![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
41 Cards in this Set
- Front
- Back

|
Blepharitis Anterior: Chronic inflammation of lid margins Posterior: Posterior lid margin disease affecting meibomian glands Symptoms: Tired, itchy, sore eyes Greasing of cls Cl intolerance General dry eye symptoms Signs: Anterior: Hyperaemia, swelling and crusting of lid margins Scales at base of lashes Reduction in lashes and misdirection Recurrent styes Ulcers Posterior: Obstruction of meibomian orifices Thick, cloudy meibomian secretions Foam in lower tear film Hyperaemia of lid margin |
|
|
Development and cause of blepharitis |
Chronic inflammation of lid margins Anterior, caused by bacterial infection or disorders of sebaceous glands Posterior, changes in meibomian secretions or bacteria. Dry eye disease More prevalent in older pxs, dermatitis poor immune systems, diet, ocular hygiene and dandruff |
|
|
D.O. management of blepharitis |
Artifical tears for comfort Routine referral to optom/CLO/GP if chronic Anterior: Lid scrubs Topical steroids Chloramphenicol if staph (no DO) Posterior: lid massage and bathing Oral tetracycline Advise pxs lid hygiene and warm compresses must become part of daily routine as condition is chronic |
|
|
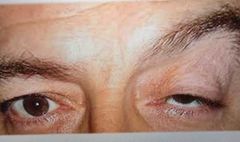
3rd Nerve Palsy Damage to the Oculomotor Nerve Signs: Ptosis Strabismus (down and out) Mydriasis Usually unilateral Symptoms: Sometimes none Diplopia If pupil covered, reduced va Possible pain and headache |
|
|
Development and cause of 3rd Nerve Palsy |
Head injury/trauma Infection Tumour Aneurysm/thrombosis Toxic reaction |
|
|
Differential diagnosis with 3rd Nerve Palsy |
Ptosis only Stroke Nerve palsies Horner's syndrome Sudden onset Diplopia Sudden onset strabismus with pain |
|
|
D.O. management of 3rd Nerve Palsy |
Differentiate with ptosis Question px about ocular pain Any sudden visual changes such as Diplopia or reduced va Lift lid to check pupil Check recent photos for onset See if there is a history Consider ptosis prop Typically there is mydriasis whereas horner syndrome there is miosis |
|
|
Referral for 3rd Nerve Palsy |
Urgent 48 hours if strabismus and ptosis Emergency if pupil involved or orbital/cranial pain |
|

|
Ptosis Dropping of upper eyelid No other pathologies Signs: Unilateral or bilateral Sudden onset or gradual Low position of upper Eyelids Symptoms: Usually none Va reduced if covers pupil Eyestrain or eyebrow ache |
|
|
Development and cause of ptosis |
Can be congenital or acquired Defect in levator palpebrae or its innervation Hypotrophy of muscle, or trauma Occurs in myasthenia gravis |
|
|
D.O. management of ptosis |
GP referral Urgent if pupil covered If acute onset with no other symptoms urgent referral Ptosis prop |
|

|
Horner's syndrome Damage to neurons travelling to face and eyes Signs: Miosis Anhydrosis Ptosis Management: Could be due to a range of associated systemic diseases Urgent referral Emergency if pain |
|

|
Epicanthus Vertical fold of skin covering the inner canthus Signs: Pseudo strabismus No symptoms Differentiate with esotropia/phoria |
|
|
Development and cause of epicanthus |
Part of normal canthal development Varies with ethnicity Some children lose folds as bridge develops |
|
|
D.O. management of epicanthus |
Reassure parent/guardian Discuss importance of routine sight tests Refer to optom if can't confirm orthophoria Urgent if sudden onset squint |
|

|
Pinguecula Degenerative conjunctival lesion Signs: Raised yellowish lesions Does not cross limbus More prominent and yellow with age Can become inflammed (pingueculitis) Symptoms: Asymptomatic Mild foreign body sensation Cosmetic concern Irritation with cls |
|
|
Development and cause of pinguecula |
Can be senile Exposure to UV Welding Cl wear |
|
|
D.O. management of pinguecula |
Px reassured GP referral for surgery UV protection Ocular lubricants for relief GP referral if not resolving |
|

|
Pterygium
Fibrovascular growth from bulbar conjunctiva to invade cornea In early stages Differentiate with pinguecula
Signs: Usually bilateral Starts with small grey opacity near limbus Gradually grows into cornea Generally triangular shaped Pink/red Flattens cornea resulting in ametropic changes Symptoms: Foreign body sensation Irritation Reduced vas Cosmetic concerns Worse with cl wear |
|
|
Development and cause of pterygium |
Age Long term UV exposure Dry, arid climate |
|
|
D.O. management of pterygium |
Advise on UV protection Ocular lubricants If inflamed,urgent referral to GP Refer to HES if threatens visual axis or produces irregular astigmatism Recurrent or chronic inflammation Cosmetic concerns |
|

|
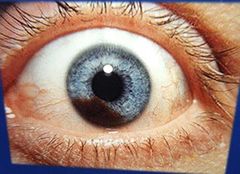
Arcus (senilus) Grayish white band in peripheral cornea with clear separation from limbus No symptoms Fat deposits in the limiting lamellar Not sight threatening and generally seen in older pxs Px reassured and if below 50, refer to GP for health check |
|

