![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
150 Cards in this Set
- Front
- Back
|
1. The insulation on the power cord of a pieceof class 1 equipment is faulty such that the active wire is in contact with theequipment casing. What will happen when the power cord is plugged in and thepiece of equipment is turned on A. The double insulationof the device will prevent macroshock when the outer casing is touched B. The electrical fuse will immediately break and disconnect the devicefrom the power supply C. Equipotentialearthing will prevent microshock D. The Line IsolationMonitor will alarm and disconnect power to the device E. The RCD will rapidlydisconnect the device from the power supply |
B? Because the earthed equipment casing will provide a low resistance pathway for conduction resulting in high electrical current. This assumes that there isn't an isolation transformer in the circuit. There is also a fuse in the case. Class I : Equipment in this class makes use of the wire from equipment case to mother earth to provide protection. Class II equipment relies on at least two layers of insulation to provide protection. Class III equipment uses low voltages provided by batteries or special power supplies to be "safe". Lower voltages are considered to be safer than high voltages. |
|
|
2. EZ99 According to the currentANZCA approved standards for labeling, the appropriate colour label for anintraosseous infusion is (some remember it saying INTERosseous, notintraosseous... possibly typo, possibly trick question) A. Yellow B. Beige C. Pink D. Blue E. Red |
C. Pink -> miscellaneous |
|
|
3. PP102 An 8 year old 30kg girlpresents for resection of a Wilms tumour. Her starting haematocrit is 35% andyou decide that your trigger for transfusion will be 25%. The amount of bloodthat she will need to lose prior to transfusion is A. 400mL B. 500mL C. 600mL D. 700mL E. 800mL |
C. MABL = EBV x (HCT – Minimum HCT) / HCT Where EBV = 70ml/kg for child and adult, 80ml/kg for infant, 90ml/kg for neonate
If use average as denominator than exactly 700 |
|
|
4. Repeat:A 30 year-old pregnant patient develops contractions at 30/40 weeks gestationwhich of the following cannot be used for tocolysis A. Clonidine B. Indomethacin C. Magnesium D. Salbutamol E. Nifedipine |
A “Transplacental passage of indomethacin has been shown to be minimalearly in gestation, although it crosses freely near term. This is one reasonindomethacin has always been considered an attractive tocolytic agent before 32weeks.” http://www.gyncph.dk/procedur/ref/obstet/indometacin%202012.pdf
|
|
|
5.A patient known to have porphyria is inadvertently administered thiopentone on inductionof anaesthesia. In recovery the patient complains of abdominal pain, prior to having a seizure and losing consciousness. Which drug should NOT be given? A. Pethidine B. Diazepam C. Haematin D. Suxamethonium E. Pregabalin |
A. From AMPSE
|
|
|
6.A patient with HOCM presents with dyspnoea and angina on exertion. Which of the following is the best agent to treat these symptoms A. Glycerol trinitrate B. Metoprolol C. Morphine D. Hydrochlorthiazide E. Salbutamol |
B. Beta blockers useful to reduce HR and negative inotropy improves coronary perfusion
|
|
|
7.A patient undergoes a femoral-popliteal bypass and has a mildly elevated troponin on day 1 post-operatively. They are otherwise asymptomatic with no other signs/symptoms of myocardial infarction and have an uneventful recovery. What do you do? A. Arrange for a cardiology follow-up and outpatient angiogram because he is at increased risk of future mycocardial infarction B. Arrange coronary angiogram as an inpatient prior to discharge C. Inform the patient that while the result is real the significance is questionable D. Repeat in a weeks time as a second troponin is a better indicator of long-term myocardial infarction risk E. Ignore the result as it is likely a laboratory error |
A. "Kimand colleagues7 measured cTnI on the first 3 postoperative days in patientsundergoing major vascular surgery; 12% had an elevated cTnI on routinepostoperative surveillance although only 3% had AMI according to WHO criteria.They found that a raised cTnI was associated with a six-fold increased risk ofdeath and a 27-fold increased risk of MI in the 6 months following surgery.There was a dose–response relationship between postoperative cTnI concentrationand mortality. Landesberg and colleagues5 demonstrated a substantial increasein perioperative cardiac riskwhen even minor elevations in cTn occur in patients having undergone vascularsurgery. A relationship existed between the finding of ischaemia withcontinuous ECG monitoring and elevations of troponin; the more prolonged theischaemia the greater the cTn increase. Those with the greatest cTnconcentrations had increased chance of a subsequent cardiac event and worselong-term mortality. Even minor elevations in cTn during first threepostoperative days predicted increased risk."Cardiac troponins:their use and relevance in anaesthesia and critical care CEACCP 2008
|
|
|
8. repeat:A 40 year-old lady with a history of a bleeding diathesis presents for a tonsillectomy. What is the most likely cause? A. FactorV Leiden B. ProteinS deficiency C. Haemophilia B D. Antithrombin III deficiency E. ProteinC deficiency |
C. |
|
|
9.What is the most cephalad intervertebral space at which a spinal can be sitedin a neonate where the risk of damage to the spinal cord is minimal A. L1/2 B. L2/3 C. L3/4 D. L4/5 E. L5/S1 |
D. |
|
|
10.St John's Wort (Hypericum perforatum) potentiates the effects of A. Dabigatran B. Heparin C. Warfarin D. Aspirin E. Clopidogrel |
E. Via induction of CYP450 2C9 |
|
|
11.REPEAT: You are performing an awake fibreoptic intubation, through the nose, onan adult patient. In order, the fibrescope will encounter structures with sensory innervation from the following nerves |
Only answer given D. trigeminal, glossopharyngeal, vagus |
|
|
12.A patient is having an electrophysiological study and ablation for atrial fibrillation. Suddenly the blood pressure drops to 76/38 mmHg, with the heart rate at 110 in sinus rhythm. What is the best investigation to confirm thecause of hypotension? A. Troponin B. ST-segment elevation C. Transoesophageal echocardiography D. Coronary Angiogram E. Electrocardiogram |
