Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
Quadriceps Contusion
|
“Charley Horse”
Location: Anterior Thigh MOI: Direct blow (to relaxed thigh)Continual blows to the thigh compressing the quad muscle against the femur. The worse the blow and the deeper into the muscle the injury occurs will depend on the structural and functional disruption. There are 3 grades of contusion: mild, moderate and severe. Pain, swelling and ROM or decreased ROM will depend on the grade of injury. Signs/Symptoms: Pain, edema, ecchymosis, pain, tenderness, temporary loss of function, immediate bleeding in the muscle, limping in grades 2 & 3 is possible. Grade 1: “Superifical Intramustular” - mild point tenderness, mild loss of range of motion. Grade 2: “Moderate” – Range of knee flexion diminished to less than 90 degrees. Grade 3: “Deep Intramuscular – Severe” – Major limitation to range of motion. May split the fascia surrounding the quadriceps causing a muscle herniation. Tx: Conservative approach: Price, gentle static stretching, Compression with elastic bandage with knee flexed to 120 degree range of motion for first 12 hours. Crutch walking if limp is present. Isometric quadriceps contractions as soon as they can be tolerated. Prevention afterwards of great importance, use protective pads held in place by elastics.Compression with ice. Wrapping bandage around thigh and then bringing knee to 120 degrees and wrapping. This prevents loss of ROM and helps to stretch the injured quad muscles. Conservative approach to rehab, and crutch walking if limp prevents walking properly. Quad contractions may begin when the athlete can handle them. No heat or massage is advised. |
|
|
Myositis Ossificans:
|
MOI: Severe or repeated blows to the thigh/quad muscle. Can cause ectopic bone formation within the muscle -- A.K.A. Myositis Ossificans Traumatica.
S/S: positive acute edema and ecchymosis following the hemorrhage, formations that resemble bone or cartilage (can be seen over x-ray about a month after injury). Tx: rehab should be very conservative, if ossification is very painful and restricts ROM it can be removed after approximately 1 year. (is possible for it to return if it is removed too early). Athlete should not attempt to run off the injury or massage the area directly. Heat is not advised. If repeated myositis ossificans is a problem, there could be an issue with the athletes blood clotting properly. |
|
|
Muscle Strain
|
Locations: Quads and *Hamstring (most commonly strained in entire body)*
MOI: over-stretching or too forceful contraction 2 grades of tearing; Hamstrings and quadriceps contract together Change from hip extender to knee flexor Fatigue Posture Leg length discrepancy Lack of flexibility Strength imbalances S/S: Pain in muscle belly or point of attachment Capillary hemorrhage Severe hemorrhage Disability Edema Loss of function Ecchymosis Palpable mass or gap Tx: RICE, Analgesics pain killers Modalities When soreness is eliminated, focus on eccentrics strengthening Recovery may require months to a full year Scaring increases risk of injury recurrence |
|
|
Femoral Fx:
|
MOI: Direct Blow (thigh bone)
S/S: pain, deformity, ecomossis, decrease ROM, edema, point tenderness, possibility of shock, shortening of muscle possibility of open wound, bleeding (Femoral artery) shorten of the hip Tx: Splint and send, pain killers or Analgesics, ice or PRICE |
|
|
Femoral stress Fx:
|
Location: Stress Fx of the femoral neck are fairly uncommon and femoral shaft stress Fx rarely occur
MOI: Over use, usually in endurance athletes, more common in females S/S: Occur several weeks after, pain in groin or anterior thigh, pain increases with activity, pain can become constant, present with a limp Tx: rest with no running, non-weight bearing activities, possible surgery if it turns into a fracture which can be up to 12 months of recovery |
|
|
Pelvic stress Fx:
|
MOI: Repetitive abnormal overuse forces occurring in Intensive training or competitive racing
S/S: Pain in the groin with a achy sensation in the thigh, pain increases with activity Tx: Referral to physicians for X-rays, If confirmed 2-5 months rest |
|
|
Femoral Stress Fracture:
|
Location: Femur (Thigh Bone)
MOI: Overuse (rarely occurs, more prevalent in women than in men), occurs after increasing intensity of activity. S/S: Pain in groin or anterior thigh, pain increases with activity and decrease when at rest, after a while it becomes constant. Athlete walks with a limp. Care: Rest, no running. Maintain cardio through non-weight bearing exercise. If not managed properly it can result in an acute fracture, send to physician and x-ray.(12 months rehab) |
|
|
Stress Fracture of the Pelvis
|
MOI: Overuse, repetitive abnormal factors, happens in intensive training, and competitive racing.
