the ketolides and what are their uses? |
Similar to macrolides -Telithromycin (similar to Azithromycin- used for CAP) |
|
|
Macrolide general features |
-Contain a LACTONE ring (usually 14-16C) to which deoxy sugars are attached -Used in patients allergic to beta-lactam antibiotics -BacterioSTATIC mainly, bactericidal at higher doses
|
|
|
Clarithromycin and Azithromycin are semi-synthetic derivatives of erythromycin and are developed to overcome which limitations of erythromycin? |
-Poor bioavailability -Frequent dosing (short half-life) -Poor GI tolerability -Limited H.influenza coverage |
|
|
What is the mechanism of action of macrolides? |
-Protein synthesis inhibitors -Irreversibly binds to 50s subunits of bacterial ribosomes and inhibits the translocation step of protein synthesis, i.e. translocation of the newly synthesized peptidyl tRNA from the acceptor site (A) to the donor site (P)
|
|
|
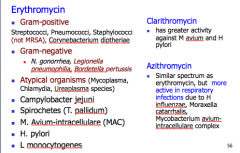
Antimicrobial spectrum of macrolides |
|
|
|
Erythromycin general features |
-ACID LABILE (Its esters are more acid stable), hence administered with enteric coating -Food interferes with absorption: Erythromycin estolate is the best absorbed oral prep -Distributes well to all body fluids EXCEPT to the brain and CSF -Diffuses into prostatic fluid and has the unique characteristic of accumulating into macrophages -Extensively metabolized, inhibits many CYP450s -Excretion is primarily in bile, hence adjustment for renal failure not necessary |
|
|
Erythromycin and Clarithromycin general features |
-Metabolized by the LIVER and excreted through the bile -Inhibit CYP450s, several drug interactions -Less tolerated in pregnancy (Clarithromycin has lower incidence of GI intolerance) |
|
|
Azithromycin general features |
-Excreted by the KIDNEY -Does NOT inhibit CYP450, free of drug interactions -MORE TOLERATED in pregnancy |
|
|
Therapeutic uses of erythromycin |
|
|
|
Clarithromycin general features |
-Derivative of erythromycin and longer half-life than erythro, permits twice daily dosing -Has improved acid stability and good absorption as compared with erythromycin -Antibact activity is almost identical to erythromycin except clarithromycin is MORE active against Mycobacterium avium complex (MAC) and H.pylori*** -Also has activity against M.Leprae, Toxoplasma gondi*, and H.influenza* -Erythromycin-resistant strep and staph are also resistant to clarithromycin |
|
|
Azithromycin general features |
-Acid stable derivative of erythro -Rapidly absorbed and well-tolerated orally (1hr before or 2 hrs after meal) -Longer half-life, permits once-daily dosing -Does NOT inhibit CYP450 -Spectrum of activity is identical to clarithromycin (but slightly less active against strep and staph compared to erythro and clarithro) -Penetrates phagocytic cells extremely well |
|
|
Azithromycin is active against what? |
-MAC, T,gondi -H.influenza *** (more active that clarithro and erythro) -Chlamydia - HIGHLY active |
|
|
When is azithromycin most commonly used? |
-CAP (pneumococcus, mycoplasma, legionella) -Pharyngitis and skin infections -Chlamydial infections (urethritis and cervicitis: single dose treatment with 1g of azithromycin is as effective as 7-day course of doxycycline for chlamydial urethritis or cervicitis) |
|
|
What is used to treat chlamydial urogenital infections during pregnancy?** |
1st line: Erythromycin 500mg 6 hourly for 7 days -Azithromycin single dose for alternative
-Chlamodyal pneumonia of infancy and ophthalmia neon atrium: use Erythromycin (tetracyclines are contra-indicated) |
|
|
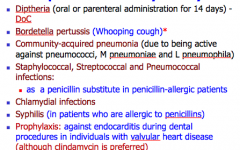
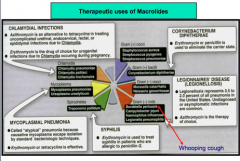
Therapeutic uses of macrolides |
|
|
|
Adverse effects of macrolides (part 1)
|
-Epigastric distress: common, moreso erythromycin (most common effect of macrocodes)
-Cholestatic jaundice with ESTOLATE form of erythromycin (fever, jaundice, impaired liver function, HSR to the estolate form) -Ototoxicity: reversible deafness at high doses |
|
|
Adverse effects of macrolides (part 2)
|
-Prokinetic action: macrolides bind with MOTILIN receptors in GIT and incr. intestinal motility (Erythro, Azithro>Clarithro)
-Prolong QT interval and arrythmias (erythromycin+cisapride or Terfenadine--> cardiotoxic drug if high dose, which it does if CYP450 inhibited) -Contradindicated: hepatic dysfunction |
|
|
Erythromycin and clarithromycin drug interactions |
|
|
|
Macrolide mechanisms of resistance development |
1. Decr. affinity of the 50s ribosomal subunit: resistance in gram+ bacteria involves production of a methylase that adds a methyl group* to the ribosomal binding site 2. Presence of plasmid associated erythromycin esterase*, that hydrolyzes macrocodes, esp. in enterobacteriacease 3. Inability to penetrate/increased efflux - shown my Gram+ organisms Cross-resistance is complete between erythromycin and other macrolides |
|
|
Clindamycin uses |
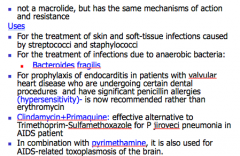
|
|
|
Adverse effects of clindamycin |
-Skin rashes -Pseudomembranous colitis***: C.diff is resistant to clindamycin -Impaired liver function and neutropenia |
|
|
Linezolid mechanism of action |
-Totally synthetic oxazolidinone antibiotic -Binds to the 50s subunit and inhibits bacterial protein synthesis by inhibiting the formation of 70s initiation complex (N-formylmethionyl-tRNA-ribosome-mRNA ternary complex) -Introduced recently to combat resistant Gram+ organisms, such as VRSA and VRE |
|
|
Linezolid therapeutic uses |
1. Vancomycin-resistant strains of S.aureus (VRSA)** 2. Vancomycin-resistant enterococcus faecium and enterococcus faecalis (VRE)** 3. Drug resistant pneumococci (nosocomial pneumonia) 4. Active against mycobacterium TB (MDR-TB) and nocardia infection |
|
|
Streptogramins: Quinupristin/Dalfopristin |
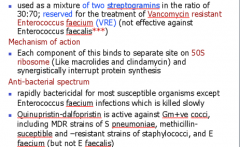
|
|
|
Folic acid synthesis inhibitors (indirect acting nucleic acid synthesis inhibitors) |
-Sulfonamides -Trimethoprim -Pyrimethamine |
|
|
Sulfonamide and trimethoprim inhibition |
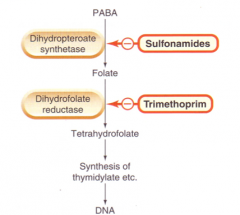
|
|
|
Sulfonamides |
-Are structural analogs of PABA -Bacteria rely on PABA for the synthesis of folic acid (Pus has high PABA, hence cannot be given with pus) -Folic acid is essential for the synthesis of purine and pyrimidines |
|
|
Sulfonamide anti-bacterial spectrum |
-BacterioSTATIC against Gram+ and Gram- (Strep pyogenes, E.coli, H.influenza, Klebsiella, Salmonella, Shigella, Enterobacter sp., Toxoplasma, P.JIROVECI, Vibrio cholera, Nocardia) -Activity is POOR against ANAerobes (P. aerugionsa is intrinsically resistant to sulphonamides) |
|
|
Sulfonamide mechanism of action |
|
|
|
Sulfonamide pharmacokinetics |
-Well absorbed from the GIT and readily penetrate CSF -Metabolized by acetylation in the liver** -Acetylated derivative is insoluble in acidic urine, hence ppt in urine and cause Crystalluria (advise patient to drink a lot of water) |
|
|
Sulfonamides of clinical interest |
Short acting: Sulfisoxazole Intermediate acting: Sulfadiazine, Sulfamethoxazole Long acting: Sulfadoxine Miscellaneous: Sulfacetamide, Sulfasalazine, Mafenide, Silver sulfadiazine (SSD) |
|
|
Sulfonamide uses |
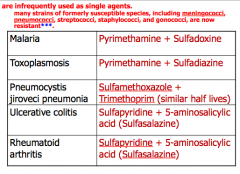
|
|
|
Sulfacetamide uses |
For eye infections (bacterial conjunctivitis and as adjunctive therapy for trachoma)- topically (ophthalmic solution or ointment) |
|
|
Mafenide uses |
Active even in the presence of pus against Pseudomonas, clostridia -Used in burn dressing -Causes burning sensation and pain -Can cause metabolic acidosis (limits its usefulness in burn patients) |
|
|
Silver sulfadiazine uses |
-Active against many bacteria and fungi- usually topical -Releases silver ions to exhibit anti-microbial action -Used in burn dressings and ulcers and preferred to mafenide for prevention of infection of burn wounds due to less toxicity |
|
|
Trimethoprim uses |
-Weak base, concentrates in prostatic fluid and in vaginal fluid, which are more acidic than plasma. Therefore, has more antibacterial activity in prostatic and vaginal fluids than many other antimicrobial drugs -Can be given alone orally in acute UTI. Many community-acquired organisms are susceptible to the high concentrations that are found in the urine. -Also in prostatitis |
