![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
validity |
does it measure what its suppose to |
|
|
reliable |
if you test multiple times do you get the same result |
|
|
criterion based standards |
-level above this value is unhealthy -enough data to support a cut off point |
|
|
normative base standards |
-no cut off -normative data -normal might not be healthy, just tells you what normal is -pulmonary stuff is normative -not enough data to give cut of point |
|
|
factors affecting gas volume |
-temp + Heating a gas will increase thevelocity of the molecules which will increase pressure (increase temp means increase collisions of molecules and the pressure increases +cooling will slow downthe movement of the molecules -atm pressure -water vapor (% hum) -these three factors have to be accounted for earn measuring volumes under differing environmentalconditions |
|
|
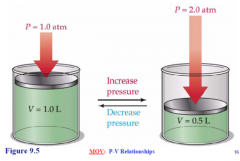
charles law |
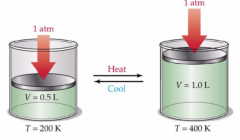
In a constant temperature system, increasing the pressure will force the molecules closer together thus decreasing volume |
|
|
Boyles Law |
|
|
|
barometer reading at sea level and at mt everest |
-sea level: 760 mm Hg -mt everest: 270mm Hg |
|
|
atm pressure affected by |
-altitude -weather (day to day changes) -heating/cool systems in a building |
|
|
I atm = |
760 mmhg or 760 torr |
|
|
water vapor |
-The volume of a gas carries depending on its water vapor content -the volume of gas is greater when the gas is saturated -dry gas occupies a lower volume -pulmonary volumes are always saturated in the body -the water vapor pressure in the lab depends on temp |
|
|
correction factors |
corrected to a standard condition of temp, pressure and water vapor |
|
|
ATPS |
-ambient temperature pressure saturated -This is the volume you measure in the lab |
|
|
STPD |

-Standard temp pressure dry -used for all metabolic volumes such as VO2 and VCO2 -Ts = temp of sample in C Pbr= barometric pressure (does it need to be corrected for?) -ph20 is vapor pressure -273 is Kalvin at 0 degrees C -760 is atm pressure at sea level -should be a value lower than 1 |
|
|
BTPS |

-Body temp and pressure saturated -used for all pulmonary volumes -FVC, RV, MVVs -should be a value greater than 1 |
|
|
pulmonary tests done when... |
-Symptoms: dyspnea, wheezing, orthopnea, couph, phlegm production, chest pain -signs: decreased breath sounds, over infiltration, expiratory slowing, cyanosis, chest deformation, unexpected crackles -abnormal lab tests: hypoxemia, hypercapnea, polycythemia (to many RBC, abnormal chest radiographs - Toscreen individuals at risk of having pulmonary diseases (.Smokers and Individualsin occupations with exposures to injurious substances) - Toassess preoperative risk - Toassess prognosis (lung transplant, etc.) -Toassess health status before enrollment in strenuous physical activity programs -To asses heraputic interventions + brochodilator therapy +steroid treatment for asthma, interstitial lung disease |
|
|
Contradictions for pulmonary tests |
-Hemoptysisof unknown origin - Pneumothorax - Unstableangina pectoris -Recentmyocardial infarction -Thoracicaneurysms -Abdominalaneurysms -Cerebralaneurysms -Recenteye surgery (increased intraocular pressure during forced expiration) -Recentabdominal or thoracic surgical procedures - Historyof syncope associated with forced exhalation -dont want to increase pressure from test that would cause issues if people had these issues above |
|
|
pulmonary function tests |
-Spirometry: assessing lung volumes by actively moving the volume of lungs; measured while inhaling/exhaling -Lung volumes: measuring lung volumes inactively -gas transfer (diffusion capacity): inhale gas and see how quickly it shows up in blood; assess alveoli function -blood gases |
|
|
lung volumes |
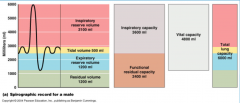
-Vital capacity: -Total Lung Capacity: -Inspiratory capacityL -tidal volume -Inspriartory reserve volume -Expiratory reserve volume -resodual volume -Functional residual capacity: - - |
|
|
total lung capacity |
the volume in the lungs at maximal inflation, the sum of VC and RV |
|
|
vital capacity |
-the volume of air breathed out after the deepest inhalation -a complete exhalation following a complete inhalation -rate is slow |
|
|
Inspiratory capacity |
the sum of IRV and TV |
|
|
tidal volume |
amount of air that you breath in and out normally |
|
|
inspiratory reserve volume |
the maximal volume that can be inhaled from the end-inspiratory level |
|
|
experatory reserve volume |
the maximal volume of air that can be exhaled from the end-expiratory position |
|
|
residual volume |
the volume of air remaining in the lungs after a maximal exhalation |
|
|
functional residual capacity |
