![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back
|
What do palpitations not related to emotion, fever or exercise suggest? |
An arrhythmia |
|
|
Name the 5 most likely diagnosis for palpitations |
Anxiety Premature beats (ectopics) - most common Sinus tachycardia Drugs (e.g. stimulants) Supraventricular tachycardia |
|
|
Name at least 6 possible diagnoses for palpitations that should not be missed |
Myocardial infarction/angina Arrhythmias: • atrial fibrillation/flutter • ventricular tachycardia • bradycardia • sick sinus syndrome • torsade de pointes Long QT syndrome Wolff–Parkinson–White (WPW) syndrome Electrolyte disturbances: • hypokalaemia • hypomagnesaemia • hypoglycaemia (type 1 diabetes) |
|
|
What is the commonest cause of an apparent pause on the ECG? |
A blocked premature atrial beat/complex (atrial ectopic) |
|
|
What are common triggers of paroxysmal supraventricular tachycardia (PSVT)? |
Anxiety and cigarette smoking |
|
|
How can you differentiate between sinus tachycardia and PSVT? |
Sinus tachycardia - Rate 100-150 - Starts and stops more gradually - Precipitated by emotion, stress, fever or exercise PSVT - Rate 160-220 - Abrupt cessation |
|
|
Name at least 5 drugs that can cause palpitations |
Alcohol Alendronate Amphetamines Antipsychotics e.g CPZ, haloperidol, olanzapine Antiarrhythmic drugs Antidepressants:• tricyclics• MAO inhibitors Atropine, hyoscine, hyoscyomine Caffeine Cocaine Digitalis Diuretics → K ↓, Mg ↓Glyceryl trinitrate Sympathomimetics:• in decongestants (e.g. pseudoephedrine, ephedrine)• β-agonists (e.g. salbutamol, terbutaline) Thyroxine |
|
|
In combination with palpitations what would the following features on history potentially indicate: Chest pain? Breathlessness? Dizziness or syncope? |
Chest pain - myocardial ischaemia or aortic stenosis Breathlessness - anxiety with hyperventilation, mitral stenosis or cardiac failure Dizziness or syncope - severe arrhythmias such as SSS and complete heart block, aortic stenosis and associated cerebrovascular disease |
|

|

|
|
|
What are possible causes of an irregular pulse? |
Ectopic beats Atrial fibrillation Atrial flutter with varying degrees of block |
|
|
Name at least 5 signs to look for on examination to help rule in a diagnosis with palpitations |
Hyperthyroid signs - exophthalmos - sweaty palms - goitre CCF - peripheral oedema - raised JVP - murmur - cardiomegaly - basal crackles in lungs Pallor of anaemia Peripheral vascular disease HTN |
|
|
What blood tests might you conduct for a patient with palpitations? Any imaging? |
FBC Thyroid function tests Serum electrolytes and magnesium Serum digoxin ? digitalis toxicity Virus antibodies ? myocarditis CXR |
|
|
What specific cardiac investigations might you consider for a patient with palpitations? |
ECG (12 lead)ambulatory 24-hour ECG monitoring echocardiography (to look for valvular heart disease and assess left ventricular function) electrophysiology studies exercise stress test (? underlying CAD) event monitor (can record up to 2 weeks) implantable monitor (may last 1 year) |
|
|
What is the gold standard investigation for arrhythmias? |
Electrophysiological studies are the gold standard investigation for tachycardias but are rarely needed for diagnosing most arrhythmias |
|

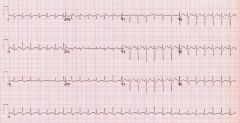
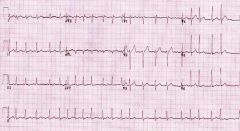
Name the rhythm |
Sinus rhythm |
|

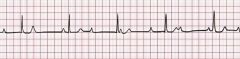
Rhythm? Causes? Rx? |
Sinus bradycardia Causes: Normal during sleep, Increased vagal tone (e.g. athletes), Vagal stimulation (e.g. pain), Inferior myocardial infarction, Sinus node disease, Hypothyroidism, Hypothermia, Anorexia nervosa, Electrolyte abnormalities – hyperkalaemia, hypermagnesaemia, Brainstem herniation (the Cushing reflex), Myocarditis Drugs e.g. beta-blockers, CCBs, digoxin, opiates, amiodarone Remove cause/ treat underlying pathology |
|
Rhythm? Rx? |