|
|
Sulfonamide adverse effects |
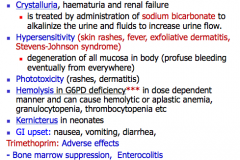
|
|
|
What is Cotrimoxazole? |
-The fixed dose combination of trimethoprim and sulfamethoxazole is called Cotrimoxazole (Combination of TRIMethoprim and sulfamethOXAZOLE) -Trimethoprim selectively inhibits bacterial dihydrofolate reductase -Cotrimoxazole causes the sequential blockade of folate metabolism |
|
|
Cotrimoxazole antibacterial spectrum and dosage |
-Spectrum includes: S.aureus, S. pneumoniae, H.influenzae, Klebsiella pneumoniae (but NOT M.pneumoniae), E.coli, Salmonella, Shigella, Toxoplasma, Pneumocystis carinii (P.jiroveci) -The dose ratio is 5:1 (S:T), leads to plasma concentration of 20:1**- for max synergy (optimal for the combined effects of these drugs in vitro) -Trimethoprim has high tissue distribution compared to sulfamethoxazole |
|
|
What is the ultimate effect of sulphonamides alone or trimethoprim alone? What is the ultimate effect of sulfonamides+trimethoprim? |
-Either alone: BacterioSTATIC -Together: BacterioCIDAL -Combo of both decreases resistance, and hence offer synergistic action by sequential blockade in folate synthesis |
|
|
Therapeutic uses of Cotrimoxazole |
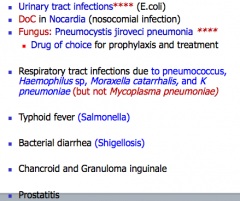
KNOW PNEUMOCYSTIS JIROVECI** |
|
|
How is sulfamethoxazole resistance acquired? |
May occur as a result of mutations that 1) cause overproduction of PABA 2) Cause production of folic-acid-synthesizing enzyme that has low affinity for sulphonamides 3) Impair permeability to the sulfonamides |
|
|
How is resistance to trimethoprim acquired? |
Results from reduced cell permeability, overproduction of dihydrofolate reductase, or production of an altered reductase with reduced drug binding* |
|
|
Direct inhibitors of nucleic acid synthesis |
Quinolones Fluoroquinolones |
|
|
What is the first member of the quinolone group? |
-Quinolones are synthetic anti-microbials which are active primarily against gram- bacteria -NALIDIXIC ACID is the first member of this group: -Active against gram- bacteria: E.coli, proteus, Klebsiella and Shigella -BacteriCIDAL, act by inhibiting bacterial DNA gyrase (topoisomerase II) -Does NOT achieve systemic antibacterial levels -High concentration in urine-lethal to urinary pathogens, hence used as urinary antiseptic and also useful in treatment of lower urinary tract infections |
|
|
Why are quinolones of minor significance today? |
-Limited therapeutic utility -Rapid development of bacterial resistance |
|
|
Adverse effects of Nalidixic acid |
-Neurological toxicity: Seizures* -Hemolysis in G6PD deficiency |
|
|
Fluoroquinolones |
-Synthetic fluorinated analogs of nalidixic acid -Have extended anti-microbial activity -BacteriCIDAL -Have CDK -Have PAE |
|
|
Fluoroquinolone variety |
-The FLOXACINS
|
|
|
Fluoroquinolone mechanism of action |
-Block bacterial DNA synthesis by inhibiting bacterial topoisomerase II (DNA gyrase) and topoisomerase IV (resp. for separation of replicated DNA during cell division) -DNA gyrase (Topo II) in bacteria required for replication in orde to remove supercoil, and even in order to introduce negative supercoil in DNA double helix -This is a required step to unwind the helix, ahead of the polymerase so that there is easier access to do replication |
|
|
What is the action of topoisomerase and how is it inhibited by fluoroquinolones? |
-Topos change the configuration or topology of DNA by a nicking, pass through, and re-sealing mechanisms -Binding of the FQs to both the enzyme (TopoII and IV) and the DNA forms a ternary complex that inhibits the resealing step, and can cause cell death by inducing cleavage of DNA |
|
|
Ciprofloxacin general features and spectrum |
-BacteriCIDAL and highly potent -Active against beta-lactam and aminoglycoside-resistant organisms Spectrum: Gram- organisms (E.coli, salmonella typhi, H.infl, N.gonorrheae, N.meningitidis, Vibrio, P.aeruginosa--> most potent FQ), gram+ strep, TB, Legionella, Brucellosis, and ANTHRAX* |
|
|
Norfloxacin |
-Least active of the FQs against both gram- and gram+ organisms, however, used in treating complicated and uncomplicated UTIs and prostatitis -Does not achieve adequate serum concentration hence not effective in systemic infections |
|
|
Trovafloxacin and Moxifloxacin |
-Not only have enhanced activity against Gram+ organisms (e.g. S.pneumoniae) but also have excellent activity against anaerobes (E.g. B.fragillis) -Although P.aeruginosa is suscp. to Trova, it is usually given with AGs -Trovafloxacin (NOT used because of liver toxicity) -Moxifloxacin- very poor activity against P.aeruginosa
|
|
|
Gatifloxacin |
Excellent activity against respiratory infections due to S.pneumoniae |
|
|
Levofloxacin |
Has superior activity against Gram+ organisms, incl. Strep Pneumo |
|
|
Pharmacokinetics of FQs |
-orally well absorbed, metabolism in LIVER -High tissue penetration- bone, prostate, and phagocytes exceeds that in plasma -FQs CHELATE Ca, Mg, Fe, and Zn -Excreted primarily in kidney by filtration and active secretion (inhibited by PROBENECID) -Reduce dose in renal dysfunction (EXCEPT Moxifloxacin) |
|
|
FQ therapeutic uses (part 1) |
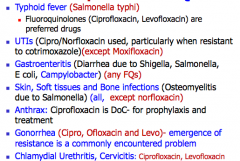
|
|
|
FQ therapeutic uses (part 2) |
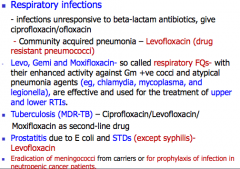
|
|
|
Adverse effects of fluoroquinolones |
-Cartilage damage, tendonitis (arthropathy)**-achilles rupture -GI distress: nausea, vomiting, diarrhea -Phototoxicity: rashes -CNS: insomnia, dizziness, headache, and seizures -QT prolonged: ALL FQs (esp. Spar and Moxi) |
|
|
FQ drug interactions |
-Plasma concentrations of theophylline, warfarin (by cipro and ofloxacin) are increased due to inhibition of metabolism of these drugs -Antacides impair absorption -NSAIDs enhance the CNS toxicity of FQs (SEIZURES are reported)- NSAIDs displace the drugs from protein-binding sites |
|
|
When are FQs contraindicated? |
-Pregnancy and in children (inhibition of chondrogenesis) |
|
|
FQ development of resistance |
-Altered target: mutations in DNA gyrase and Topo IV -Inactivation of the drug: amino glycoside acetyltransferase can also inactivate Ciprofloxacin |
|
|
Causative agents of UTIs |
-E.coli (80-95% of UTIs) -Klebseilla -Proteus -Pseudomonas -Enterococcus -Staph saprophyticus |
|
|
Antimicrobial treatment of acute uncomplicated cystitis in a non-pregnant woman |
-Cotrimoxazole (trimethoprim+sulfamethoxazole) for 3 days, as long as the local rate of resistance to cotrimoxazole among urinary pathogen is <20% -Nitrofurantoin for 5 days (eff. alternative with a low rate of E.coli resistance) -Fosfomycin (single dose) |
|
|
Antimicrobial treatment of acute uncomplicated cystitis in a pregnant woman |
-Nitrofurantoin, Amoxicillin, or cephalosporin -However, nitrofurantoin should NOT be given in the 3rd trimester or during labor and delivery due to risk of hemolytic anemia of newborn |
|
|
Which drugs have become the most common class of antibiotics prescribed for UTI, but shouldn't be used as first-line agents for EMPIRIC treatment of acute uncomplicated cystitis?** |
-FQs (esp. Ciprofloxacin) |
|
|
Antimicrobial treatment of acute uncomplicated pyelonephritis for non pregnant women |
-7-day course of Ciprofloxacin, or -5-days of Levofloxacin (if resistance to FQs aong uropathogens is <10%) -Cotrimoxazole (alternative, if uropathogens are susceptible) -2nd alternative: single IV inj. of Ceftriazone, followed by 7-14 days of an oral antimicrobial to which the patient is susceptible -Oral beta lactams are generally considered less effective for treatment of pyelonephritis than FQs or cotrimoxazole |
|
|
Antimicrobial treatment of complicated UTIs |
-Occur in patients with indwelling urinary catheters or anatomic or functional abnormalities of the urinary tract -Most likely to be caused by antibiotic-resistant gram- bacilli, S.aureus, Enterococci (incl. Vancomycin-resistant strains) -FQs (such as Ciprofloxacin or Levofloxacin)-First choice -Alternative: Cotrimoxazole, amoxicillin+Clavulanate or an oral 3rd generation cephalosporin (such as Cefinir or Ceftibuten) |