C. |
|
|
13.Which is the most powerful predictor of atrial fibrillation post cardiac surgery. A. Age B. History ofhypertension C. History of CVA D. History of diabetes E. Time on Bypass |
A. http://eurheartj.oxfordjournals.org/content/30/4/410.full Atrial fibrillation following cardiac surgery: Clinical features and preventative strategies The overall incidence of post-operative AF depends on arrhythmia recording method with the best diagnostic value using continuous ECG monitoring techniques. Advanced age has been shown the best predictive clinical factor, whereas other features, including ECG and echocardiographic parameters, lack a high specificity and positive prediction value. |
|
|
14.A man with a history of Parkinsonsdisease has undergone uncomplicated general anaesthetic for a knee replacement but develops post-operative nausea and vomiting (PONV). He received 4mg dexamethsone intraoperatively as prophylaxis. What would you use to treathis PONV in recovery? A. Dexamethasone B. Prochloperazine C. Metoclopramide D. Droperidol E. Ondansetron |
E. |
|
|
15.Which of the following is of the least benefit in the treatment of severe anaphylaxis? A. Cardiopulmonarybypass B. Nebulised salbutamol C. IV crystalloid D. IV vasopressin E. Subcutaneous adrenaline |
RPA: E RNSH: B or E ? Evidence of less reliable absorption of subcutaneous adrenaline secondary to local vasoconstriction. http://www.rch.org.au/clinicalguide/guideline_index/Anaphylaxis/
|
|
|
16.A 70 year old patient is being treated for congestive cardiac failure. They areable to shower themselves and complete other ADLs but get dyspneoa on mowingthe lawn. They are New York Heart Association classification A. Class 1 B. Class 2 C. Class 3a D. Class 3b E. Class 4 |
B. |
|
|
17.The percentage of post duralpuncture headaches that would resolve spontaneously by 1 week isclosest to A. 90% B. 70% C. 50% D. 30% E. 10% |
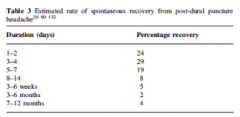
B. |
|
|
18. Which piece of airway equipment is designed for use with a fibreopticbronchoscope A. Aintree B. Cook’s airwayexchange catheter C. Frova introducer D. ? E. ? |
A. Aintree intubation catheter (AIC) is an adaption of the cook airway exchange catheter. It is more malleable and has a larger internal diameter. It is preloaded onto a paediatric bronchoscope and inserted down an LMA. A ETT is then railroaded over the AIC. Frova is basically a bougie with the option to ventilate down it. |
|
|
19.A 50 year old lady is seen at the pre-operative assessment clinic, she is on150mg/day methadone, what is the most likely ECG change to be found in herpre-op ECG? A. Prolonged PR interval B. Prolonged QTc C. ST depression D. U wave E. Tented T-waves |
B. May prolong QT as < mg |
|
|
20.Current guidelines regarding cardiopulmonary resuscitation include all of thefollowing EXCEPT A. Allow equal time forchest compression and relaxation B. Give 2 rescue breath before commencement of CPR C. Chest compression at100bpm D. Chest compressionshould be at least 5cm depth E. Chest compression tobreath ratio at 30:2 |
B. |
|
|
21.When a 3 lead ECG is applied correctly in the CS5 position, you will monitorlead II when you suspect which of the following conditions A. Anterior ischemia B. Inferior ischemia C. Lateral ischemia D. Atrial ischemia E. Posterior ischemia |
B. |
|
|
22.You are anaesthetizing a 50 year old man who is undergoing liver resection forremoval of metastatic carcinoid tumour. He haspersistent intraoperative hypotension despite fluid resuscitation andintravenous octreotide50 ug. The treatment most likely to be effective in correcting the hypotensionis: A. Adrenaline B. [[Dobutamine] C. Levosimenden D. Milrinone E. Vasopressin |
E. CEACCP 2011 Carcinoid: the disease and its implications foranaesthesia:Carcinoid tumors secrete various vasoactive hormones particularlyserotonin and histamine. This results in unpredictable blood pressure swingsand hypotension may be refractory to conventional inotrope and pressor therapy.Octreotide has similar effects to the natural hormone somatostatin.A significant proportion of the surgery related to carcinoid will befor the removal of metastases by hepatic resection. Here, the need to try tomaintain a relatively low CVP, during clamping of the hepatic artery and portalvein to avoid backflow into the liver and venous bleeding, will furtherexacerbate the risk of hypotension. The response to inotropic and vasopressoragents is unpredictable and, in general, drugs such as norepinephrine andepinephrine can be hazardous in carcinoid patients. Norepinephrine has beenshown to activate kallikrein in the tumour and can even lead to the synthesis andrelease of bradykinin resulting paradoxically in further vasodilatation andworsening hypotension, although exaggerated hypertensive responses may be seen.Indeed, any pharmacological stimulation of the autonomic nervous system has thepotential to provoke further problems with vasoactive hormone release. In practice,cautious administration of small doses of phenylephrine has been found helpfulin some patients. Vasoactive hormone release intra-operatively is best treated withintravenous boluses of 20–50 mg of octreotide, titrated to haemodynamicresponse. Vasopressin as an alternative vasoconstrictor that may be useful ifprolonged vasoconstriction is required; however, the evidence base is small. |
|
|
23. Using the American Heart Association specification, the colours of theelectrodes in a 3-lead electrocardiographic (yes the typo is what they used) is A. Right arm = Black;Left arm = White; Left leg = Red B. Right arm = White;Left arm = Black; Left leg = Green C. Right arm = Black;Left arm = Green; Left leg = Red D. Right arm = White; Left arm = Black; Left leg = Red E. Right arm = Red; Leftarm = White; Left leg = Green |
D. |
|
|
24.->AZ84 When performinglaryngoscopy using a Macintosh blade, your best view is of the patient'sepiglottis touching the posterior pharyngeal wall. Using the Cormack and Lehanescale this is grade A. 1 B. 2 C. 3a D. 3b E. 4 |
D. 3a - only epiglottis, but liftable, 3b - only epiglottis and not liftable |
|
|