Sinus tachycardia Causes: Exercise, Pain, anxiety, Hypoxia, hypercarbia, Acidaemia, Sepsis, pyrexia, Pulmonary embolism, Hyperthyroidism Drugs: Beta-agonists: adrenaline, isoprenaline, salbutamol, dobutamine Sympathomimetics: amphetamines, cocaine, methylphenidate Antimuscarinics: antihistamines, TCAs, carbamazepine, atropine Others: caffeine, theophylline, marijuana Rx: Treat underlying cause |
|
|
What should you think of if the ECG shows any of the following? Sinus Bradycardia Sinus Arrhythmia — associated with sinus node dysfunction in the elderly in the absence of respiratory pattern association Sinoatrial Exit Block Sinus Arrest — pause > 3 seconds Atrial fibrillation with slow ventricular response Bradycardia – tachycardia syndrome. |
Sick sinus syndrome |
|
|
Name at least 5 symptoms a patient with sick sinus syndrome might exhibit |
Bradycardia Syncope Fatigue Weakness Shortness of breath (dyspnea) Chest pain (angina) Disturbed sleep Confusion Heart palpitations |
|
|
What are the 5 possible intrinsic causes of sick sinus syndrome? |
Idiopathic Degenerative Fibrosis (commonest) Ischaemia Cardiomyopathies Infiltrative Diseases e.g. sarcoidosis, haemochromatosis Congenital abnormalities. |
|
|
What are the 4 possible extrinsic causes of sick sinus syndrome? |
Drugs e.g. digoxin, beta-blockers, calcium channel blockers Autonomic dysfunction Hypothyroidism Electrolyte abnormalities — e.g. hyperkalaemia |
|
|
What treatment options are there for sick sinus syndrome? |
Treat underlying cause Insertion of pacemaker |
|

Dx? Causes? Rx? |
1st degree AV block - P waves buried in preceding T wave Causes: Increased vagal tone Athletic training Inferior MI Mitral valve surgery Myocarditis (e.g. Lyme disease) Electrolyte disturbances (e.g. Hyperkalaemia) AV nodal blocking drugs (beta-blockers, calcium channel blockers, digoxin, amiodarone) May be a normal variant Rx: No specific treatment required |
|

Dx? Causes? Rx? |
AV block: 2nd degree - Mobiz I (Wenckebach) Progressive prolongation of the PR interval culminating in a non-conducted P wave Causes: Drugs: beta-blockers, calcium channel blockers, digoxin, amiodarone Increased vagal tone (e.g. athletes) Inferior MI Myocarditis Following cardiac surgery (mitral valve repair, Tetralogy of Fallot repair) Rx: If asymptomatic - no rx required Symptomatic patients usually respond to atropine Permanent pacing is rarely required. |
|

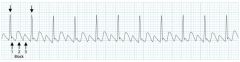
Dx? Causes? Rx? |
AV block: 2nd degree - Mobitz II Intermittent non-conducted P waves without progressive prolongation of the PR interval Causes: Anterior MI (due to septal infarction with necrosis of the bundle branches) Idiopathic fibrosis of the conducting system (Lenegre’s or Lev’s disease) Cardiac surgery (especially surgery occurring close to the septum, e.g. mitral valve repair) Inflammatory conditions (rheumatic fever, myocarditis, Lyme disease) Autoimmune (SLE, systemic sclerosis) Infiltrative myocardial disease (amyloidosis, haemochromatosis, sarcoidosis) Hyperkalaemia.Drugs: beta-blockers, calcium channel blockers, digoxin, amiodarone Rx: Mobitz II is much more likely than Mobitz I to be associated with haemodynamic compromise, severe bradycardia and progression to 3rd degree heart block Onset of haemodynamic instability may be sudden and unexpected, causing syncope (Stokes-Adams attacks) or sudden cardiac death The risk of asystole is around 35% per year. Mobitz II mandates immediate admission for cardiac monitoring, backup temporary pacing and ultimately insertion of a permanent pacemaker. |
|
|
How can you tell the difference between Mobitz I and II in a patient with either 2:1 or 3:1 fixed ratio blocks? |
Mobitz I conduction is more likely to produce narrow QRS complexes, as the block is located at the level of the AV node. This type of fixed ratio block tends to improve with atropine and has an overall more benign prognosis. Mobitz II conduction typically produces broad QRS complexes, as it usually occurs in the context of pre-existing LBBB or bifascicular block. This type of fixed ratio block tends to worsen with atropine and is more likely to progress to 3rd degree heart block or asystole. |