|
|
Antimicrobial treatment of hospitalized patients with complicated UTIs |
-Empiric parenteral treatment with Cefepime, Ceftriaxone, a FQ, Ticarcillin+Clavulanate, Piperacillin+Tazobactam, or a Cabapenem is generally recommended |
|
|
What are the first line drugs for TB? |
-Isonazid (INH): BacterioCIDAL -Rifampin (RIF): BacterioCIDAL -Pryazinamide (PZA): BacterioCIDAL -Ethambutol (ETH): BacterioSTATIC -Streptomycin
First 4 are the main first-line drugs. They must be given together for active TB. |
|
|
Isonazid (INH) |
-Prodrug: structural congener of pyridoxine (vitB6) M/A: -Activated by KatG **, a mycobacterial catalase-peroxidase -Activated form covalently complexes with an acyl-carrier protein (AcpM) and KasA, a beta-ketoacyl carrier protein synthetase --> blocks mycolic acid synthesis and kills the cell -Mycolic acids are unique to mycobacterium and are incorporated into a waxy sheath -Produces profound early bacteriCIDAL activity against rapidly dividing organisms |
|
|
Isonazid (INH) resistance - part 1
|
-Associated with mutations resulting in over expression of inhA, which encodes an NADH-dependent acyl carrier protein reductase
-Mutation or deletion of the katG gene -Promoter mutations resulting in overexpression of ahpC, a putative virulence gene involved in protection of the cell from oxidative stress; and mutations in kasA |
|
|
INH resistance- part 2 |
-Overproducers of inhA express low-level isonazid resistance and cross resistance to ethionamide -KatG mutants express high level isonazid resistance and often are NOT cross-resistant to ethionamide |
|
|
Adverse effects of INH |
-HEPATITS: most common (incr. enzyme elevation) -Peripheral neuropathy: slow acetylators and patients with predisposing conditions such as malnutrition, alcoholism, diabetes, AIDS, and uraemia (prophylaxis with vitB6) -SLE-like effects -CNS effects (dizziness, drowsiness, irritability) -Monoamine (histamine/tyramine poisoning) -Diarrhea -Urine color (red) -HSR |
|
|
What is used to monitor INH compliance for TB? |
-Urine color |
|
|
Rifampin** |
-Derivative of rifamycin (from Streptomyces mediterrani) -BacteriCIDAL (in vitro activity against gram+ and gram- cocci, mycobacteria, some enteric bacteria and chlamydiae)
|
|
|
Rifampin mechanism of action |
-Binds to beta subunit and inhibits bacterial DNA-dependent RNA polymerase *** -Particularly effective against rapidly growing organisms, and semi-dormant organisms |
|
|
Rifampin resistance |
Any one of several possible POINT MUTATIONS in rpoB (gene for the beta subunit of RNA polymerase) |
|
|
Rifampin adverse effects |
-Hepatotoxicity --> hepatitis -Pruritis and rash, fever, "flu-like" symptoms -Thrombocytopenia -Orange discolouration of body fluids --> permanently stain contact lens (harmless) ** |
|
|
Rifampin precautions |
-Contraindicated or use with extreme caution in HIV-infected patients, esp. those taking protease inhibitors and/or nucleotide reverse transcriptase inhibitors (use Rifabutin or rifapentine as alternative) |
|
|
Rifampin drug interactions |
-Potent ENZYME INDUCER (1A2, 2C9, 2C19, 2D6, 3A4) -->decr serum levels of oral contraceptives, WARFARIN, glucocorticoids, hypoglycemic agents, digitalis, ketoconazole, and cyclosporine
|
|
|
Rifabutin and Rifapentine** |
-Alternatives to rifampin for use in patients taking drugs susceptible to inducer metabolism e.g. HIV/AIDs* on PIs and NNRTIs |
|
|
Pryazinamide (PZA)
|
BacteriCIDAL
M/A: -inhibits mycobacterial FA synthesis by targetting FA synthase I complex -Most active against dormant and semi-dormant organisms contain w/i macrophages or the acidic environment of caseous foci |
|
|
PZA adverse effects |
-Hepatotoxicity -Hyperuricemia - Asympt: an expected effect - Acute gouty arthritis: rare (give NSAIDs) |
|
|
PZA monitoring |
-Initial serum uric acid and liver chemistry measurements |
|
|
PZA cautions/contraindications |
-Should NOT be used in patients with GOUT -Should be used with care in patients with liver disease |
|
|
Ethambutol |
-BacteriCIDAL at HIGH doses and bacterioSTATIC at low doses -Effective against rapidly growing organisms -Mainly used to prevent growth of drug -resistant organisms |
|
|
Ethambutol M/A
|
-Inhibits formation of arabinogalactan polysacc layer that binds the mycolic acid shell to the interior cell membrane of mycobacterium
|
|
|
Ethambutol adverse effects |
-Hyperuricemia- an expected effect -Retrobulbar neuritis: decr. visual acuity, missing words during reading from central scotomas (blind spots), and decr. green and red colour discrimination -Monitoring requires a visual acuity test and testing for colour discrimination (Ishawara test) as a baseline when starting the drug |
|
|
Standard treatment of active TB |
Initial phase - 2 months: Empiric 4 drug regiment until susceptibility results are available: -Isonazid -Rifampin -Pyrazinamide -Ethambutol Continuation phase: 4 to 7 months -Continue with 3 drug combo (INH, RIF and PZA); if PZA not used (liver disease? - use ETH instead) Note: with resistance, add streptomycin (if the person is sick and hospitalized) |
|
|
Recommended duration of therapy of active TB |
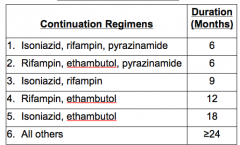
*not tested
|
|
|
Treatment of latent TB infection (LTBI) |
Standard treatment: Isonazid (is susceptible, 9 months) -Alternative: Combo: Isonazid and Rifapentine (DOT) weekly, 9 months, in a patient 12YO+ -MDR LTBI: 2 DRUGS to which the organism is susceptible (e.g pyrazinamide plus either ethambutol or a fluoroquinolone for 9-12 months) -Similar treatment for somebody who is receiving prophylactic treatment after being exposed to somebody with active TB |
|
|
Drug resistance in TB infections |
Divided into 2 types: 1. Primary resistance: causes initially infected with resistant organisms 2. Acquired resistance: develops during TB therapy
|
|
|
Multi-drug resistance TB (MDR TB) |
-TB bacteria no longer susceptible to at least isoniazid (INH) and rifampin (RIF) -More diff to treat than ordinary TB and requires up to 2 years of multi drug therapy -Use a combo of 2nd line drugs (may have more side effects, treatment may last longer, and cost may be up to 100 times more than first-line therapy) -MDR-TB strains can also grow resistant to 2nd line drugs |
|
|
Extensively drug-resistant TB (AKA XDR-TB) |
-Less common form of multi drug resistant -Resistant to INH and RIF, plus most of the alternative drugs used against MDR-TB -Any fluoroquinolone and at least one of the other 3 injectable anti-TB drugs: amikacin, kanamycin, or caprenomycin -May also be resistant to additional drugs -Most challenging to treat and needs up to 2 years of extensive drug treatment |
|
|
Mycobacteria: Resistance Mechanisms |
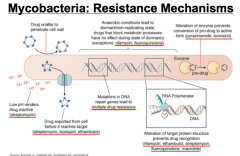
|
|
|
2nd and 3rd line anti-TB drugs |
-Aminoglycosides (Streptomycin, Amikacin, and Kanamycin) -Capreomycin -Fluoroquinolones (Levofloxacin, Moxifloxacin, Ciprofloxacin) -Thionamides (Ethionamide, Prothionamide) -Cycloserine (and Terizidone) -Para-aminosalicylic acid (PAS) |
|
|
Aminoglycosides and Capreomycin |
Aminoglycosides: -Streptomycin, amikacin, kanamycin Capreomycin (3rd line): Cyclic glycopeptide- inhibits protein synthesis M/A: Action similar to amino glycosides --> interferes with several ribosomal functions including: -Formation of 30s subunit initiation complex -Blockage of tRNA translocation from the A to the P site |
|
|
Capreomycin |
Has significant cross-resistance with viomycin, kanamycin, and neomycin Adverse effects: -Ototoxicity (subclinical hearing loss: 11%; clinical loss: 3%) -Renal: nephrotoxicity (36%), increased BUN (1-10%) -Incr. neuromuscular blocking effects of several drugs -Electrolyte disturbances |
|
|
Fluoroquinolones |
Levofloxacin, gatifloxacin, moxifloxacin M/A: Target DNA gyrase -Levofloxacin: preferred drug, esp. in patients with drug resistant TB Adverse effects of levofloxacin: -GI (nausea and bloating) -Cutaneous (rash and photosensitivity) -Neurological (dizziness and insomnia)- very uncommon -Fluoroquinolones should be given at least 2 hours before or after antacids, and/or other medications containing divalent cations |