|
Naevus Pigmented areas on iris equivalent to freckles. Can be flat or slightly raised and regular in shape Melanocytes clump together No symptoms Differentiate with malignant melanoma Manage with reassurance Monitor for changes |
|
|
Iris melanoma A malignant tumour Signs: Area of iris different in colour May appear thicker and cause distortion of pupil Can bleed Usually Asymptomatic, but if angles blocked, secondary glaucoma |
|
|
Development and cause of iris melanoma |
Uncontrolled growth of melanocytes Can develop from naevi More common for pxs over 50 More prevalent in light coloured irides |
|
|
D.O. management of iris melanoma |
Urgent referral to GP/HES Needs surgery |
|

|
Hordoleum Externum (Stye)
Signs: Painful red swelling on upper or lower lid margin associated with eyelashes May develop a yellow centre
Symptoms: Pain
Caused by bacteria infection of eyelash follicles, invading the glands of Moll causing them to swell
|
|
|
D.O. management of Stye |
Hot compresses Px advised to improve hygiene Refer to GP to test for systemic conditions Antibiotic ointment may be needed |
|

|
Hordoleum Internum Signs: Painful swelling of the Eyelids Red inflamed region of tarsal conjunctiva with a build up of puralence Symptoms: Pain Caused by infection of the tarsal gland by staphyloccal bacteria |
|
|
D.O. management of hordoleum internum |
Hot compresses Surgery may be required |
|

|
Chalazion Signs: Painless swelling in the eyelid Swelling is hard and gets larger Grayish area seen in tarsal conjunctiva Symptoms: No pain, but may put pressure on the cornea causing blurred vision Caused by swelling of tarsal gland perhaps due to blockage of the duct |
|
|
D.O. management of chalazion |
May disappear spontaneously but surgery may be required |
|

|
Dacryocystitis Signs: Inflammation the lacrimal sac Symptoms: Pain if acute Overflow of tears (epiphoria) Caused by infection or blockage of the nasolacrimal duct Treated with systemic antibiotics Hot compresses Surgery may be required |
|

|
Dacryoadenitis Signs: Inflammation of the lacrimal gland Swelling in upper eyelid Symptoms: Pain Acute Inflammation of the lacrimal gland caused by bacteria. Can occur with mumps and glandular fever Treated by antibiotics, and systemic issues investigated |
|

|
Ectropion
Signs: Lower lid margin turned outwards Palpebral conjunctiva becomes dry and red. Cornea may suffer from exposure keratitis Tears run down face
Symptoms: Soreness of cheeks due to tears overflow
Caused by age and loss of muscle tone May need surgery Advise patient not to wipe eyes |
|

|
Entropion Signs: Eyelid margin rolls inward Causes eyelashes to rub against the globe causing inflammation Unilateral or bilateral Symptoms: Pain and lacrimation Loss of vas if cornea scarred Caused by spasm of orbicularis oculai muscle. Scarring of conjunctiva, following severe Conjunctivitis Treated by removal of eyelashes or surgery Adhesion tape to reposition lid margin |
|

|
Xanthelasma Signs: Yellowish masses of fat deposited below the skin along both upper and lower Eyelids Usually bilateral Elderly women most affected Symptoms: None Caused by high levels of cholesterol More common in diabetic patients Advise px to seek medical advice Surgery required if cosmetically unacceptable |
|

|
Contact Dermatitis Signs: A localised allergic reaction causing inflammation of the eyelids and conjunctiva. Blood vessels of the conjunctiva are dilated giving a red appearance. Eyelids Red and puffy Possibly extending to eyelids and cheeks Skin is dry and wrinkled Symptoms: Severe itching of the eye and eyelids caused by contact with cosmetics or eyedrops. Allergic reaction. Px could have rubbed eyes with an irritating substance on their hands Treat with cold compress Steroid drops or skin cream for inflammation |
|
|
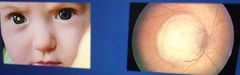
Retinoblastoma Signs: Highly malignant tumour of the retina, usually found affecting children. A white or yellow appearance to the pupil and a raised white mass will be seen on the fundus. Both eyes are often affected and more than one tumour may be present Symptoms: A squint may occur in unilateral cases Can cause secondary glaucoma or iritis Caused by genetic mutation or inherited. Emergency referral |
|

|
Keratoconus Signs: Cornea becomes thinner and bulges into a conical shape Bilateral More common in males Irregular astigmatism Munsons sign: cornea observed from above Symptoms: Px vision becomes more increasingly blurred Some Diplopia possible No real known cause Glasses don't always fully correct RGP cls may be more helpful |
|

|
Basal Cell Carcinoma Signs: Malignant tumour of the skin Commonly found on lower lid Small raised nodule gradually enlarges and leaves a dimple that becomes ulcerated Symptoms: No symptoms in early stages Later the ulcerated centre may bleed Caused by exposure to UV such as the sun or tanning beds forming skin cancer Surgery may be needed. Refer to GP routinely |