S/S: Groin pain, aching dull pain in the thigh, increases activity and decreases with inactivity, pelvic pain following intense exercise. Care: Refer to physician, X-ray, maintain cardio through non-weight exercise, if managed improperly acute fracture can occur. Surgery is then needed. (2-5 months rehab) |
|
|
Hip Pointer:
|
Structures: Iliac Crest
MOI: Direct Blow to iliac crest S/S: Immediate Pain, spasms, inability to rotate trunk, cannot flex thigh without pain T: RICE (48hrs), bed rest, x-ray, ice massage, ultrasound, steroid, anti-inflamatory |
|
|
Osteitits pubis
|
from repeated stress on the pubis symphisis. Chronic inflammation of the pubic symphisis. Normally seen in long distance runners and soccer players. Pain is present in the groin, including point tenderness during running, squats, and sit-ups. rx- anti-inflammatories (including injectables), rest, and gradual return to play.
|
|
|
Legg-Calve Perthes Disease
|
Avascular necrosis of the femoral head
Disruption of circulation at the femoral head MOI: not sure what causes it but the theory that blood supply does not reach that part of the femur but that is just a theory S/S: pain in the groin, also can be referred to the knee or abdomen, limping, decreased ROM TX: may need a brace to avoid direct on weight on the hip joint, needs rest and non-weight bearing Develops slowly Most common in children, boys age 4-10 More prone to dislocations because the femoral head becomes misshapen when the bone dies and does not fit in the hip joint like it should |
|
|
SLIPPED CAPITAL FEMORAL EPIPHYSIS
|
A slipped capital femoral epiphysis is a separation ball of the hip joint from the thigh bone (femur) at the upper growing end (growth plate) of the bone. SCFE happens in about two out of every 100,000 children. It is more common in growing children between the ages 10 to 17, especially boys who are tall and thin or very fat. Children with hormonal misbalance in ¼ of the cases happen in both hips. The cause of SCFE is unknown. In many cases is overweight
The symptoms are difficulty walking, walking with a limb, knee pain, hip pain, and hip stiffness outward, and turning leg, decrease range of motion and restricted hip movements. The treatment for SCFE is as follows: • In case minor displacement, rest and no weigh bearing may prevent further injury. • In major cases the treatment is mostly immediate, most likely; surgery is usually performed with in 24 to 48 hours. Surgery stabilizes the bone with pins and screws which prevent further, slippage or displacement at the ball of the hip joint. |
|
|
Pelvic Fracture:
|
Close circuit- bilateral fx = fracture on one side results in fracture on both sides.
MOI: Direct blow results in bones being displaced. S/S: obvious deformity, pain, no ROM, ecchymosis, edema, shock T/X: Splint & send to the hospital for x-rays. |
|
|
Dislocated Hip:
|
Bone: acetabulum
Hip fractures are common with dislocated hip. Falling on bent knee of falling on the side, severe twisting motion. S/S: Flexed abducted, internally rotated. Pain, muscle guarding,positive deformity, ecchymosis. edema, decrease ROM, complications include damage to sciatic nerve, nutrient loss to artery = avascular necrosis Tx: medical emergency. O.R.I.F. = open reduction internal fixation. immobilize 2 wks. crutches for one month or longer. |
|
|
Piriformis Syndrome:
|
Muscle in butt.
nerve gets compressed or irritated by tightness or muscle spasm of piriformis. MOI: Muscle spasm S/S: pain, numbness, tingling in butt, & can extend to the knee & foot. May worsen due to sitting long periods of time, stairs, walking or running, Tx: stretching, massage, NSAID's, stop activity of running, bicycling, climbing, corticoid steroid injection, possible surgery. |
|
|
Herniated Lumbar Disc:
|
4 degrees/ levels
MOI: lifting & twisting in the a.m. & there is increased risk with age. Sx: Depends on the level of damage. Only on one side may not have signs or symptoms. pain, spasms, decreased rom, decreased strength. Tx: degree I & II, rehab, conservative degree III = conservative or surgery, rest, core strength, traction degree IIII = surgery |
|
|
Spondylolysis:
|
stress fx of vertebrae on one side of PARS articularis,
MOI: compression, shearing forces, torsion, -> broad options for MOI. Sx: achy constant pain in low back, no specific MOI. Tx: MRI or bone scan, proper mechanics, stretching, strengthen. |
|
|
Spondylolisthesis
|
fx on both sides of PARS articularis, 5 degrees. grade 5 is when there is an over gap.