|
|
Thionamides
|
Ethionamide and Prothionamide (related to INH)
M/A: Inhibit mycolic acid synthesis -Will have cross-resistance with INH if via inhA mutation -Poorly tolerated due to GI upset Side effects: -Hepatotoxicity , neuropathy (give B6) -HYPOTHYROIDISM |
|
|
Cycloserine
|
-Analog of D-alanine -BacterioSTATIC -No cross-resistance with other anti-TB drugs -Widely distributed in tissues and body fluids: CSF penetration (80-100% of serum concentration), higher if meninges inflamed -Additive nervous system side-effects (psychiatric and seizures) with Ethionamide and Isonazid -May incr. levels; combo with alcohol, incr. risk of seizures -VitB6 decreases CNS adverse effects |
|
|
Para-Aminosalicylic Acid (PAS) - M/A and side effects |
MoA: Folate synthesis antagonist - effective drug -Widely used in 50s and 60s (INH+SM+PAS) Side effects: -GI symptoms universal (NV); hepatotoxicity (hepatitis) -Malabsorption (steatorrhea and low folate levels) -Can indue hypothyroidism -Coagulopathy (doubles the prothrombin time) -Monitor with baseline liver function and TSH levels every 3 months |
|
|
Drugs for Leprosy |
-Clofazamine -Dapsone -Rifampin
Objectives: -interrupt transmission of leprosy by sterilizing infectious patients as rapidly as possible with bacterioCIDAL drugs -Ensure early detection and treatment of cases to prevent deformities -Prevent drug resistance - never use single drug |
|
|
Multi-drug therapy (MDT) drugs for Leprosy |
-Combination of rifampin, clofazamine, and dapsone for multibacillary (MB) patients -Combination of rifampin and damson is used for paucibacillary (PB) patients -Ethionamide and prothionamide (more expensive than other drugs --> used when clofazamine cannot be used --> quinolones and minoclycline) |
|
|
Rifampin |
-Only drug highly bacteriCIDAL against M.Leprae -Given once/month (big advantage) -Turns urine RED (warn patient)
|
|
|
Dapsone |
-Cheap and effective -Weakly bactericidal against M.leprae -Common side effects: Hemolytic anemia, hepatitis and neuropathy, agranulocytosis -Can cause dapsone-syndrome (fever, enlarged lymph nodes, exfoliative dermatitis, hepatitis, and maculo-papular rash has also been reported) --> potentially fatal -Prescribe iron routinely with dapsone |
|
|
Clofazamine |
-Originally designed for treatment of TB but found to be more useful in Leprosy -Has anti-leprosy and anti-inflammatory properties --> suppresses and prevents reactions |
|
|
Clofazamine mode of action |
-Binds to bacterial DNA guanine bases --> blocks template function of DNA --> BacterioCIDAL -Incr. release of bacterial phospholipase A2 --> release and accumulation of lysophospholipids which are toxic to bacteria |
|
|
Adverse effect of Clofazamine |
Darkens skin color
|
|
|
Ofloxacin |
-Fluoroquinolone effective in leprosy, side effects are rare and generally mild
|
|
|
Minocycline |
Moderately active against leprosy at 100mg QD |
|
|
Anti-viral strategies |
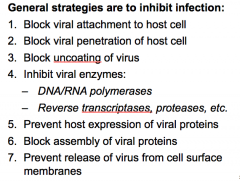
|
|
|
Drugs active against Herpes Virus (Varicella Zoster and Herpes Simplex) |
-Acyclovir/Valacyclovir -Famciclovir/Penciclovir -Ganciclovir/Valganciclovir -Foscarnet -Adefovir -Cidofovir
Other causes: Adenovirus, enterovirus, cidofovir, pleconaril |
|
|
Drugs for HSV infections |
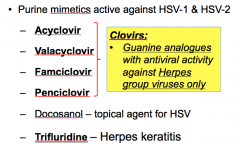
|
|
|
Acyclovir mechanism of action |
-Sequentially activated first by viral thymidine kinase, then by host cellular kinase (2 steps) to triphosphate form (acyclovir-TP) -Triphosphate competes with dGTP for viral DNA polymerase --> incorporated into viral DNA by binding to DNA template and terminating chain elongation |
|
|
Acyclovir mechanism of action (2) |
Activation through 3 phosphorylation steps, first to monophosphate -Requires viral kinase -Viral kinase requirement provides selectivity for infected cells -Selected activation results in triphosphate accumulation only in infected cells -Acyclovir triphosphate accumulates in infected cells and inhibits viral DNA synthesis |
|
|
Acyclovir M/A picture |
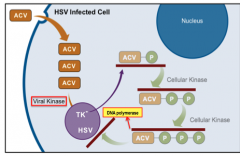
|
|
|
Resistance to Acyclovir |
-Mutation in viral thymidine kinase -Also alteration of DNA polymerase - less important |
|
|
Acyclovir acts against which viruses? |
-HSV1 and HSV2 treatment and prophylaxis -Varicella (VZV), Epstein Barr (EBV) -HSV1> HSV2>VZV=EBV -CMV is practically resistant |
|
|
Acyclovir pharmacokinetics |
-Acyclovir has poor oral absorption (15-30%) -Cleared primarily by glomerular filtration and tubular secretion -t1/2 varies enormously dependent on renal function -Drug tissue levels vary from 50 to 100 % of serum levels |
|
|
Acyclovir indications |
-Genital herpes (HSV2) -Mucocutaneous herpes (HSV1): remains localized to lips and gums -H. simplex encephalitis (HSV1) -H.simplex keratitis (HSV1): good corneal penetration -Herpes zoster (VZV): Shingles, adults -Chicken pox (VZV): children |
|
|
Adverse reactions of Acyclovir |
Generally few -Most frequently toxicity (if renal dysfunction) Occasional: -GIT: nausea, vomiting, diarrhea -CNS: tremor, lethargy |
|
|
How is acyclovir given? Side effects? |
IV administration -Infusion site phlebitis/inflammation infection (or extravasation) -Reversible kidney dysfunction due to crystalline nephropathy (risk by rapid infusion, dehydration, high dosage, renal insuff) |
|
|
What are the other clovirs? |
Primarily PRO-DRUGS -Valacyclovir: Prodrug metabolized to acyclovir (prolonged release of acyclovir) -Famciclovir: Prodrug metbaolized to Penclovir |
|
|
Penclovir |
-Not absorbed orally but similar activity to acyclovir when given by IV route -Not chain-terminating but achieves higher intracellular levels than acyclovir -Not available commercially for IV use |
|
|
Acyclovir resistance |
In HSV and VZV: -Alteration in viral thymidine kinase -DNA polymerase mutation -Def. in thymidine kinase activity (cross resistance with valacyclovir, famciclovir, penciclovir, and ganciclovir) -Resistant HSV infections in HIV-positive patients associated with: chronic cutaneous lesions and invasive disease (rarely) |
|
|
Foscarnet |
A tri-sodium salt of phosphonoformate (inorganic pyrophosphate)
|
|
|
Foscarnet mechanism of action |
-Specifically inhibits viral DNA polymerase, RNA polymerase, and HIV reverse transcriptase by competing for the PP binding site
|
|
|
Indications of use for Foscarnet |
-Drug of choice for acyclovir resistant HSV or VZV infections -Immunocompromised patients with CMV retinitis and mucocutaneous acyclovir-resistant HSV infections -Alternative drug for CMV retinitisF |
|
|
Foscarnet side effects |
Renal impairment (the major toxicity) --> hypokalemia and hypomagnesemia |
|
|
Anti-herpes group drugs |
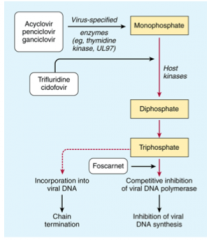
|
|
|
Anti-herpes virus drugs (Table) |
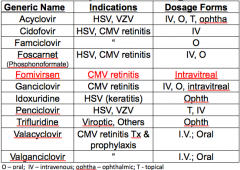
|
|
|
Drugs for CMV infection |
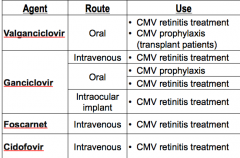
|
|
|
Influenza virus picture |
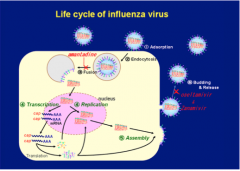
|
|
|
Which drugs are active only against Influenza A? |
Amantadine Rimantadine |
|
|
Which drugs are active against both Influenza A and B? |
Oseltamivir Zanamivir |
|
|
Amantadine and Rimantadine mechanism of action |
Prevent uncoating of Influenza A by binding M2 protein -Appear to be viruSTATIC by preventing uncoating of virus particle -Affect maturation of Influenza HA glycoprotein in trans-golgi network Note: NOT active against Infl. B (No M2 protein) -Resistance is high, not currently recommended to treatment |
|
|
Amantadine and Rimantadine resistance |
-Fairly common, 2ndary to mutations of the M-2 protein (e.g. associated with adding it to ANIMAL FEED)A |
|
|
Amantadine and Rimantadine uses |
Prophylaxis and early treatment of Infl. A |
|
|
Amantadine and Rimantadine toxicity |
-GI: nausea -CNS: lightheadedness, insomnia (5-33%) (Amantadine>Rimantadine, occur more commonly in elderly) |
|
|
Oseltamavir and Zanamivir mechanism of action
|
-Selectively inhibit viral neuraminidases of infl. A and B, incl. H1N1 and H5Na --> prevent virion release
|
|
|
Oseltamavir and Zanamivir resistance |