25.You are doing a supraclavicular brachial plexus block on an awake 35 year-oldlady who is healthy with no significant past medical hsitory. Soon afterinjecting 20mLs of 0.375% ropivicaine she becomes agitated, has a seizure andloses consciousness. Your 1st step in management is A. Intralipid 20%1.5ml/kg bolus B. Midazolam C. Propofol D. Establish airway and give 100% O2 via a facemask E. Feel for radial pulseand give 100mcg adrenaline |
D. |
|
|
26.A G1P0 patient with a dilated cardiomyopathy and an ejection fraction (EF) of35% presents for a caesarean section. The benefits of regional vs generalanaesthesia are A. Decreased heart rate B. Decreased systolicblood pressure C. Increased ejection fraction D. Increased myocardial contractility E. Decreased preload |
C > D C = due to decreased after load |
|
|
27. ET05 A patient has a terminalmalignancy. His family doesn’t want you to tell the patient about his diagnosisand prognosis. Your decision to inform him is an example of: A. Autonomy B. Beneficence C. Confidentiality D. Non-maleficence E. Utilitarianism |
A. Wiki: it is the capacity of a rational individual to make an informed, un-coerced decision. |
|
|
28.A septic patient has a CVP of 12mmHg, a blood pressure of 80/40mmHg and a pulserate of 90/minut:E. Which is the best agent to treat their hypotension A. Dopamine B. Dobutamine C. Noradrenaline D. Adrenaline E. Levosimenden |
C. MAP = (HRxSV) + SVR CVP 12 - implies preload adequate, and presumably SV is normal. HR 90 =reasonable for CO. (ie. neither tachy, nor brady). Therefore decreased SVR is the probable culprit, which also fits the pathophysiology of sepsis. Vasopressor = preferred agent. |
|
|
29.Which organ is least tolerant of ischaemia following removal fortransplantation A. Cornea B. Heart C. Liver D. Kidney E. Pancreas |
B. Different organs exhibit different tolerances to warm and cold ischaemia, in part related to the nature of the organ and in part because of the demands on the organ after transplantation. Hence the heart, which has to function immediately upon transplantation, has the shortest tolerance to cold ischaemia, and each hour beyond the first results in a measurable reduction in survival;38 it should ideally be transplanted in <4 h. This in turn mandates that heart retrieval cannot begin until a suitable recipient has been identified, admitted to transplant centre, and indeed prepared for surgery. Although lungs are slightly more tolerant, with good function to be expected as long as cold ischaemia is <6–8 h, similar principles very often apply. Kidneys, in contrast, need not work immediately and the recipient can be supported on dialysis until they do work. Nevertheless, there is an increased recognition that even kidneys fare better if transplanted as quickly as possible, and ideally within 18 h. The liver and pancreas lie in between and are best transplanted within 12 h. |
|
|
30.You are performing a TAP block. If the needle is correctly positioned wherewill you deposit the local anaesthetic A. Beneath theperitoneum B. Into the transverseabdominus muscle C. Between the transverse adominus muscle and the internal obliquemuscle D. Between thetransverse abdominus muscle and the external oblique muscle E. Between the internaloblique and the external oblique muscle |
C. "The aim of a TAP block is to deposit local anaesthetic in the plane between the internal oblique and transversus abdominis muscles targeting the spinal nerves in this plane." http://www.nysora.com/jnysora/volume12/3170-tapblock.html |
|
|
31. You are inserting a left sided double lumen tube into a 140kg 160cmwoman. At what depth measured at the incisors is it most likely to be in thecorrect position A. 25cm B. 26cm C. 27cm D. 28cm E. 29cm |
D. "The average depth of insertion for both male and female patients 170 cm tall was 29 cm, and for each 10-cm increase or decrease in height, average placement depth was increased or decreased 1 cm." Brodsky JB, Benumof JL, Ehrenwerth J. Depth of placement of left double-lumen endobronchial tubes. Anesth Analg 1991; 73: 570–2 |
|
|
32.A patient is cooled to 33 degrees Celcius in an attempt to improve neurologicaloutcome after out-of-hospital ventricular fibrillation cardiac arrest. Theevidence for this treatment comes from A. Case Reports B. Case Control Studies C. Systematic Review D. Randomized ControlTrial E. Pseudo-randomizedTrial |
C. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004128.pub3/abstract;jsessionid=3306DE06583F0982B1B23B47BF2AB005.f03t02 |
|
|
33. Which of the following decrease during pregnancy A. Functional Residual Capacity B. Forced ExpiratoryVolume in one second C. Tidal Volume D. Respiratory Rate E.Vital Capacity |
A. |
|
|
34.You are anaesthetizing a patient with chronic renal failure for removal of aTenkoff catheter and have intubated using rocuronium at a dose of 1.2mg/kg. Youare immediately unable to intubate or ventilate and you decide to reverse thepatient with sugammadex. What dosage would you use A. 2mg/kg B. 4mg/kg C. 8mg/kg D. 12mg/kg E. 16mg/kg |
E. Adult dosage guides (a) Reversal of shallow neuromuscular blockade induced by rocuronium* Use Bridion at a dose of 2 mg/kg (reversal likely within 1.2 and 1.5 minutes) (b) Reversal of profound neuromuscular blockade induced by rocuronium* Use Bridion at a dose of 4 mg/kg (reversal likely within 2.3 and 3.3 minutes) (c) Immediate reversal of neuromuscular blockade induced by rocuronium* Use Bridion at a dose of 16 mg/kg (reversal likely within 5.7 and 6.7 minutes) |
|
|
35.During an elective thyroidectomy a patient develops symptoms consistent withthe diagnosis of “thyroid storm” which of the following treatment options inNOT appropriate A. Carbimazole B. Beta-blocker C. Propythiouracil D. Plasmaphoresis E. Hydrocortisone |
D>A. Endocrine practitioner 2010 Jul-Aug; 16(4): 673-3. Successful treatment of thyroid storm with plasmapheresis. Medscape – rarely as a life saving measure plasmapheresis has been used to treat thyroid storm in adults. www.anaesthesia.med.usyd.edu.au/resources/lectures/thyroid_tmc.html Carbimazole: Prodrug. Rapid onset of anti-thyroid effect but clinical effect takes 3-4 weeks due to fact does not block peripheral conversion of T3 to T4. Therefore, stores must be depleted first. Also only available in PO form.