|
Dx: Causes: Rx: |
Complete (3rd degree) heart block There is complete absence of AV conduction- none of the supraventricular impulses are conducted to the ventricles. Causes: Same as Mobitz I and II but important ones are: Inferior myocardial infarction AV-nodal blocking drugs (e.g. calcium-channel blockers, beta-blockers, digoxin) Idiopathic degeneration of the conducting system (Lenegre’s or Lev’s disease) Rx: Patients with third degree heart block are at high risk of ventricular standstill and sudden cardiac death. They require urgent admission for cardiac monitoring, backup temporary pacing and usually insertion of a permanent pacemaker. |
|

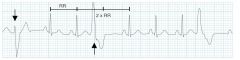
Dx? |
Premature Atrial Complex An abnormal (non-sinus) P wave is followed by a QRS complex The P wave typically has a different morphology and axis to the sinus P waves. PACs may be either: Unifocal – Arising from a single ectopic focus; each PAC is identical. Multifocal – Arising from two or more ectopic foci; multiple P-wave morphologies. |
|
|
What are the possible causes of a Premature Atrial Complex? |
Anxiety. Sympathomimetics. Beta-agonists. Excess caffeine. Hypokalaemia. Hypomagnesaemia. Digoxin toxicity. Myocardial ischaemia |
|
|
What is the clinical significant of a Premature Atrial Complex? |
PACs are a normal electrophysiological phenomenon not usually requiring investigation or treatment. Frequent PACs may cause palpitations and a sense of the heart “skipping a beat”. In patients with underlying predispositions (e.g. left atrial enlargement, ischaemic heart disease, WPW), a PAC may be the trigger for the onset of a re-entrant tachydysrhythmia — e.g. AF, flutter, AVNRT, AVRT. |
|
|
Explain the following in regards to premature atrial complexes: Bigeminy Trigeminy Quadrigeminy Couplet Triplet |
Bigeminy — every other beat is a PAC. Trigeminy — every third beat is a PAC. Quadrigeminy — every fourth beat is a PAC. Couplet – two consecutive PACs.Triplet — three consecutive PACs. |
|
|
Describe a Stokes-Adams Attack |
Sudden onset without warning Patient falls to Collapse with loss of consciousness Pallor and still as if dead with slow or absent pulse Recovery—in seconds back to normal Patient flushes as pulse increases Refer for management as attacks may be recurrent |
|
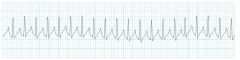
Rate is 150–220/min Dx? |
Supraventricular tachycardia - Can be paroxysmal or sustained Paroxysmal SVT (pSVT) describes an SVT with abrupt onset and offset There are at least eight different types of SVT with differing risks and responses to treatment. PSVT commonly presents with a sudden onset in otherwise healthy young people. Passing copious urine after an attack is characteristic of PSVT. Look for predisposing factors such as an accessory pathway and thyrotoxicosis. Approximately 60% are due to atrioventricular (AV) node re-entry and 35% due to accessory pathway tachycardia (e.g. WPW). Look for evidence of accessory pathways after reversion because accessory pathways can lead to sudden death (avoid digoxin in WPW). Consider SSS in a patient with SVT and dizziness. |
|
|
What treatment can be given for paroxysmal supraventricular tachycardia? |
Vagal stimulation can be attempted. Carotid sinus massage is the first treatment of choice. Other methods of vagal stimulation include: Valsalva manoeuvre (easiest for patient) self-induced vomiting ocular pressure (avoid) cold (ice) water to face or swallowing ice immersion of the face in water If vagal stimulation fails: give adenosine IV (try 6 mg first over 5–10 seconds, then 12 mg in 2 minutes if unsuccessful, then 18 mg in 2 minutes if necessary and well tolerated). Second-line treatment is verapamil IV 1 mg/min up to 10–15 mg (provided patient is not taking a beta blocker). |