-Results from viral neuraminidase mutations (~1% of adults and 4% of children) |
|
|
Oseltamivir |
-Pro-drug activated in the LIVER -Used for prophylaxis and early treatment -Oseltamivir toxicity: GI -Zanamivir toxicity: bronchospasm |
|
|
Schematic representation of influenza virus attachment, internalization, replication and exit from the host respiratory cell and steps inhibited by antiviral drugs |

|
|
|
Drugs active against hepatitis virus
|
-Interferons
-Ribavirin -Lamivudine -Adefovir -Entecavir -Telbivudine -Tenofovir -Telaprivir -Boceprevir |
|
|
Interferons |
-Group of proteins produced naturally by cells in the immune system after exposure to viruses General classes of interferons: alpha, beta, gamma -Secreted by diff types of cells -Administration by parenteral routes only (IM, SQ, topical-nasal spray)
|
|
|
Interferon |
BROAD spectrum anti-viral activity DNA viruses: -HSV 1 and 2 -Herpes zoster -HPV (genital warts) -Chronic hepatitis B and C RNA viruses: -influenza, common cold -Chronic hepatits B and C -Also used for breast cancer, lung cancer, Kaposi sarcoma (AIDs-associated cancer) |
|
|
Interferon mechanism of action |
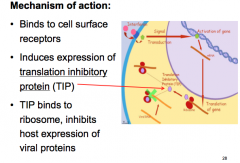
|
|
|
Interferon adverse effects |
-Flu-like symptoms (headache, fatigue or asthenia, myalgia, arthralgia, fever, chills) -Neuropsychiatric: depression, emotional liability, insomnia -Alopecia -Thyroiditis: can unmask or exacerbate; IFN-induced disease may not be reversible after stopping treatment |
|
|
Interferon indications |
HepB: -HBeAg+ carriers with chronic active hepatitis -Response rate: 30-40% HepC: -Interferon may be considered for chronic active hepatitis -Response rate is around 50% but 50% of responders will relapse upon withdrawal of treatment |
|
|
Lamivudine |
-Nucleoside analog -Inhibits HBV DNA polymerase -Also inhibits HIV reverse transcriptase -Well tolerated, most patients will respond favorably -Tendency to relapse on cessation of treatment -Rapid emergence of drug resistance |
|
|
Adefovir |
-Adefovir dipivoxil-adenin nucleotide analog phosphorylated by cellular kinases to active diphosphate metabolite --> competitively inhibits HBV DNA polymerase and causes chain termination after incorporation into viral DNA -In vitro activity against a wide range of DNA and RNA viruses, incl. HBV, HIV, and herpesvirus -Less likely to develop resistant than lamuvidine -May be used to treat lamivudine-resistant HBV -More expensive and toxic |
|
|
Entecavir |
-Guanosine nucleoside analog -Powerful antiviral similar to Adefovir -Successful response to treatment will result in the disappearance of HBsAg, HBV-DNA and seroconversion to HBeAg
|
|
|
Entecavir mechanism of action |
-Competitively inhibits all 3 functions of HBV: DNA polymerase, incl. base priming, reverse transcription of the negative strand and synthesis of the positive strand of HBV DNA -Oral bioavailability ~100% |
|
|
Drugs used to treat viral Hepatitis B |
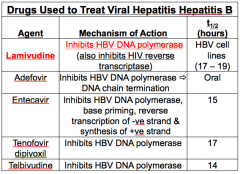
|
|
|
Hepatitis B drug summary |
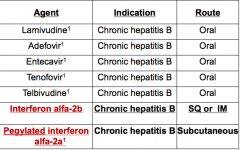
|
|
|
Drugs used to treat viral HepC interferons and ribavirin |
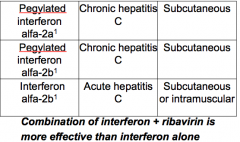
|
|
|
Ribavirin (for Hep C) |
-Guanosine analog phosphorylated by host cell enzymes to active drug -Used in combo with interferon and ribavirin |
|
|
Ribavirin mechanism of action |
-Interferes with synthesis of GTP; inhibits viral RNA-dependent DNA polymerase and capping of viral mRNA -Triphosphate inhibits replication of a wide range of DNA and RNA viruses, incl. Influenza A and B, parainfluenza, RSV, paramyxovirus, HCV, and HIV1 |
|
|
Antiviral treatment summary |
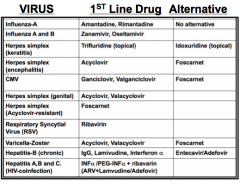
|
|
|
Summary of antiviral targets |
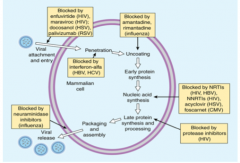
|
|
|
HIV structure |
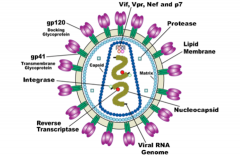
|
|
|
HIV enzymes |
It is and RNA retrovirus with two major strains (HIV-1 and -2) -Reverse transcriptase: converts HIV RNA genome into a DNA copy -Integrase: Inserts the HIV DNA copy into the host genome -Protease: cleaves and processes immature HIV proteins into mature, functioning proteins |
|
|
HIV infection and replication process |

|
|
|
HIV clinical course summary |
1. Viral transmission 2. Primary HIV infection 3. Sero-conversion: Ab development after 6-8 weeks 4. Asymptomatic chronic infection with or without persistent generalized lymphadenopathy 5. Symptomatic HIV infection 6. AIDS (presence of AIDS indicator conditions or CD4 cell count <200/mL) 7. Advanced HIV infection (CD4 cell count < 50/mL) |
|
|
Opportunistic infections gained by weakened immunity |
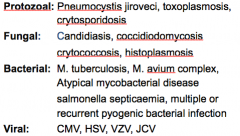
|
|
|
Pathophysiology of HIV infection |
-AIDS now defined as CD4 count <200/mL -Infected and untreated people develop S&S typical of HIV infection (AIDS-related infections and cancers) -Infections acquired as CD4 counts decrease are common with CD4 counts below 350/mL -HSV infections with lesions in mouth or genitals and occurring more frequently and more severely than previously |
|
|
Infections common in those with HIV |
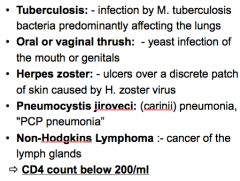
|
|
|
HIV/AIDS disease progression (markers) *note timeline |
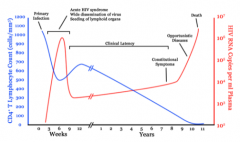
|
|
|
At what viral load do we start to treat somebody with HIV? |
500CD4/mL |
|
|
Goals of therapy and treatment approach for HIV |
Pharmacological goals are to: -Maximally and durably suppress HIV viral load -Restore and preserve immunologic function Treatment approach: -Current recommendation for primary therapy is to administer 2 NRTIs+ either a protease inhibitor or an NNRTI |
|
|
Prior to Zidovudine, what was the focus of treatment for HIV? |
Decreasing occurrence of opportunistic infections that caused a high degree of morbidity and mortality in AIDs patients |
|
|
What is the plan of treatment for those with HIV? |
-Highly active regimen (combo drugs) is used to suppress HIV replication and restore the number of CD4 cells and immunocompetence -5 classes of antiretroviral drugs, each of which targets one of four viral processes |
|
|
5 HIV drug classes |
1. Entry (fusion) inhibitors 2. Integrase inhibitor 3. Nucleoside and Nucleotide reverse transcriptase inhibitors (NRTIs) 4. Non-nucleoside reverse transcriptase inhibitors (NNRTIs) 5. Protease inhibitors |
|
|
What are the several key proteins involved in HIV entry into cells? |
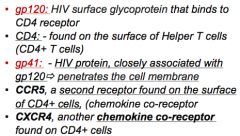
|
|
|
What is the small peptide entry inhibitor available in injectable form only? |
Enfuviritide Mechanism of action: -Mimics the components of the HIV-1 fusion machinery and displaces them, preventing GP120 from deforming to allow the viral protein GP41 to embed itself into the host cell's plasma membrane -Expensive -Used as a reserve for "salvage" therapy in patients with multi-drug resistant HIV |
|
|
What are the side effects of Enfuviritide? |
-Injection site reactions (COMMON) -HSR (uncommon) -Eosinophilia -Increased risk of pneumonia on Phase III studies |
|
|
How is resistance to enfuviritide acquired? |
-Changes in gp41 |
|
|
Which entry inhibitor interferes with binding of HIV to CD4+ receptors and chemokine co-receptors? |
Maraviroc Mechanism of action: -Blocks the chemokine receptor CCR5 -Because HIV can also use another co-receptor, CXCR4, and HIV tropism test such as trofile assay must be performed to determine if the drug will be effective |
|
|
What are the reverse transcriptase inhibitors? |
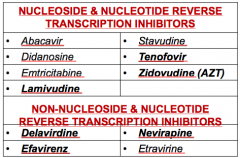
|
|
|
What are Nucleoside Reverse Transcriptase Inhibitors? What is the difference with nucleotide variants? |
Inactive drugs PHOSPHORYLATED to active metabolites that compete with endogenous nucleosides for incorporation into viral DNA -Competitively inhibit HIV reverse transcriptase and terminate synthesis of DNA chains (Nucleotides are the same thing but do NOT require phosphorylation) |
|
|
NRTIs Mechanism of Action: Nucleoside analogs (e.g. AZT) |
-Analogs of thymidine, cytosine, adenine, or guanine -Tri-phosphorylated inside the cells to the active compound -Incorporated into the growing HIV viral DNA strand by reverse transcriptase -When administered as a single anti-retroviral anent, HIV rapidly develops resistance |