|
|
|
36.A young female patient with anorexia nervosa, had just started eating again.After three days she develops dyspnea and is found to have cardiac failure.Which of the following is the most important to correct A. Potassium B. Chloride C. Phosphate D. Glucose E. Sodium |
C. |
|
|
37.(repeat) A pregnant lady is undergoing neuroradiological coiling of a cerebralaneurysm. At what gestational age should you monitor foetal heart rate toensure adequate uteroplacental blood flow A. 20 weeks B. 24 weeks C. 28 weeks D. 30 weeks E. 32 weeks |
B. CEACCP Anaesthesia for non-obstetric procedures during pregnancy 2012 |
|
|
38.(repeat) What is the mechanism of central sensitisation? A. Increasedintracellular magnesium B. Antagonism of theNMDA receptor C. Glycine is the majorneurotransmitter involved D. Recurrent a-deltafibre activation E. Alteration in gene expression |
E. |
|
|
39.Which of the following is the best predictor of a difficult intubation in amorbidly obese patient A. Pretracheal tissue volume B. Mallampati score C. Thyromental distance D. BMI E. Severity of OSA |
A. (old question – neck circumference) Neck circumference, though now there is a question of the utility of pretracheal tissue thickness as a possible surrogate as measured by ultrasound. Morbid Obesity and Tracheal Intubation (Anesth Analg 2002) |
|
|
40.A female patient with a history of COPD presents for lung volume reduction surgery, which of the following is a contraindication for surgery (? indicates a poor prognosis) A. Age > 60 years B. Chronic asthma C. Evidence of bullous disease on CT scan D. FEV < 25% E. Long-term prednisolone 10mg/day |
D. Oxford Handbook of Anaesthesia 3e p 367 "Generally accepted minimum preoperative values of FEV1 for the following procedures are (as % of predicted value): · pneumonectomy >55% lobectomy >40% · wedge rescetion >35%
|
|
|
41.A patient with known metastatic lung cancer is found to have hypercalcaemia, all of the following would help excretion of calcium except A. Bisphosphates B. Calcitonin C. Frusemide D. Sodium Chloride E. IV crystalloids |
A. Bisphosphonates: inhibit osteoclast activity thereby causing a fall in plasma calcium. But, also produces a decrease in renal excretion of calcium. Calcitonin: produced by parafollicular cells of the thyroid, acting to oppode the effects of parathyroid hormone. Works via 3 mechanisms: inhibition of intestinal calcium absorption, inhibition of bone osteoclast activity, and inhibition of renal tubular cell resorption of calcium, thereby increasing urinary excretion Frusemide: potent loop diuretic acting at the Na/K/2CL cotransporter in the thick ascending limb of the loH. Twofold action: allows for aggressive fluid loading and also some effect on decreased renal calcium resorption. NaCL - Renal excretion of Na results in concurrent Ca excretion via increased RBF. IVT - Increased renal Ca excretion
|
|
|
42.What potentiates/interacts with adenosine A. Aspirin B. Warfarin C. Clopidogrel D. Dabigatran E. Dipyrimadole |
E>D. MIMS say severe reaction with dipyridamole but; 1. This drug blocks the cellular uptake of adenosine, thereby increasing the concentration of adenosine at its receptors. 2. By enhancing the effects of intravenous adenosine, dipyridamole may make the recommended initial bolus dose of adenosine unsafe.
|
|
|
43.A 2 year-old child has just undergone strabismus surgery. They had an URTI 1/52prior to surgery. They had an uneventful general anaesthetic with a 4.5mmcuffed ETT, was extubated and sent to recovery. 20 minutes later they developrespiratory distress. Their saturations are 96% on room air, and there isnoticeable tracheal tug. What is the most appropriate initial management thatwill help with their respiratory distress A. Apply CPAP via a facemask B. Propofol 1mg/kg C. Dexamethasone0.4mg/kg D. Gas induction andreintubate E. Nebulized adrenaline (1:1000) 0.5mL/kg |
A > E. as "initial management" CEACCP 2008, Tracheal extubation. Laryngospasm: Most common cause of upper airway obstruction and mostly in children due to extubation in light planes of anaesthesia. Mx; Oxygen, jaw thrust, clear secretions, CPAP, propofol (20% induction dose) and sux (0.5mg/kg to relieve obstruction) Oedema: Risk factors: difficult intubation, surgery > 1h or coughing on ETT CEACCP 2007 Acute Stridor in Children. Clinical signs generally occur within 30mins of extubation and respond well to treatment with nebulised epinephrine (0.5ml/kg 1:1000) and iv dexamethasone 0.25mg/kg, warm humdified oxygen or heliox. |
|
|
44.Which antihypertensive is not safe to use in pregnancy A. Aspirin B. Enalapril C. Metoprolol D. Hydralazine E. Nifedipine |
B. "Enalapril has been assigned to pregnancy category D by the FDA for use during the second and third trimesters and to category C during the first trimester. Animal and human data have revealed evidence of embryolethality and teratogenicity associated with ACE inhibitors. There are no controlled data in human pregnancy. Congenital malformations have been reported with the use of ACE inhibitors during the first trimester of pregnancy, while fetal and neonatal toxicity, death, and congenital anomalies have been reported with the use of ACE inhibitors during the second and third trimesters of pregnancy" |
|
|
45.Which has the weakest evidence for prevention of postoperative infection A. Intraoperative low inspired O2 B. Intraoperative blood transfusion C. Intraoperative hypothermia D. Intraoperative hyperglycaemia E. Cigarette smoking |
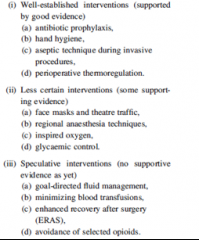
B.
|
|
|
46.During a cerebral aneurysm clipping, the anaesthetist can assist with theplacement of the clip by giving the patient which drug immediately prior toclipping A. Nimodipine B. Thiopentone C. Hypertonic saline D. Adenosine E. Mannitol |
D. |
|
|
47.The POISE trial showed that the perioperative administration of metoprolol XR resulted in decreased A. Perioperativemortality B. Hypotension C. Congestive CardiacFailure D. Myocardial Infarction E. Stroke |
D.