MOI: slip over time. Sx: depends on the level of severity. can damage nerves, constant local pain, point tender. Tx: grade I & II = conservative grade III = conservative or surgery grades 4 & 5 = aggressive, surgery, fuse vertebrae together or fuse slipped (as is) |
|
|
Sacroiliac sprain:
|
MOI: improper mechanics.
Sx: pelvis is rotated Tx: muscle energy used to put perlvis back in correct position, strengthen, fix bio-mechanics problems. |
|
|
Coccyx Injuries:
|
MOI: direct blow, common in gymnasts.
Sx: deep pain, in middle of butt & not possible to palpate. Tx: send for x-rays, doughnut circle to comfort, improve ROM, core strength, stretch muscles. |
|
|
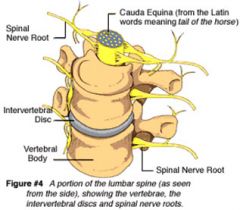
Spine
|
7 Cervical vertebrae: top region, C1= atlas, C2=axis, 8 cervical nerves
12 Thoracic vertebrae, 12 thoracic nerves 5 lumbar vertebrae: 5 lumbar nerves. Sacrum: 5 fused vertebrae Coccyx: 3-4 fused vertebrae. |
|
|
Spine anatomy:
|
Intervertebral Discs: in between vertebrae, outside firm, inside not firm, protects nerves
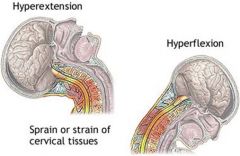
Ligaments: anterior longitudinal - to prevent hyper extension. posterior longitudinal - to prevent hyper flexion. Muscles: Abs flex lumbar spine. Erector spinae will extend spine. Rotation & lateral movement. |
|
|
Spinal Nerves
|
|
|
|
Cervical Fracture:
|
MOI:axial load is most common & it is a direct blow from the top of head.
Sx: burning, tingling, numbness bilaterally, muscle spasms, point tenderness. Tx: head between knees & palpate w/ fingers & hands. palpate down & back up. start @ C2 & look for point tenderness @ the same vertebrae. Wait for EMS, helmet, mask & shoulder pads all have to come off together. Fx of C2 is a hangman fracture & is put in halo collar. Controversial tx: injection of cold fluid to lower core temp. |
|
|
Cervical Dislocation
|
MOI: axial load plus a rotation of neck
Sx: rotation position, ecchymosis, edema, point tenderness, burning, tingling, numbness. Tx: Surgical, anterior surgery is the most successful. DQ'd from official sport. |
|
|
Cervical Sprain:
|
MOI: whiplash. common with soccer, football & rugby. anterior & posterior ligament hyper extension & hyper flexion.
Sx: dull achy pain, decrease ROM, pain, muscle spasms. Tx: cervical collar, limit ROM, decrease muscle spasms w/ ice, heat after 72 hours, gentle stretching, strengthen, |
|
|
Cervical Sprain
|
|
|
|
Acute Torticollis: Rye or Stiff Neck
|
MOI: holding head in an unusual position for an extended period of time. Most common in athletes after the weekend due to athletes passing out.
Sx: decreased ROM, pain, stiffness, muscle spasms. Tx: stripping muscle (type of massage), stretching, heat, ice, e-stimulation. |
|
|
Brachial Plexus Neurapraxia:
stinger, burner, dead arm. |
MOI: brachial plexus (group of nerves on both sides of neck) stretched due to traction or compression.
Sx: burning, tingling & numbness on injured side. Tx: never diagnose bilateral because it could be a fx. send for x-rays. wait & see, feeling should return within few minutes. Full strength & full ROM required to return to play. |
|
|
Low Back Pain: L.B.P.
|
80%:of population effected
Pre-Disposing Factors:poor posture, tight hamstrings, weak core, poor biomechanics. MOI: Improper lifting mechanics, not using core, direct blow, axial load. Sx: muscle spasms, achy pain, decrease ROM, burning, tingling, numbness. Tx: stretch hamstrings, strengthen core, transverse abdominus & multivitus. work on uneven surface ex. bosu ball. chiropractor. |
|
|
Lumbar Fracture:
|
MOI: not common. compression fx due to axial load force.