|
|
NRTIs Mechanism of Action: Nucleotide analogs (e.g. Tenofovir (TDF)) |
-Do NOT need to be tri-phosphorylated, only di-phosphorylated to active compound |
|
|
Zidovudine (AZT or Azidothymidine) |
-Sometimes co-formulated with Lamivudine -Active orally, widely distributed -Hepatic metabolism, renal excretion -Used to prevent vertical transmission of HIV from mother to child (HAART is preferred in pregnant women and is very effective in preventing resistance) -Resistance via reverse transcriptase inhibitors -High grade resistance requires serial multiple mutations (hence, overcome by increasing the dose) -First line NRTI in paediatric patients and pregnancy * |
|
|
What are the adverse effects of Zidovudine? |
-Bone marrow suppression -GI complaints -CNS: headaches, insomnia, peripheral neuropathy -Mitochondrial toxicity, myalgia, myopathy, cardiomyopathy -Lactic acidosis*: severe and can be fatal -Cholestatic hepatitis, lipodystrophy -NOT tertatogenic, can be started as early as 14 weeks gestation |
|
|
Lactic acidosis caused by Zidovudine |
-Damage to mitochondria in cells -Elevated lactate, low pH/bicarb, N/V, SOB, if untreated can lead to death |
|
|
Hepatomegaly with steatosis caused by Zidovudine |
-Build up of fat droplets inside liver cells -Enlarged liver |
|
|
NRTIs: Agent-specific side effects (part 1) |
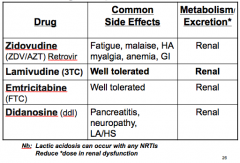
|
|
|
NRTIs: Agent-specific side effects (part 2) |
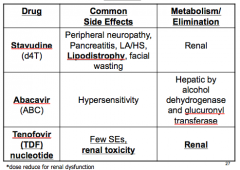
|
|
|
NRTI combinations |
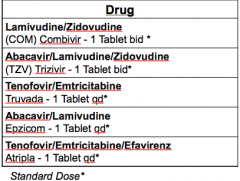
-Combivir is first choice, Trizivir is alternative -1 tablet helps with compliance and resistance |
|
|
NNRTI mechanism of action |
-Directly bind to reverse transcriptase to inhibit transcription -NNRTIs do not require phosphorylation to be active
|
|
|
HIV drugs and location of effect picture |
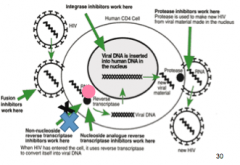
|
|
|
NNRTIs |
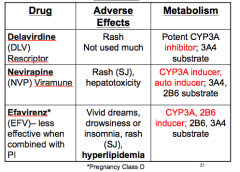
|
|
|
What do NNRTIs and Rifampin have in common? |
CYP3A4 inducers!! So cannot treat TB and HIV with these at the same time, or risk compromising treatment as a whole |
|
|
Protease inhibitors |
Viral protease gene encode viral enzyme which cleave polyprotein into core structural proteins -Protease inhibitors are designed to block active site of viral protease -Generally, used in combo with NRTIs and NNRTIs -Resistance due to protease gene mutations -High grade resistance requires serial, multiple mutations |
|
|
What is a protease inhibitor for HIV and a potent cytochrome P450 inhibitor? |
RITONAVIR -First line drug when combined with other PIs (Lopinavir) -Low doses will "boost" serum levels and half lives of other Protease inhibitors --> allows use of lower doses and reduce toxicity -Good availability but TASTES BAD |
|
|
What are the adverse effects of Ritonavir? |
-Common when used in FULL dose -GI, esp. taste sensation -Hypertriglyceridemia -Rare paresthesias -multiple drug interactions (inhibits p450) |
|
|
What is the most potent protease inhibitor (HIV)? |
LOPINAVIR (LPV) -Co-formulated with Ritonavir in order to take advantage of P450 inhibition by Ritonavir, increases antiviral effect of LPV -Well tolerated with some GI toxicity and hyperlipidemia -1st line when combined with ritonavir |
|
|
What is a protease inhibitor that contains a sulphonamide moiety (HIV)? |
FOSAMPRENAVIR (FPV) and DARUNAVIR -1st line when combined with ritonavir -Therapeutic failure when used "unboosted" |
|
|
What are the adverse effects of Fosamprenavir and Darunavir (protease inhibitors - HIV)? |
-Stevens-Johnson syndrome -Headache -Fosamprenavir: transaminase elevation, hyperglycemia and hyperlipidemia -Darunavir: GI and metabolic disturbances |
|
|
What is a protease inhibitor that is sensitive to gastric pH (HIV)? |
Atazanavir (ATV) -1st line drug when combined with ritonavir
|
|
|
Atazanavir (protease inhibitor-HIV) toxicity |
-Cardiac, hyperlipidemia, nephrolithiasis -NOT to be used with NVP -Inhibits cytochrome enzymes --> drug-drug interactions |
|
|
What is HAART and what is the selection of appropriate drugs for combinations based on? |
Highly active anti-retroviral therapy 1. Avoiding the use of 2 agents of the same nucleoside analog 2. Avoiding overlapping toxicities and genotypic and phenotypic characteristics of the virus 3. Patients factors, e.g. disease symptoms and concurrent illnesses 4. Impact of drug interactions 5. Ease of adherence to complex regimen |
|
|
Drugs for HIV: combinations |
Rationale: delay resistance -2 nucleoside/-tide reverse transcriptase inhibitors + 1 protease inhibitor +/- ritonavir -2 NRTI + 1NNRT |
|
|
Summary: sites of action of anti-HIV drugs |

|
|
|
What are the major invasive fungal organisms? |
1. Candida 2. Aspergillus 3. Blastomyces 4. Coccidioides 5. Cryptococcus 6. Histoplasma 7. Zygomycosis (Mucor) 8. Sporotrix |
|
|
What leads to increased susceptibility to fungal infections? |
1. Immunosuppressive disease (congenital or acquired) 2. Immunosuppressive therapy (Cancer, HIV/AIDs, organ transplant) 3. Use of broad-spectrum antibiotics 4. IN-DWELLING CATHETERS |
|
|
Classification of anti-fungal drugs |
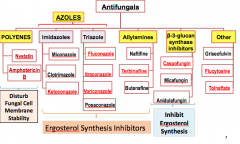
|
|
|
What is the mechanism of action of polyenes? |
-Binds to ergosterol in the fungal cell membranes, forms pores, and increases the permeability to proteins and monovalent ions, esp. K+ and divalent cations -Eventually leads to cell death -Polyenes attach with higher affinity to ergosterol-containing membranes than cholesterol-containing ones (i.e. mammalian) |
|
|
What are the adverse effects of polyenes? |
AmphoB may also induce oxidative damage in fungal cells and has been reported to stimulate host immune cells -Causes the release of inflammatory cytokines by circulating monocytes, resulting in fever, chills, rigour, nausea, vomiting, myalgias, arthralgias, and headache during IV infusions -At higher concentrations, amphoB binds to cholesterol in mammalian cell membranes, leading to various organ toxicities, esp. nephrotoxicity |
|
|
What are the indications for Amphotericin B? |
-Systemic mycotic infections including aspergilliosis, blastomycosis, and coccidomycosis -Nephrotoxicity may occur when given in high doses -HYPOKALEMIA might occur (pregnancy category B) |
|
|
Amphotericin B spectrum of activity |
-BROAD spectrum antifungal -Active against most holds and yeasts -Holes: C. lusitanae, fusarium, Tricosporon, Scedosporium |
|
|
AmphoB activity spectrum picture |
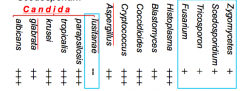
|
|
|
AmphoB resistance mechanisms |
-Resistance in a previously susceptible species is uncommon -Leads to reductions in ergosterol biosynthesis -Synthesis of alternative sterols that lessen the ability of AmphoB to interact with the fungal membrane |
|
|
Which polyene increases fungal cell membrane permeability and is only good for candida infections? |
NYSTATIN -Topical, GI, GU drug only -Oral, intestinal, and vaginal candidiasis S/E: -PO: anorexia, MD (large doses), stomach cramps, rash -Vaginal: Rash, burning sensation Contraindications: HSR, pregnancy (vaginal) |
|
|
Which anti-fungal inhibits ergosterol synthesis by inhibiting CYP-450-dependent lanosterol 14-alpha demethylase? |
AZOLE -Leads to depletion of ergosterol in fungal cell membrane -Impair fungal ATPase function -Broad spectrum activity: Candida, cryptococcus, blastomyces, histoplasma, coccidiodes, dermatophytes |
|
|
Fluconazole |
-Low molecular weight and high water solubility, leading to rapid absorption and high bioavailability -Effectively penetrates the CSF, brain and eyes (50-90% plasma levels) ->90% renal excretion S/E: -Very well tolerated, even up to 1600 mg/day -GI, reversible transaminase elevation Advantage: IV and oral interchangeable (>90% bioavailability), azole of choice for treatment and 2nd prophylaxis of cryptococcal meningitis |
|
|
Which azole is fungicidal in vitro against ASPERGILLUS? |
VORICONAZOLE -Also fungicidal for scedosporium, and fusarium spp. -Fungistatic in vitro against Canadida spp. Indications: -Invasive aspergillosis, esophageal candidiasis -Fungal infections caused by Scedosporium and fusarium spp. in patients intolerant of or refractory to other therapy