|
|
|
48.In paediatric trauma, the Broselow tape is used to estimate A. Blood loss B. Weight and drug dosages C. Urine output D. Abdominal girth E. Head circumference |
B. http://en.wikipedia.org/wiki/Broselow_Pediatric_Emergency_Tape The Broselow Tape relates a child’s height as measured by the tape to his/her weight to provide medical instructions including medication dosages, the size of the equipment that should be used, and the level of shock voltage when using a defibrillator. |
|
|
49.Which of the following should be used by a lay person to indicate that theyshould commence CPR A. Absence of central pulse B. Absence of peripheral pulse C. Loss of consciousness D. Absence of breathing E. Obvious airway obstruction |
D>C It is loss of consciousness and abnormal breathing |
|
|
50.A patient presents for dilation of a pharyngeal stenosis postlaryngopharyngectomy 12 months earlier. After inducing anaesthesia you site asize 7 reinforced ETT in the stoma. Over the next 30 minutes the patient gradually desaturations. Despite hand bag ventilation and an increased FiO2 of1 the saturations remain at 88%. This is due to A. Endobronchial intubation B. Aspiration C. Tension Pneumothorax D. Circuit leak E. Blockage of ETT withsecretions |
A. Group consensus |
|
|
51.PiCCO determines cardiac output utilizing A. Thermodilution B. Pulse contouranalysis C. Thermodilution and pulse contour analysis D. ? Doppler E. ? |
C. |
|
|
52.During scoliosis surgery with monitoring of somatosensory evoked potentials, which tract are they mainly monitoring A. Anterior horn B. Anterior corticospinal tract C. Dorsal column D. Spinothalamic tract E. Lateral corticospinaltract |
C. |
|
|
53.(repeat) patient has suffered flash burns of the upper half of the left upperlimb, all of the left lower limb and the anterior surface of the abdomen. The approximate percentage of the body surface which has been burned is A. 18% B. 23% C. 32% D. 41% E. 48% |
C. Upper half of left upper limb = 4.5% Left lower limb = 9% front + 9% back = 18% Anterior surface of abdomen = 9% Total = 18 + 9 + 4.5 = 31.5% |
|
|
54. Complications of mediastinoscopy include all of the following except A. Air embolism B. Cardiac laceration C. Pneumothorax D. Recurrent laryngeal nerve palsy E. Tracheal compression |
B cardiac lac |
|
|
55. A 70 year old man with severe mitral stenosis and normally in sinus rhythm, is going for an ORIF of fractured radius and uln:::A. Soon after induction of GA, he develops a tachyarrhythmia with BP 70/40mmHg and HR 130bpm. The most appropriate immediate action is A. Amiodarone B. Adenosine C. IV fluid bolus D. Adrenaline E. Direct cardioversion |
E. |
|
|
56. The time constant of the alveoli is A. Resistance multiplied by compliance B. Resistance divided by compliance C. Resistance plus compliance D. Resistance minus compliance E. |
A. |
|
|
57. The MAC awake:MAC ratio of sevoflurane is closest to A. 0.22 B. 0.34 C. 0.45 D. 0.76 E. 1.00 |
B |
|
|
58.Abnormal Q waves occur in all the following EXCEPT A. Digitalis toxicity B. LBBB C. Recent transmural MI D. Wolff-Parkinson-White E. Previous MI |
A. |
|
|
59. Patient complains of numbness in the anterior 2/3 of tongue after GA with LMA. Most likely nerve injured is A. Glossopharyngeal B. Facial nerve C. Mandibular D. Superior vagus E. Maxillary nerve |
C. Lingual nerve of V3 and taste chords tympani taste branch if facial nerve |
|
|
60. A 70 year old man with non-valvular atrial fibrillation is taken off his warfarin for 7 days prior to surgery and has no bridging therapy. His daily risk of stroke is A. 0.001% B. 0.01% C. 0.1% D. 4% E. 10% |
B. |
|
|
61. In patient with ankylosing spondylitis which of the following is INCORRECT A. Amyloid renal infiltration is rarely seen B. Cardiac complications occur in < 10% C. Normocyctic anaemia occurs in 85% of cases D. Uveitis is the most common extra-articular presentation E. Sacroilitis is an early sign of presentation |
C. - only 15% are anaemic |
|
|
62. Which of the following are NOT useful in the management of Torsades de Pointes A. Isoprenaline B. Procainamide C. DCCV D. Electrical pacing E. Magnesium |

B. – prolongs QT |
|
|
63. Compared with a plenium vaporizer what is NOT a disadvantage of draw-over vaporizer (repeat but still not quite remembered correctly) A. Basic temperature compensation B. Basic flow compensation C. Cannot use sevoflurane D. Small volume reservoir E. ? |
C. |
|
|
64. The desflurane vaporizer is heated because of its A. High SVP B. High boiling point C. Low SVP D. High MAC E. Low MAC |
A. |
|
|
65. The thermoneutral zone in a neonate in degrees celcius is A. 26-28 B. 28-30 C. 30-32 D. 32-34 E. 34-36 |
D. |
|
|
66. Which of the following is most effective way to reduce renal failure in AAA surgery A. Fluid bolus prior to aortic clamping B. Fluid bolus after aortic clamp release C. Frusemide D. Minimize cross-clamp time E. Mannitol |
D. |
|
|
67. Which type of aortic dissection can be managed conservatively/non-operatively A. Debakey 1 B. Debakey 2 C. Stanford A D. Stanford B E. Stanford C |
D. |
|
|
68. The most likely cause of death after pharyngeal, oesophageal or tracheal perforation is A. Air embolus B. Hemorrhage C. Failure to intubate D. Failure to ventilate E. Sepsis |
E. |
|
|
69. An essential criteria for diagnosis of left bundle branch block (LBBB) on ECG is A. RSR in V1 B. Minimum duration QRS of 0.2 secs C. Deep slurred S wave in V6 D. Loss of septal Q waves in V5 and V6 E. T waves opposite direction to main direction of QRS |
D. |
|
|
70. If a patient experiences parasthesia in the little finger during supraclavicular brachial plexus block, the needle is in proximity to the A. Posterior cord B. Middle trunk C. Ulnar nerve D. Lower trunk E. Medial cord |
D. |