|
|
What precautions should you use when administering adenosine for the treatment of paroxysmal supraventicular tachycardia? |
Adenosine causes less hypotension than verapamil but may cause bronchospasm in asthmatics Use only if narrow QRS and BP >80 mm Hg Carefully monitor blood pressure AVOID verapamil if taking β-blockers and persistent tachycardia with QRS complexes >0.14 s (suggests ventricular tachycardia) |
|
|
What can you consider if giving adenosine fails in the treatment of paroxysmal supraventicular tachycardia? |
DC cardioversion Overdrive pacing |
|
|
What can by used for the prevention of paroxysmal supraventricular tachycardia? |
To prevent recurrences (frequent episodes) use atenolol or metoprolol, flecainide (only if no structural heart damage) or sotalol. If these agents fail, consider amiodarone. Do an echocardiograph first to exclude structural heart disease. Radiofrequency catheter ablation, which is usually curative, is indicated for frequent attacks not responding to medical therapy. |
|
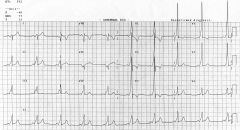
Young pt Usually hereditary Associated with risk of sudden cardiac death Dx? Rx? |
Wolff-Parkinson-White syndrome PR interval <120ms Delta wave – slurring slow rise of initial portion of the QRS QRS prolongation >110ms ST Segment and T wave discordant changes – i.e. in the opposite direction to the major component of the QRS complex Pseudo-infarction pattern can be seen in up to 70% of patients – due to negatively deflected delta waves in the inferior / anterior leads (“pseudo-Q waves”), or as a prominent R wave in V1-3 (mimicking posterior infarction). Rx: Vagal manoeuvres Anti-arrhythmic drugs - to slow the heart rate or to prevent attacks. Electric cardioversion (shock) - to stop a tachycardia attack. Radiofrequency ablation An artificial pacemaker Open-heart surgery - to eliminate the extra pathway. |
|
Diagnosis? |
Atrial fibrillation Irregularly irregular rhythm. No P waves. Absence of an isoelectric baseline. Variable ventricular rate. QRS complexes usually < 120 ms unless pre-existing bundle branch block, accessory pathway, or rate related aberrant conduction. Fibrillatory waves may be present and can be either fine (amplitude < 0.5mm) or coarse (amplitude >0.5mm). Fibrillatory waves may mimic P waves leading to misdiagnosis. |
|
|
Name at least 5 causes of Atrial fibrillation |
Ischaemic heart disease (15%) Hypertension Valvular heart disease (esp. mitral stenosis / regurgitation) Acute infections Electrolyte disturbance (hypokalaemia, hypomagnesaemia) Thyrotoxicosis Drugs (e.g. sympathomimetics) Pulmonary embolus Pericardial disease Acid-base disturbance Pre-excitation syndromes Cardiomyopathies: dilated, hypertrophic. Phaeochromocytoma No cause found in isolated AF - 12% |
|
|
What are the 4 main types of AF? ( think 3 P's) |
First episode – initial detection of AF regardless of symptoms or duration Recurrent AF – More than 2 episodes of AF Paroxysmal AF – Self terminating episode < 7 days Persistent AF – Not self terminating, duration > 7 days Long-standing persistent AF – > 1 year Permanent (Accepted) AF – Duration > 1 yr in which rhythm control interventions are not pursued or are unsuccessful |
|
|
What is the CHADSVASc2 score? |
Congestive Heart Failure = +1 Hypertension = +1 Age in Years: <65 = 0 65-74 = +1 ≥75 =+2 Diabetes Mellitus = + 1 Sex: Male = 0 Female = +1 Vascular Disease History = +1 Stroke/TIA/Thromboembolism = +2 |
|
|
How might you use the CHADSVASc2 score to guide your treatment of AF? |
Score 0 - no therapy or aspirin Sore 1 - oral anticoagulant or aspirin Score 2 - oral anticoagulant Annual Stroke Risk CHADS2 Score Stroke Risk % 0 1.9 1 2.8 2 4.0 3 5.9 4 8.5 5 12.5 6 18.2 |
|
|
What is the role of digoxin, sotalol, flecainide and amiodarone in treating AF? |