|
|
|
What are the adverse effects of Voriconazole? |
-Visual disturbances: decr. electrical currents in the retina -Incr. liver function tests, skin reacions |
|
|
Which azole tends to inhibit mammalian CYT P450 enzymes and are less selective for fungal P450 than newer azoles? |
KETOCONAZOLE (no longer used much in USA) -Inhibits mammalian steroid synthesis (cortisol, testosterone --> gynecomastia) Drug interactions: Serum levels DECREASED by Rifampin (used for TB) and other inducers |
|
|
Itraconazole |
-Only ionized at low pH, leading to wide inter patient variability in plasma concentrations -nonlinear serum PK -Extensively metabolized in the liver* Adverse effects: -Hepatotoxicity (~5%), negative inotrope (decr. heart contractility) Drug interactions: -Substrate and inhibitor of CYP3A4 -NB also affects and affected by the enzyme inducers - rifampin, phenytoin, phenobarbital |
|
|
Itroconazole spectrum of activity |
-Paracoccidiomycosis -Blastomycosis -Histoplasmosis -Sporotrichosis -Cutaneous and mucosal candiasis -Aspergillosis |
|
|
Azole antifungal spectrum of activity |
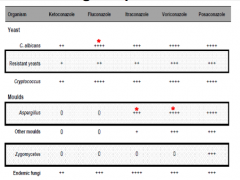
|
|
|
Which anti-fungal drug inhibits squalene2,3-epoxidase? |
ALLYAMINES (Terfinafine, nafitifine, amorolfine, butenafine) -Effective against dermatophytes (aspergillus sp., and candida and pityrosporum yeasts) - Fungistatic against Candida but can cure in after 2-4 weeks -Inhibition of the epoxidase leads to the accumulation of squalene (toxic/cidal to sensitive organism) -Used ORALLY for dermatophytes |
|
|
Which anti-fungal drug is extensively distributed to the hair follicle, nail plate, and sebum rich skin and can be detected in the nail clippings three weeks after the initiation of therapy? |
TERBINAFINE (Allyamine) -Well absorbed from GIT -Metabolized then excreted in urine S/E: -Alcohol and hepatotoxic medications may increase risk of liver damage -Potentiates the effects of caffeine and theophylline |
|
|
Terbinafine drug interactions |
Substrate of CYP1A2, 2C9/19, and 3A4 -Cimetidine decr. clearance by 33% -Rifampin incr, clearance by 100% (avoid combo) Strong inhibitor of CYP-2D6 -Increase levels or t1/2 or Cmax of tricyclic antidepressants (TCAs, e.g. notriptyline, amitriptyline, desipramine) -Avoid combo or adjust dosages |
|
|
Which fungistatic anti-fungal is a pro-drug deaminated to 5-fluoroacil (5-FU)? |
FLUCYTOSINE (5-FC) -Incorporated into RNA and disrupts protein synthesis -Resistance develops during therapy, esp. monotherapy -Single point mutation leading to loss of permease necessary for cytosine transport -Decr. activity of UMP phosphorylase or cytosine deaminase -Incr. synthesis of pyrimidines which compete for 5-FU metabolites, leading to decreased antimycotic activity
|
|
|
Flucytosine Mechanism of Action |
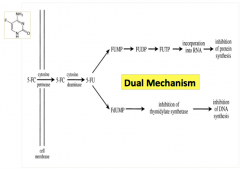
|
|
|
What is the spectrum of activity of Flucytosine (5-FC)? |
Cryptococcus neoformans* -Candida spp. (except C.kusei) -Little to no activity against Aspergillus sp. and other molds Pharmacokinetics: ORAL DOSING ONLY -Distribution: CSF levels (75%) Elimination: 90% excreted via GFR, t1/2 is 6 hours, adjust dose in RF |
|
|
Adverse effects of flu cytosine (5-FU) |
-Dose-dependent bone marrow suppression (decr. WBC, decr. platelets) -GI: nausea/vomiting/diarrhea
|
|
|
Flucytosine clinical uses |
-Cryptococcal meningitis, hepatosplenic candiasis, candida endophthalmitis -Used in COMBO ONLY (usually with Amphotericin B, ampho potentiates uptake, minimizes development of resistance) |
|
|
Which fungistatic drug is mostly used topically and disrupts fungal mitotic spindles and inhibits mitosis? |
GRISEOFULVIN -Used for microsporum, epidermophyton, trichophytons (tinea capitis, corporis, and cruris), athletes foot S/E: -Headache (15%), peripheral neuropathy, confusion -Antabuse (disulfiram-like) reactions -Photosensitivity and drug interactions |
|
|
Griseofulvin |
-Hepatic metabolism -Weak inducers of CYPs 1A2, 2C9, 3A4 -Decreased effectiveness of cyclosporine (dec. 40%), estrogens, warfarin -Monitor effectiveness of treatment -Phenobarbital and omeprazole decreased absorption (may require increase in dose) -Theophylline dose reduction when administered together |
|
|
Which group of antifungals irreversibly inhibit Beta-1,3-D glucan synthesis (enzyme complex that forms glucan polymers in the fungal cell wall) |
Echinocandins : Caspfungin, micafungin, anidulafungin -Glucan polymers provide rigidity to cell wall, leading to disruption of beta-1,3-D glucan synthesis and reduced cell wall integrity, cell rupture, and cell death |
|
|
Spectrum of activity of Echinocandins |
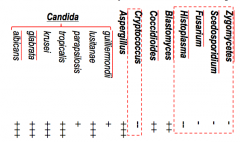
|
|
|
Anti-fungals summary (part 1) |
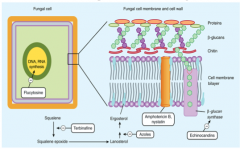
|
|
|
Anti-fungals summary (part 2) |

|
|
|
What is the most severe form of Malaria and can be fatal (accounts for up to 80-90% of deaths)? |
Plasmodium falciparum -Can infect RBCs of ALL ages, resulting in high levels of parasitemia -End-organ disease may develop rapidly specifically involving CNS, lungs, and kidneys leading to hypoglycaemia, lactic acidosis, severe anemia, and multi-organ dysfunction due to hypoxia |
|
|
Symptoms of malaria |
-Flu-like illness with moderate to severe shaking/chills -High fever, headache, muscle aches and tiredness -Profuse sweating as body temp falls -Nausea, vomiting, and diarrhea -Anemia and jaundice -Chills, fever, headache, anemia P.falciparum: if not treated, can cause kidney failure, seizures, mental confusion, coma, and death |
|
|
Which malarial parasite can cause a severe form of disease similar to falciparum? |
P. knowlesi |
|
|
Which malarial parasites only infect YOUNG RBCs? |
P. vivax and P.ovale -Benign TERTIAN fever, every 3rd day -Have exo-ertythrocytic stage |
|
|
Which malarial parasite is a quartan malaria (only every 4th day) with NO EXO-ERYTHROCYTIC STAGE? |
P. Malariae |
|
|
Malaria infective cycle |
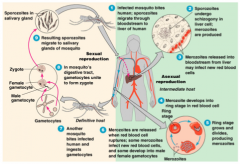
|
|
|
What are the 4-aminoquinolone derivatives of anti-malarials? |
-Hydroxychloroquine -Chloroquine -Quinine and quinidine -Mefloquine |
|
|
What are the 8-aminoquinolone derivatives of antimalarials? |
Primaquine |
|
|
What are the atermisinins of antimalarials? |
Artesunate Artemether |
|
|
What are the sulfones and sulphonamide of antimalarials? |
-Sulfadiazine -Dapsone |
|
|
What are the dihydrofolate reductase inhibitors of antimalarials? |
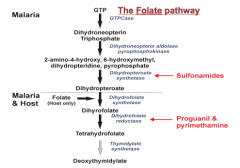
-Chloroguanide, Pyrimethamine, Trimethoprim |
|
|
Which 2 antibiotics are used against malaria? |
Tetracyclines Doxycycline |
|
|
What are common drug combinations used against malaria? |
-Pyrimethamine and sulfadioxine --> fansidar -Pyrimethamine and dapsone --> maloprim -Halofrantrine- N/A in USA;/Lamifantrine (in Coartem) |
|
|
What is the drug classification of antimalarials? |
Classification based on selective actions of drugs on different phases of the parasite life cycle 1. Tissue schizonticides: Eliminate developing or dormant (hypnozoites) liver forms 2. Blood schizonticides: Act on erythrocytic parasites 3. Gametocides: Kill sexual stages and prevent transmission to mosquitoes NB: No ONE available agent can reliably effect a RADICAL CURE |
|
|
Which synthetic 4-aminoquinoline anti-malarial is formulated as the phosphate salt for oral use? |
CHLOROQUINE -Plasmodium accumulate chloroquine in food vaculoes -Drug is incorporated into the DNA chain of plasmodium - inhibits proliferation -Prevents the polymerization of hemoglobin breakdown product (heme) into hemozoin --> buildup of free heme toxic toparasite -Increases the cellular pH --> decreases plasmodium protease activity |
|
|
Chloroquine mechanism (malaria) |
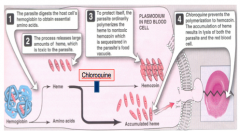
|
|
|
How is resistant to chloroquine acquired? (malaria) |
Thought to be due to increased efflux of the drug -Very common among strains of P.falciparum and uncommon but increasing for P.vivax
|
|
|
What are the pharmacokinetics of chloroquine? (malaria) |