Sx: point tenderness, decrease ROM, muscle spasm, burning, tingling, numbness in both legs. Tx: immobilize w/ vacuum splint or back board & protect on both sides of the body. Surgery by fusing bones together, bone graft or plating with titanium, rehab after surgery. |
|
|
Lumbar Sprain/Strain
|
MOI: Improper lifting
Sx: spasms, dull achy pain, decrease ROM, decrease strength, Tx: rest, ice, NSAID's, core strength, belt, reinforce proper lifting, proper mechanics. |
|
|
Contusions:
|
MOI: direct blow. low back & therefore there is a concern for damage to kidneys
Sx: ecchymosis, edema, tender, blood in urine. Tx: pad. |
|
|
Sciatica:
|
compression of sciatica nerve
Pre-Disposing Factors: females w/ wide hips, runners & cyclists. MOI: compression Sx: burning, tingling, numbness on back of the legs. Tx: stretch, figure 4 stretch, & ball massage |
|
|
This injury results in bone being laid down in the muscle belly:
|
Myositis Ossificans
|
|
|
This injury results in femoral head shaping incorrectly due to a poor blood supply:
|
Legg Calve Perthes Disease
|
|
|
The most commonly strained muscle in the body is:
|
Hamstrings
|
|
|
What is the #1 sign/symptom of a concussion:
|
Headache
|
|
|
Where will a lacerated spleen refer pain?
|
Left shoulder
|
|
|
Which of the following head injuries is due to an arterial bleed within the brain?
|
epidural hematoma
|
|
|
This injury results in the pleural cavity filling with blood:
|
Hemothorax
|
|
|
The leading cause of sudden athlete death in the U.S. is:
|
Hypertrophic Cardiomyopathy
|
|
|
McBurney's point is referred pain site from what structure?
|
Appendix
|
|
|
This injury results in the diaphragm becoming paralyzed:
|
Solar Plexus Blow
|
|
|
Which of the following injuries will occur due to holding one's head in an unusual position for an extended period of time?
|
Acute Torticollis
|
|
|
What is hematuria?
|
Blood in urine
|
|
|
This injury is a stress fracture on one side of the vertebrae:
|
Spondylolysis
|
|
|
Head Anatomy:
|
Brain does not regenerate
Bones: skull, temporal, poreatals, frontal, occipital -> all fused together. Brain Cerebrum Cerebellum Pons Medulla Oblongata Meninges Cerebrospinal Fluid: fluid in the spine & skull, protects, lubricates, & provides nutrients. Leaking fluid from nose, ears, etc is a medical emergency. |
|
|
Skull Fracture:
|
Depression fx is the most common
MOI: direct blow. S/S: swelling, point tenderness, edema, crepitis, raccoon eyes, battle sign (bruising behind ears) Tx: palpate for crepitis, 911 & send to hospital to monitor pressure on brain. |
|
|
Epidural Hematoma:
|
MOI: Artery. Arterial bleed, fast & spurting. Direct blow.
S/S: develop quickly, fast spurting bleed, dizziness, nausea, headache, pupil on side of bleed dilates. Tx: Hospital. Medical emergency. install shunt to release pressure. |
|
|
Subdural Hematoma
|
MOI: Direct blow. Venous bleed. Takes a while to develop.
S/S: slow bleed. Tx: Hospital, install shunt to release pressure. Is a medical emergency. |
|
|
Scalp Injuries
|
MOI: Direct blow, torsion forces, shearing forces, laceration, incision, avulsion, rupture.
S/S: a lot of blood, tender to palpation. Tx:control bleeding, facial or scalp injuries always refer for sutures. |
|
|
Concussions:
|
MOI: direct blow to head or body. If body it's from shearing forces or whiplash in the brain stem.
Grading: NOT GRADED. A concussion is simply a concussion.MRI & CAT scan are done to rule out hematomas. S/S: headache in 94%, nausea, disorientation, dizzy, sensitive to light, emotional changes, sleep problems, cognitive disturbances. Tx: rest, no stress, NO MEDS! Return to play guidelines: 5 steps, 24 hours in between each step, called A-symptomatic for 24 hours between each step. 7 days of minimum rest. 3 concussions increase risk for alzheimers, lou gherig diseas, clinical depression & ADD. Testing: neuro-cognitive tests memory & reaction time. |
|
|
Second Impact Syndrome
|
MOI: return to play too quickly following injury & re-injure head. 2nd injury is less severe than the 1st.
S/S: coma, lose consciousness & dies. Tx: send to hospital to relieve pressure on brain. If a person lives they will have permanent brain damage. |
|
|
Post Concussion Syndrome:
|
MOI:multiple concussions
S/S: psychological & physical. sleep apnea, insomnia, decreased knowledge, personality changes, clinical depression - all 6 mos. or longer. Tx: medication, can't return to play, happens in 20-30% of athletes. |