Digoxin controls the ventricular rate but does not terminate or prevent attacks. Sotalol, flecainide and amiodarone are used for conversion of atrial fibrillation and maintenance of sinus rhythm. Flecainide should never be prescribed in patients with reduced LV function. Evidence basis: RCTs showed that digoxin was beneficial for lowering the ventricular rate in the short term but no better than placebo in restoring rhythm. Beta blockers and calcium-channel antagonists benefited rate control but verapamil was much less effective than amiodarone at restoring cardiac rhythm. |
|
|
What can be used for rate control in AF? |
1. Atenolol 25 to 100 mg orally, daily OR 1. Metoprolol tartrate 25 to 100 mg orally, twice daily |
|
|
What are the contraindications to using beta-blockers? |
Bronchospasm or predisposition eg allergic disorders (incl rhinitis); Airway obstruction history; Heart failure e.g RVF, RVH, Non-compensated CHF; Sinus bradycardia (< 45-50 beats/min); 2nd, 3rd degree A-V block; shock incl cardiogenic, hypovolaemic; sick sinus syndrome (unless permanent pacemaker in place); severe peripheral arterial circulatory disorders; MI (HR < 45 beats/min, PR interval > 0.24 sec, systolic BP < 100 mmHg +/- mod-severe heart failure); Hypotension; untreated phaeochromocytoma; beta-blocker hypersensitivity; beta-agonist inotropic therapy |
|
|
What side effects should you warn patients about when starting on a beta-blocker |
Fatigue; bradycardia; postural disorder; Raynaud's phenomenon; palpitation; dizziness; headache; GI upset; hypotension; depression; nightmare; weight gain; dyspnoea incl exertional; pruritus; rash; conjunctival xerosis; sleep, visual disturbance; raised free T4; bronchospasm, heart failure deterioration, cardiogenic shock (acute MI), arrhythmia (rare); photosensitivity (very rare) |
|
|
Which patients might you consider using digoxin in for rate control in AF? What dose? |
Elderly sedentary patients Pts with atrial fibrillation and heart failure Where other drugs may be contraindicated or may need to be introduced very slowly (eg beta blockers) Digoxin 62.5 to 250 micrograms orally, daily, according to age, eGFR and plasma digoxin concentration |
|
|
What are the contraindications for using digoxin in AF patients? |
Digitalis glycoside hypersensitivity; intermittent complete heart block; 2nd degree A-V block esp with Stokes-Adams attack history; ventricular tachycardia, fibrillation; arrhythmia induced by cardiac glycoside intoxication; accessory A-V pathway assoc supraventricular arrhythmia eg WPW syndrome unless deleterious electrophysiological effects evaluated; known, suspected accessory A-V pathway without supraventricular arrhythmia history; hypertrophic obstructive cardiomyopathy unless concomitant AF and heart failure |
|
|
What are some of the side effects you should warn a patient about when prescribing digoxin? |
Conduction disorder; arrhythmia incl sinus bradycardia (esp in toxicity in children); PR prolongation, ST segment depression; false +ve ST-T changes during exercise testing; dizziness; drowsiness; headache; confusion; visual disturbance; GI upset; anorexia; rash; thrombocytopenia, gynaecomastia (very rare) |
|
|
What medications might you consider for rhythm control in a patient with AF (new and old but only if certain episode has lasted less than 48 hours)? |
1. Amiodarone 200 to 400 mg orally, 3 times daily for 1 week, then twice daily for 1 week, then 100 to 200 mg orally, daily as an ongoing dose OR 1. Flecainide 50 to 100 mg orally, 2 to 3 times daily (in patients with normal left ventricular function and no coronary disease). |
|
|
What should you know about giving flecainide in a patient with rapid AF? |
If using flecainide, there is a possibility of accelerating the ventricular rate (higher proportion of atrial impulses being conducted through the atrioventricular (AV) node, particularly in atrial flutter). Consider pre-treatment with an AV-nodal-blocking drug (such as digoxin), a beta blocker, verapamil or diltiazem. |
|
|
If oral therapy fails what other options are there for rhythm control in patients with atrial fibrillation and flutter? |