|
|
71. Which of the following are feature of Conn's syndrome? A. Hypoglycaemia, hyponatremia, hyperkalemia B. Hypoglycaemia, hypernatremia, hypokalemia C. Normoglycaemia, hypernatremia , hypokalemia D. Normoglycaemia, hyponatremia, hyperkalemia E. Hyperglycaemia, hyponatremia, hyperkalemia |
C. |
|
|
72 Commonest valvular heart disease seen in pregnancy is A. Aortic stenosis B. Aortic regurgitation C. Mitral Stenosis D. Mitral regurgitation E. Tricuspid reguritation |
C. |
|
|
73. Incidence and severity of vasospasm following sub-arachnoid haemorrhage is seen maximally at A. 0-24 hrs B. 2-4 days C. 6-8 days (note 5-7 days in the old question) D. 7-10 days E. 2 weeks |
D. CEACCP – greatest risk is 4-10days |
|
|
74. The predominant pathology seen in restrictive heart disease is A. Diastolic dysfunction B. Systolic dysfunction C. Valvular dysfunction D. ? E. ? |
A. |
|
|
75. What is the first sign/symptom seen with an inadvertent total spinal whilst performing caudal anaesthesia in a neonate A. Hypotension B. Bradycardia C. Desaturation D. Tachycardia E. Loss of consciousness |
C. |
|
|
76. Which of the following is an absolute contraindication to electroconvulsive therapy A. Cochlear implant B. Epilepsy C. Pregnancy D. Raised Intracranial Pressure E. Recent myocardial infarct |
D. |
|
|
77. SG65 Prolonged Trendelenburg (head-down) positioning causes which of the following A. No change in intracranial pressure B. No change in intraocular presssre C. No change in pulmonary venous pressure D. Increased myocardial work E. Increased pulmonary compliance |
D. |
|
|
78. Performed a brachial plexus block. Normal sensation still remains in medial forearm. Which part of brachial plexus is most likely to have been missed A. Posterior cord B. Anterior division C. Median brachial cutaneous nerve D. Ulnar nerve E. Inferior trunk |
E. |
|
|
79. A 29 year old female undergoes craniotomy for posterior fossa tumour. Which of the following is an absolute contraindication to the sitting position A. Patent ventriculo-atrial shunt B. Previous back surgery C. Pacemaker D. Small patent foramen ovale E. Oesophageal stricture contraindicated for transoesophageal echocardiogram |
A. |
|
|
80. A 4 year old child booked for minor surgery is seen in pre-admission clinic where a murmur is detected. Which feature will warrant further investigation A. Loudness 4/6 B. Decreases on inspiration C. Vibratory quality D. Ejection systolic murmur E. Louder on supine |
A. |
|
|
81. The autonomic supply of the ciliary ganglion is such that it A. Receives its sympathetic nerve supply from the cervical ganglion B. Receives its parasympathetic nerve supply from the trochlear nerve C. Is located inferiorly in the orbit D. Is at risk from injury during peribulbar nerve block E. Receives parasympathetic nerve supply from the Edinger Westphal Nucleus |
E. |
|
|
82. Regarding Thallium Stress Testing in predicting perioperative cardiac events A. A positive result requires further investigation with a pulmonary artery catheter B. It has a high negative predictive value C. It has a low negative predictive value D. It has a high positive predictive value E. Thallium Stress testing is considered inferior to Dobutamine Stress Echo |
B. Up-to-date:Thallium-Dipyridamole stress testing – Sensitivity 83%, Specificity 49%,NPV98%, PPV 18%. Preferred in arrhythmias as dobutamine can induce arrhythmias |
|
|
83. An elderly gentleman on warfarin has suffered a subdural haematom:::A. His INR on admission was 4.5. The resident in Ed has already given him 2.5mg of Vit K. To reverse his coagulopathy prior to urgent surgery you should give him A. Factor VIIa B. FFP C. Cryoprecipitate D. Prothrominex E. Prothrombinex and FFP |
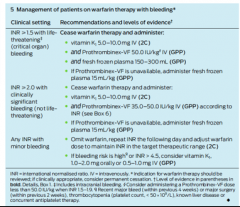
E. |
|
|
84. During caesarean section a meconium stained floppy apnoeic baby is delivere:D. When the midwife gives you the baby, it is apnoeic, cyanotic with heart rate of 90 bpm. What do you do next A. Give naloxone B. Dry and stimulate C. Start chest compressions D. Give positive pressure ventilation E. Suction the trachea |
E. |
|
|
85. A 70 year old lady suffered a subdural haematoma. She is currently confused and the neurosurgeon wants to take her to theatre for urgent decompression. She is a vague historian, but from notes you find out she had ablation and pacemaker put in 7 months ago - DDD mode. Cardiac technician in 1 hour away and the surgeon wants to proceed. What do you do A. Postpone until cardiology review B. Postpone until pacemaker checked by technician C. Postpone until temporary pacemaker inserted D. Proceed after having implemented external pacing E. Proceed with magnet available |
E. Stone et al. Perioperative management of patients with cardiac implantableelectronic devices BJA 2011 |
|
|
86. New blood pressure measuring device is develope:D. Best was to compare it to the current gold standard A. SCUSUS B. Bland Altman Plot C. Kendall Coefficient of Concordance D. Pearsons coefficient E. Friedmans ?? |
B. |
|
|
87. What happens when you place a magnet over a biventricular internal cardiac defibrillator A. Switch to asynchronous pacing B. Damage the internal programming C. Nothing D. Switch off antitachycardia function E. Switch of rate responsiveness |
D |
|
|
88. A 54 year-old patient is on warfarin for AF. They have a history of alcohol abuse and liver failure with a bilirubin of 28 and an albumin of 30. He also has a history of DVT following a flight. What is his CHADS2 score A. 0 B. 1 C. 2 D. 3 E. 4 |
A. |
|
|
89. A full size C oxygen cyclinder (size A in New Zealand) has pressure regulated from A. 16000kpa to 400kpa B. 16000kpa to 240kpa C. 11000kpa to 400kpa D. 11000kpa to 240kpa E. ? |
A. |
|
|