-amount of air left in lungs after a normal expiration - the volume in the lungs at the end-expiratory position -important because this is the natural state that the lungs want to be in -diaphragm contracts for inspiration and relaxes for expiration; father past that point the more muscles activity is needed |
|
|
VC procedure |
-subject stands -a nose clip is placed on nose -subject breaths in completely and exhales completely with a tight seal around mouth peice |
|
|
VC criteria for acceptability |
-at least 2 acceptable VC maneuvers should be preformed with 200 ml or less difference -VC should be within 200 ml of FVC -if computerizes there should be a clear plateau observed for both inspiration and expiration and the end expiatory volume should carry less than 100 ml for three preceding breaths |
|
|
VC interpreting results |
-VC in healthy adults is determined by age height and gender -normative data -VC evaluation is based on % of predicted -health individuals can carrie up to 20% |
|
|
reasons of low VC |
-was it a true effort? was it reproducible? -loss of distendable lung volume: tumor or surgical removal of lung tissue -restrictive (causes big change in VC) and some obstructive diseases -neural disorders: can't inhale/exhale maximally -a reduction in VC is considered a nonspecific finding and further testing should be done |
|
|
restrictive diseases |
-total amount of air moving is lower than normal but rate is normal -ex: scar tissue, tumor, -causes big change in VC -FEV1/FVC will be normal (above 80%) |
|
|
obstructive diseases |
-total amount of air being moved is normal but rate is lower than normal -ex: COPD, asthma -causes small change in VC -FEV1/FVC will be abnormal |
|
|
FVC |
-forced vital capacity -inhalation is rapid and exhalation is maximal -allows measurement of rates as well as volume (important in distinguishing between diseases) -stronger diagnostic test -the total amount of air expired as quickly as possible after taking the deepest breath possible -measured in L |
|
|
FVC procedure |
-subject stands -nose clip -breath into mouth piece attached to spirometer -subject breaths normally for 3-4 breaths -inhales completely and w/o pausing the subject exhales as forcible and quickly as they can |
|
|
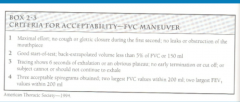
FVC test acceptability criteria |
|
|
|
interpreting FVC results |
-FVC should be w/in 200ml of VC -if FVC is less than VC either the person was not giving max effort or they have an obstructive disease (pressure causes small airways to com apes during max effort) (emphysema or asthma) or a restrictive disease -restrictive diseases cause bigger change than obstructive diseases |
|
|
FEV1 |
-volume of air which can be forcibly exhaled from lungs in the first second of a forced expiratory maneuver -rate is taken into consideration -both restrictive and obstructive diseases are going to lower the FEV1 but how they do it is different |
|
|
FEV1/FVC |
-indicates what percentage of the total FVC was expelled from the lungs during the first second of forced exhalation -normal = above 80% -restrictive will have normal value while obstructive will have abnormal value |
|
|
FEF 25%-75% |
-The amount of air expelled from the lungs during the middle half of the FVC test -represents airway flow in the small to medium airways -large variability in normal people limits its usefulness transition from middle to small airways |
|
|
PEF |
primarily a measure of large airway function -extremely effort dependent -consistently low= obstructive disease in large airways (asthma) |
|
|
asthma |
-peak experatory flow reduced so maximum height of loop is reduced -concaves shape of downward slope -more concaved means more severe - Airflow reduces rapidly with thereduction in the lung volumes because the airways narrow and the loop becomeconcave -Concavity may be the indicator ofairflow obstruction and may present before the change in FEV1 or FEV1/FVC |
|
|
emphysema |
-Airways may collapse during forced expirationbecause of destruction of the supporting lung tissue causing very reduced flowat low lung volume and a characteristic (dog-leg) appearance to the flow volumecurve |
|
|
2 compartment model |
- Assumesbody is made up of fat, and everything else (fat free mass) - Everythingelse (muscle, bone, organs, body water etc… exists in a constant ratio) -Thismodel has been around since early 60s -Usedextensively for body composition -Hydrostaticweighing is based on this model -fat mass = 0.900 g/cc -FFM= 1.100 g/cc -density of water is 1 so fat floats and everything else doesn't |
|
|
problems with 2 compartment model |
-how hydrated the person is -decreased bone density -ratio of bone to muscle -blacks have been found to have a higher FFM density of 1.113 g/cc than whites -exercise training/athletes have more muscle which means more h2o, connective tissue, and increased bone density -based on a few cadaver studies, but not many healthy people are dead to get info on -aging decreases muscle, bone density connective tissue and water |