Synchronised electrical cardioversion for atrial fibrillation requires a DC shock, starting with 100 joules in an average adult but consider starting at 200 or even 300 joules in a large patient, or where there is a history of requiring a large shock. Atrial flutter generally requires much less current; start with 50 joules. |
|
|
What should you consider prior to cardioverting a patient (with drugs or shock) for treatment of atrial fibrillation/ flutter? |
ECHO - to rule out clot If a transoesophageal echocardiogram is performed and shows no evidence of thrombus in the atria, it is safe to proceed at once to attempted cardioversion with drugs or direct current (DC) shock. If this is successful, the patient should be anticoagulated (usually with subcutaneous enoxaparin) for at least a few days to reduce the risk of thromboembolism from stunning. If a transoesophageal echocardiogram is not performed, or is done and shows thrombus, cardioversion should not be attempted until the patient has been fully anticoagulated, preferably for 3 weeks. |
|
|
What anticoagulation would you consider using in a patient with AF if indicated by the CHADSVASc2 score? |
If aspirin is indicated, use: aspirin 100 to 300 mg orally, daily. If oral anticoagulation is indicated, use: 1. Warfarin orally, daily according ETG chart then daily dosing adjusted to a target INR of 2 to 3 OR 2. Dabigatran 150 mg orally, twice daily * The dabigatran dose should be reduced to 110 mg twice daily if age is 75 years or more, or there is a potentially higher risk of major bleeding. Do not use dabigatran if estimated glomerular filtration rate (eGFR) is less than 30 mL/min; use warfarin instead. |
|
|
What medication should be used for maintenance of sinus rhythm after electrical, pharmacological or spontaneous cardioversion in patients with AF? |
1. Flecainide 50 to 100 mg orally, twice daily (in patients with normal left ventricular function and no coronary disease) OR 1. Sotalol 40 to 160 mg orally, twice daily OR 2. Amiodarone 200 to 400 mg orally, 3 times daily for 1 week, then twice daily for 1 week, then 100 to 200 mg orally, daily as an ongoing dose. |
|
|
Why is amiodarone second line in maintenance of sinus rhythm for patients with AF despite being more effective? |
Amiodarone has been shown to be the most effective of the drugs above but is listed as second-line because of its long-term adverse effect profile. |
|
|
What should you monitor for in patients on sotalol? |
If using sotalol, monitor for excessive QT prolongation; cease if QT or QTc interval exceeds 500 milliseconds or increases by more than 20% from baseline. Use low doses or not at all in patients with impaired kidney function. |
|
|
What are the adverse effects of amiodarone that you should warn patients about? |
Corneal deposits; photosensitivity; hyper/ hypothyroidism; CNS effects; neuropathy; muscle weakness; pulmonary disorder incl interstitial penumonitis (discontinue), ARDS; QT prolongation; torsades de pointes; bradycardia; sinus arrest; abnormal LFTs, TFTs; GI upset; pancreatitis; dysgeusia; hepatic failure; weight gain; anxiety; SIADH; cerebellar ataxia, benign intracranial hypertension (very rare); blood dyscrasia; severe skin reaction eg SJS, TEN (discontinue); anaphylaxis incl shock |
|
|
What drugs can interact with amiodarone? |
Other QT prolonging drugs esp antiarrhythmics, digoxin; P-gp substrates eg dabigatran; beta-blockers; Ca channel blockers eg verapamil, diltiazem; fluoroquinolones; hypokalaemia inducing drugs eg tetracosactrin, amphotericin, diuretics, corticosteroids, stimulant laxatives; anaesthetics; CYP3A4 substrates eg simvastatin, lovastatin, atorvastatin, cyclosporin, fentanyl, lignocaine, tacrolimus, sildenafil, midazolam, triazolam, ergotamine, dihydroergotamine, colchicine; CYP1A1, CYP1A2, CYP2D6 (eg flecainide), 2C9 (eg phenytoin, anticoagulants incl warfarin) substrates; CYP3A4 (eg grapefruit juice), 2C8 inhibitors; sofosbuvir +/- HCV antivirals eg daclatasvir, simeprevir, ledipasvir (not recommended, monitor cardiac function if coadmin); sofosbuvir +/- HCV antivirals eg daclatasvir, simeprevir, ledipasvir (not recommended, monitor cardiac function if coadmin); highly protein bound drugs (poss); TFTs |