90. What is approximately the systolic blood pressure in an awake neonate (mmHg) A. 55 B. 70 C. 85 D. 100 E. 115 |
B. |
|
|
91. A 25 year male with a history of asthma who is usually on fluticonasone and salbutamol nebs presents with an acute exacerbation. On examination you see he is distressed, RR 26 bpm. On auscultation: poor air entry and polyphonic wheeze bilaterally. ABG: pH 7.45, pCO2 27, pO2 75, HCO3 24. He has been treated with salbutamol and ipratropium nebules and intrasvenous hydrocortison:E. What is the next step in his treatment A. Inhaled helium/oxygen B. IV aminophylline C. IV magnesium D. IVsalbutamol E. Intubation and ventilation |
C. CEACCP 2008 Management of life threatening asthma in adults |
|
|
92. You are doing an awake fibreoptic intubation and having difficulty identifying the anatomy of where you ar:E. Then you observe a trifurcation. The lobe of the lung to which this airway is conected is A. LUL B. Lingula C. RUL D. RML E. RLL |
C. |
|
|
93. A 35kg 5 year old girl is having elective surgery for suturing of a superficial leg laceration. After induction with N2O/Sevoflurane/O2 and in absence of any visible veins you have placed an appropriately sized LM:::A. Following this her SpO2 immediately drop to 90%. What is your initial management A. Remove LMA and increase inspired Sevoflurane concentration B. Increase inspired Sevoflurane concentration through the LMA C. Give sublingual Suxamethonium D. Give intramuscular Atropine E. Give intramuscular Suxamethonium |
A. |
|
|
94. Ulcerative colitis is associated with all of the following EXCEPT: A. Cirrhosis B. Iritis C. Psoriasis D. Arthritis E. Sclerosing cholangitis |
C. |
|
|
95. Regarding rotameters EZ85 A. The bobbin is contained in a tube with parallel sides B. There is laminar flow at high flows C. The height of the bobbin is directly proportionate to the pressure drop across the bobbin. D. There is a constant pressure difference across the bobbin at all flows. E. Resistance increases at high flows |
D. |
|
|
96. You see a man in his 60s in clinic 1 week prior to laparoscopic cholecystectomy. He has dilated cardiomyopathy with an ejection fraction of 30%, but does not get dyspnoeic with normal activities of daily living. What is the most appropriate management of his heart failure? A. Amiodarone 100mg bd B. Digoxin 250mcg daily C. Enalapril 2.5mg bd D. Metoprolol 100mg bd E. Diltiazem slow release 240mg daily |
C. |
|
|
97. The best clinical indicator of severe aortic stenosis is A. Presence of a thrill B. Mean pressure gradient of 30mmHg C. Area 1.2cm2 D. Slow rising pulse E. ESM radiating to the carotids |
RPA A |
|
|
98. Atrial Septal Defect murmur is heard due to blood flow through A. Tricuspid valve B. Pulmonary valve C. Mitral valve D. Aortic valve E. Atrial Septal Defect |
B. |
|
|
99. At what valve area do you begin to get symptoms at rest, with mitral stenosis? A. 4.5 cm2 B. 3.5 cm2 C. 2.5 cm2 D. 1.5 cm2 E. 1.0 cm2 |
RPA E LVP D POW D. Circulation 2005: Symptoms at rest correlate to class IV NYHA disease. This occurs in severe disease at valve area <1cm2 . This is different to onset of ANYsymptoms with exertion that can begin with mild disease. OHCA: Symptom free until valve area 1.6-2.5cm ”ACC/AHA PracticeGuidelines. Guidelines for the Management of Patients With Valvular Heart Disease: The normal mitral valve area is 4.0 to 5.0 cm2. Narrowing of the valve area to <2.5 cm2 must occur before development of symptoms. A mitral valve area>1.5 cm2 usually does not produce symptoms at rest. However, if there is anincrease in transmitral flow or a decrease in the diastolic filling period,there will be a rise in left atrial pressure and development of symptoms. Thus,the first symptoms of dyspnea in patients with mild MS are usually precipitatedby exercise, emotional stress, infection, pregnancy, or atrial fibrillation with a rapid ventricular response
|
|
|
100. Nitrous oxide anaesthesia may cause all of the following EXCEPT A. An increased incidence of myocardial ischaemia B. Decreased leukocyte chemotactic response C. Elevation of plasma homocysteine levels D. Megaloblastic anaemia E. Reversible inhibition of methionine synthetase |
E. CEACCP 2005 Nitrous OxideProlonged administration of nitrous oxide causes irreversible inhibition of methionine synthetase, which results in interference with DNA synthesis in both leukocytes and erythrocytes.
|
|
|
101. The diagnosis of neuroleptic malignant syndrome requires the presence of A. Diaphoresis B. Elevated plasma creatine kinase C. Hypertension D. Muscle rigidity E. Tachycardia |
D. DSM 4 – must have elevated temp and severe rigidity
|
|
|
102. Regarding tryptase level testing for suspected anaphylaxis, all are true EXCEPT: A. Levels peak within 1 hour B. Increased with anaphylactoid and anaphylactic reactions C. 99% of the body’s stores are found in mast cells D. Levels of > 20ng/mL are suggestive of anaphylaxis E. Test should be repeated at 24-48 hours |
E. |
|
|
103. An 18 month old boy presents for surgery for an incarcerated inguinal hernia. On examination you note that he has had an URTI for approximately one week. Your advice regarding surgery should be A. Postpone the surgery for two weeks B. Proceed with surgery under spinal anaesthetic C. Proceed with surgery with a full course of antibiotics to treat the URTI D. Undertake surgery, but avoid the use of an ETT E. Proceed with surgery with careful monitoring |
E. |
|
|
104. The incidence of fat embolism syndrome following a unilateral closed femoral fracture is A. 0 -3% B. 4 – 7% C. 8 -11% D. 12 – 15% E. 16 - 19% |
A. CEACCP 2007 fat embolismà "patientswith a single long bone fracture have a 1–3% chance of developing the syndrome,but it has been reported in up to 33% of patients with bilateral femoral fractures."