|
|
3 compartment model |
-fat free mass, fat mass and total body water -total body water is measured by isotope dilution -expensive and is rarely used - TBW is used in conjunction withbody density from hydrostatic weighing or plethysmography fora more precise estimation of body composition -%fat=[(2.11/Db)-0.78W-1.354]X100 -W = total body water as a fractionof body weight -more accurate than 2 comp model |
|
|
isotope dilution |
-TBWis the ratio of a dose of a tracer given to it’s concentration found in the bodyafter an equilibrium period -Samplesare analyzed using mass spectroscopy or gas chromatography -thistechnique likely over estimates TBW by 0.5-2%- correction factors are usuallyused. -Howeverthis technique is very reproducible -Recentresearch has suggested that under controlled conditions, TBW can be estimatedusing multifrequency BIA |
|
|
BIA |
-passes electrical current through you and sees how fast electrons move because water conducts electrons faster -is pretty accurate, much cheeper and faster than isotope dilution |
|
|
4 compartment model |
-fat, water, bone, protein/other -Use DEXA (dual energy x ray absorptometry) to get bone mineral content -use isotopic enrichment to measure total body water (TBW) -use hydrostatic weighing or bod pod to get Db (fat/muscle) - These values are then plugged intoan equation to get body fat % -%BF=[2.559/Db-0.734W+0.983TBBM-1.841]X100 -W is TBW/body mass -TBBM is TBM (kg)/body mass -water density contributes to the biggest variation from 2c to 4c |
|
|
essential body fat |
-found around organs for insulation and protection, brain, cell component -is not there for energy -its a protective tissue -if yu are obese your essential fat increases -female body fat is essential energy surplus for feeing child and is hormonally metabolized for the child and not for the mother -men have 3% essential while women have 12% -too little essential fat and mentration ceases |
|
|
storage fat |
-purpose: where we store extra calories -location: subcutaneous and verseral fat -mostly subcutaneous (how skin fold work) -location is determined by hormones -women store fat around legs and hips while men store fat centrally -hip/waist ratio is best test to determine subcutaneous vs visceral fat -is the same for male and female |
|
|
archimedes 1st principle |
if you submerge an object in water the volume of that object is equal to the volume of water displaced |
|
|
archimedes 2nd principle |
weight that is lost under water is equal to the weight of the volume of water that is displaced |
|
|
ways to get underwater weight |
-cadaver scale: hanging scale in water -force plate |
|
|
what else makes a person more buoyant?
|
-air in lungs +need to get to RV -air in GI tract +overmnight fast +no soda or legumes -swimsuits/hair trapping air +should pat down |
|
|
equations of body comp |
-used to convert Db to % body fat -Siri -Brozek -RV: can estimate w/ formula(age, gender, height) or can predict using VC -GI gas: no way to predicting so used standard for equation |
|
|
disadvantages of hydrostatic weighing |
-costly to build/ maintain -lab only -lengthy test -subject dependent -limited number of pop specific equations |
|
|
hydrostatic weighing prosedure |
-no food for at least 2 hrs -no exercise before -no diuretics -go to bathroom -get weight on land in clothes they will be wearing in water -calabrate -subject gets in tank -rbs body -get on scale -add weights -chin just above water -nose plug -couple of full breaths -max exhale under h2o -no bubbles for 7 sec and then subject and come up -repete 10x -use either highest weight, average of last 3 trials -use either highest weight if found more than once, 2nd highest weight if found more than once, or third highest weight i |
|
|
helium dilution |
x |
|
|
skin folds |
-measuresdouble thickness of skin and subcutaneous fat |
|
|
skin fold advantages |
-inexpensive -fast -portable -largedatabase |
|
|
skin fold assumptions |
-predicts non-subcutaneous fat -sites selected represent averagethickness of all subcutaneous fat -compressibility of fat similarbetween subjects -thickness of skin negligible |
|
|
skin fold limitations |
-Skinfoldthickness affected by factors other than amount of fat +exerciseincreases skin thickness +dehydrationreduces skin thickness +edemaincreases skin thickness +dermatitisincreases skin thickness -Poorlypredicts visceral fat -Useshydrostatic weighing as criterion measure |
|
|
skin fold sources of error |
-Poor inter tester reliability -Siteselection is biggest problem +Differencein “pinch” +Alwaysuse same tester for serial measures +Researchsuggest a minimum of 50-100 tests before a person is competent - Calipers (not a big change) -Equations used -Size of skin fold +easy to do on lean males +hard to do for overweight individuals because tester doesn't know what to pinch |