|
|
What are the contraindications to starting flecainide? |
2nd, 3rd degree A-V block or right bundle branch block assoc with left hemiblock (unless pacemaker in situ); cardiogenic shock; asymptomatic premature ventricular contractions and/or asymptomatic nonsustained ventricular tachycardia with MI history; severe renal, hepatic impairment |
|
|
What are the adverse effects of flecainide that you should warn patients about? |
Proarrhythmic effects; conduction disturbances; dizziness; fatigue; rash; constipation; tremor; nervousness; paraesthesia; headache; chest pain; visual disturbance; nausea; dyspnoea; cholestasis, hepatic failure (rare); pulmonary fibrosis (very rare); blood dyscrasia (extremely rare) |
|
Dx? Rx? |
Atrial Flutter Narrow complex tachycardia Regular atrial activity at ~300 bpm Flutter waves (“saw-tooth” pattern) best seen in leads II, III, aVF — may be more easily spotted by turning the ECG upside down! Flutter waves in V1 may resemble P waves Loss of the isoelectric baseline Rx: Refer for both Atrial fibrillation and flutter Medication as per AF |
|
Dx? Clinical significance? |
Premature Ventricular Ectopics/ Complex Clinical significance: PVCs are a normal electrophysiological phenomenon not usually requiring investigation or treatment. Frequent PVCs may cause palpitations and a sense of the heart “skipping a beat”. In patients with underlying predispositions (e.g. ischaemic heart disease, WPW), a PVC may trigger the onset of a re-entrant tachydysrhythmia — e.g. VT, AVNRT/AVRT. |
|
|
Define these terms in regards to PVCs? Unifocal Multifocal Bigeminy Trigeminy Quadrigeminy Couplet Triplet |
Unifocal — Arising from a single ectopic focus; each PVC is identical. Multifocal — Arising from two or more ectopic foci; multiple QRS morphologies. Bigeminy — every other beat is a PVC. Trigeminy — every third beat is a PVC. Quadrigeminy — every fourth beat is a PVC. Couplet — two consecutive PVCs. Triplet — three consecutive PVCs. |
|

Haemodynamically unstable pt Dx? Clinical significance? |
Ventricular tachycardia may impair cardiac output with consequent hypotension, collapse, and acute cardiac failure. This is due to extreme heart rates and lack of coordinated atrial contraction (loss of “atrial kick”). The presence of pre-existing poor ventricular function is strongly associated with cardiovascular compromise. Decreased cardiac output may result in decreased myocardial perfusion with degeneration to VF. Prompt recognition and initiation of treatment (e.g. electrical cardioversion) is required in all cases of VT. |
|
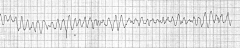
Dx? Rx? |
Ventricular Fibrillation Chaotic irregular deflections of varying amplitude No identifiable P waves, QRS complexes, or T waves Rate 150 to 500 per minute Amplitude decreases with duration (coarse VF -> fine VF) Rx: Advance life support - requires defibrillation |
|

Dx? |
Torsades de points Torsades de pointes (TdP) is a specific form of polymorphic ventricular tachycardia occurring in the context of QT prolongation; it has a characteristic morphology in which the QRS complexes “twist” around the isoelectric line. For TdP to be diagnosed, the patient has to have evidence of both PVT and QT prolongation. TdP is often short lived and self terminating, however can be associated with hemodynamic instability and collapse. TdP may also degenerate into ventricular fibrillation (VF). QT prolongation may occur secondary to multiple drug effects, electrolyte abnormalities and medical conditions; these may combine to produce TdP, e.g. hypokalaemia may precipitate TdP in a patient with congenital long QT syndrome. |