-Rapidly and almost completely absorbed from GIT -Very large apparent volume of distribution of 100-1000L/kg -Necessitates the use of a loading dose to rapidly achieve effective serum concentrations -Slowly released from tissues and metabolized -Principally excreted in the urine |
|
|
What is the anti-malarial action of chloroquine? |
-Highly effective blood schizonticide -Moderately effective against gametocytes of P.vivax, P.ovale, and P.malariae but NOT against P.falciparum gametocytes -Not active against liver storage parasites* -Also has immunosuppressive action |
|
|
What are the clinical uses of chloroquine? (malaria) |
-Treatment of sensitive falciparum and non-falciparum -Combined with PRIMAQUINE of radical cure of P.vivax and P.ovale because chloroquine does not eliminate dormant liver forms of these species |
|
|
When is chloroquine used for chemoprophylaxis? |
-For areas WITHOUT resistant falciparum malaria in malarious regions -Amebic liver abscess * -NB: Not effective for treating intestinal or other extra-hepatic amebiasis |
|
|
What are the adverse effects of chloroquine? (malaria) |
-Usually very well tolerated -Pruritis is common -Nausea, vomiting, abdominal pain, headache, anorexia, malaise, blurred vision, and utricaria are uncommon -Dosing after meals may reduce some adverse effects -Rare reactions include hemolysis in G6PD-deficient persons, impaired hearing, confusion, psychosis, seizures, hypotension, ECG changes -Teratogenesis? Pregnancy risk category C |
|
|
What is an alkaloid derived from the bark of the cinchona tree, a traditional remedy for intermittent fevers from South American and used against malaria? |
QUININE and QUINIDINE -Remains the 1st line therapies for P.falciparum infection, esp. severe disease -Quinine is the levorotatory stereoisomer of quinidine
|
|
|
Which anti-malarial drug complexes with dsDNA to prevent strand separation, hence blocking DNA replication and transcription to RNA? |
QUININE -Rapidly absorbed orally and is metabolized before renal excretion -IV administration possible in severe infections -Solely a blood schizonticide -Used against P.falciparum infections that are resistant to chloroquine in patients who can tolerate oral treatment -Used with doxycycline or clindamycin to shorten the duration of therapy and limit toxicity |
|
|
What is the anti-malarial drug that is the dextrorotatory stereoisomer of quinine? |
QUINIDINE -IV use in the US for treatment of severe falciparum malaria -Drugs should not be used routinely for prophylaxis to delay emergence of resistance
|
|
|
Which anti-malarial drug causes Cinchonism and what does it consist of? |
Toxicity by QUINIDINE/QUININE -GI distress, headache, vertigo, blurred vision, and tinnitus |
|
|
What are the toxic reactions caused by the anti-malarials Quinine/Quinidine? |
-Severe overdose --> disturbances in cardiac conduction that resemble quinidine toxicity -Hematotoxic effects: Hemolysis in G6PD-deficient patients -Blackwater fever (IV hemolysis) --> rare and sometimes fatal complication in quinine-sensitized persons -Quinine is contraindicated with pregnancy |
|
|
Which drug is used for chloroquine-resistant falciparum malaria, esp. for cerebral malaria? |
QUININE -Oral treatment of falciparum malaria -Malarial chemoprophylaxis -Both Quinine and Quinidine are administered PARENTERALLY for treatment of severe falciparum malaria -Quinine is also used for Babesiosis infection |
|
|
What are the cautions and adverse effects associated with Quinine (anti-malarial)? |
-Cinchonism -Cardiovascular effects: severe hypotension and arrhythmia can follow TOO RAPID IV infusion -Idiosyncrasy: hemolysis with G6PD deficiency -Others: hypoglycaemia through stimulation of insulin release; stimulate uterine contractions |
|
|
Which anti-malarial 4-quinoline derivative is used as the 1st line drug for prophylaxis in all areas with chloroquine resistance and alternative drug to quinine in acute attacks resulting from P.falciparum? |
MEFLOQUINE -Only given orally due to local irritation, and absorption is variable -Mechanism of action is unknown -Resistance has emerged in regions of southeast asia |
|
|
What are common adverse effects of Mefloquine? (malaria) |
-Psychiatric disorders -Neurologic symptoms -Seizures -GI distress, skin rash, headache, dizziness -At high doses can cause cardiac conduction disturbances |
|
|
Which anti-malarial forms quinoline-quinone metabolites, which are electron-transferring redox compounds that act as cellular oxidants? |
PRIMAQUINE -Tissue (liver)schizonticide, also limites transmission by acting as a gametocide |
|
|
Which drug eradicates the liver stages of P.vivax and P.ovale and should be used in conduction with a blood schozonticide? |
PRIMAQUINE -Not active alone in acute attacks of P.vivax and P.ovale malaria |
|
|
Clinical use and adverse effects of Primaquine? |
-14 day course of primaquine is standard after treatment with chloroquine (RADICAL cure) S/E: -Usually well tolerated but may cause GI distress, pruritis, headaches and methemoglobinemia -Serious toxicity involves hemolysis in G6PD-deficient patients -Contraindicated in pregnancy |
|
|
What is Atovaquone?
|
-Anti-malarial drug, also used against. J.Jiroveci (PCP), and Babesia -M/A unknown but probably inhibits mitochondrial electron transport --> inhibiting metabolic enzymes (and may also inhibit folate metabolism?) -Used orally (poorly absorbed) and should be given with food to maximize bioavailability -Eliminated mostly via feces unchanged |
|
|
How is resistance to Atovaquone in malaria acquired? |
Mutations in cytochrome B associated (in vivo and in vitro) |
|
|
What are the common adverse effects of Atovaquone (anti-malarial)? |
-Rash, cough, NVD, fever, and abnormal liver function tests -Should be avoided in patients with a history of cardiac conduction defects, psychiatric disorders, or seizures |
|
|
Which 2 anti-malarial drugs rely on the fact that malaria synthesizes folate and the host does not? |
SULFONAMIDES and SULFONES -Sulfonamides: inhibit dyhydropteroate synthetase
|
|
|
Which 2 anti-malarial drug bind dihydrofolate reductase, inhibit formation of tetrahydrofolate, and inhibit production of purines and synthesis of nucleic acids? |
PROGUANIL and PYRIMETHANINE* -Only inhibit plasmodia in exoerythrocytic stage -Always used in combo with other agents Combinations: -Sulfadoxide/pyrimethamine (Fansidar) -Atovaquone/proguanil (Malarone) |
|
|
Which anti-malarial drugs are used for chemoprophylaxis for travellers to geographical areas with both chloroquine- and mefloquine-resistant P.falciparum? |
TETRACYCLINE AND DOXYCYCLINE
|
|
|
Which anti-malarial drug is active against the erythrocytic stage of all 4 human malaria species, including chloroqune-resistant falciparum? |
HALOFRANTINE -M/A is unknown -Active against erythrocytic stages of all 4 human malaria species, including chloroquine-resistant falciparum -Not used for chemoprophylaxis due to its potential for cardiotoxicity (QT prolongation) and embryoxicity |
|
|
What are the Artemisinin anti-malarials? |
ARTESUNATE AND ARTEMETHER -Metabolized in the food vacuole of the parasite to free radicals -Alkylate heme via free radical formation -Very effective blood schizonticides active against P.falciparum, including MDR strains -Not used for chemoprophylaxis because of their short half lives? |
|
|
Which Artemisinin combination drug is highly effective in Southeast asia where resistance to many antimalarials is common? |
ARTESUNATE-MEFLOQUINE -1st line therapy in some countries in SE Asia and South America -Relatively high cost and poor tolerability
|
|
|
Which Artemisinin combination drug is now the standard treatment for uncomplicated falciparum malaria in most countries in African and additional endemic countries elsewhere? |
ARTESUNATE-AMODIAQUINE OR ARTMETHER-LUMEFANTRINE
|
|
|
Which new Artemisinin combination drug is the new regimen with excellent efficacy? |
DIHYDROARTEMISININ-PIPERAQUINE -1st line therapy for falciparum malarian in Vietnam |
|
|
Drugs for chemoprophylaxis of malaria |
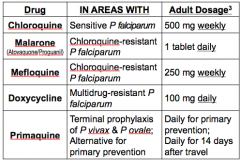
|