|
|
|
105. The thoracodorsal nerve arises from A. A Medial cord of brachial plexus B. Lateral cord of brachial plexus C. Posterior cord of brachial plexus D. Dorsal scapular nerve E. Long thoracic nerve |
C. |
|
|
106. SN19 Neurosurgery operation in the sitting position. MAP 80mmHg, CVP 5mmHg, the transducers are located 13cm below the external auditory meatus. What is the CPP? *Note - I specifically remember that 70mmHg was an option* A. 62 mmHg B. 65 mmHg C. 67 mmHg D. 72 mmHg E. 75 mmHg |
B. CPP = MAP or ICP=CVP. Presume ICP = 0 secondary to open cranial vault. Therefore MAP = 80 - (13 x 1.3) (conversion from mmHg to cmH2O) = 70. Therefore CPP = 70 - 5 = 65 but both transducers at same level therefore CVP 0 at head therefore CPP = 70
|
|
|
107. A man attending his daughter's wedding is involved in fight with his son-in-law. He does not know where he is, opens eyes to voice, but removes tie when instructed. What is his GCS? A. 10 B. 11 C. 12 D. 13 E. 14 |
D. M6V4E3 |
|
|
108. Which of the following drugs is least likely to cause hypoxia in ARDS A. Noradrenaline B. Milrinone C. Isoprenaline D. Isoflurane E. Sodium nitroprusside |
RPA A LVP A POW A |
|
|
109. What is the best predictor of poor prognosis with aortic stenosis? A. Chest pain B. Paroxysmal nocturnal dyspnoea C. Syncope D. Palpitations E. Fatigue |
B. Patients die within anaverage of 5 yrs after onset of angina, 3 yrs after onset of syncope and 2years after onset of heart failure symptoms |
|
|
110. Pierre-Robin sequence is characterized by cleft palate, micrognathia and A. Craniosynostosis B. Macroglossia C. Glossoptosis D. Microstomia E. ? |
C. |
|
|
111. After 3 litres of normal saline, the dilutional anaemia is initially offset by A. Increased cardiac output B. Increased oxygen extraction C. Capillary vasodilation D. ? E. ? |
A. |
|
|
112. Anaesthetic Machine is left on all weekend with flow rate of oxygen at 6 litres/min. A Desflurane vaporiser is placed on it on Monday morning without changing the CO2 absorber. What is the most likely toxic product produced? A. Ca(OH)2 B. Carbon dioxide C. Carbon monoxide D. Compound A E. Compound B |
C. |
|
|
113. 2ml of 0.75% ropivacaine is injected for an interscalene block. Soon after the patient loses consciousness. The most likely place of inadvertent injection is A. Subdural B. Internal jugular vein C. Common carotid artery D. External jugular vein E. Vertebral artery |
A>E as first is LOC other MCQ very similar but with seizures etc which will be VA injection |
|
|
114. An 18 month old infant is undergoing a routine spontaneously breathing GA with an LMA. They have a sudden onset of SVT with a heart rate of 220 and a BP of 84/60 with an ETCO2 of 32 and SpO2 of 98. The best management strategy is A. Adenosine 100mcg/kg B. DCR 2J/kg C. DCR 4J/kg D. Amiodarone 5mg/kg E. CPR |
A. |
|
|
115. When stimulating the ulnar nerve with a nerve stimulator, which muscle do you see twitch A. Opponens abducens B. Abductor pollicis brevis C. Adductor pollicis brevis D. Extensor pollicis E. Flexor pollicis brevis |
C. |
|
|
116. A middle-aged male with severe mitral stenosis having general anaesthesia for repair of fractured ulna/radius. Ten minutes into the case you notice a tachyarrythmia with his HR 130 and BP 70/-. He is normally in sinus rhythm. What do you do A. Adenosine B. Amiodarone C. Shock D. Volume E. Metaraminol |
C. |
|
|
117. Circuit disconnection during spontaneous breathing anaesthesia A. Will be reliably detected by a fall in end-tidal carbon dioxide concentration B. Will be detected early by the low inspired oxygen alarm C. Will be most reliably detected by spirometry with minute volume alarms D. May be detected by an unexpected drop in end-tidal volatile anaesthetic agent concentration E. Can be prevented by using new, single-use tubing |
D. |
|
|
118. ET04 An 85 year old patient with a bleeding disorder (? haemophilia) suffers a fractured neck of femur (#NOF). You discuss the possibility of a needing a blood transfusion but despite your explanation they refuse because they are scared of CJD infection post transfusion. Subsequently you decide not to proceed with the case because of the high risk of bleeding. The ethical principle that this is an example of is A. Paternalism B. Coercion C. Justice D. Beneficience E. Autonomy |
A. |
|
|
119. A type I diabetic is fasting pre-operatively and you decide to place them on an IV insulin infusion to optimize their perioperative glycaemic control. Their BSL is 7 mmol/L. By what mechanism does the insulin infusion decrease their BSL A. Stimulates glucose uptake into the liver B. Stimulates glucose uptake into skeletal muscle C. Inhibits glucose production in the liver D. Decreases glucose absorption from the gastrointestinal tract E. Inhibit glucagon release |
RPA B LVP C BJA article MARC POW E |
|
|
120. Patient has undergone a bilateral lung transplant. All of following are impaired EXCEPT A. Mucociliary clearance B. Cough reflex distal to anastomosis C. Hypoxic pulmonary vasoconstriction D. Response to CO2 E. Lymphatic drainage |
C. |
|
|
121. Patient with history of long QT syndrome treated with long term propranolol. How do you know the treatment is effective A. Normal QTc B. No further prolongation of QT in response to valsalva manoeuvre C. ? D. ? E. ? |
B. BJA 2003 Long QT Syndrome and Anaesthesia
Or HR<130 when exercising |
|
|
122. A neonate is born with meconium stained liquor but is vigorous and crying. The reason for not suctioning the pharynx is A. Hypertension B. Hypotension C. Bradycardia D. Tachycardia E. ? |
C. |
|
|
123. What organism most commonly causes meningitis post spinal anaesthesia A. Staphylococcus epidermidis B. Staphylococcus aureus C. Streptococcus pneumonia D. Streptococcus salivarius E. Escherichia coli |
D. CEACCP 13 No 2 Postnatal neurological problems 2013
Most common epidural abscess staph aureus |
|
|
124. A male patient has a haemoglobin of 8g/dL and reticulocyte count 10%. The most likely diagnosis is A. Untreated pernicious anaemia B. Aplastic anaemia C. Acute leukaemia D. Anaemia of chronic disease E. Hereditary spherocytosis |
E. |
|
|
125. An advantage of supraclavicular block over an interscalene nerve block for shoulder surgery A. Less phrenic nerve block B. Easier landmarks in obese patient C. Arm can be in any position for block D. Less risk pneumothorax E. Better cover for shoulder surgery |
A. |
|
|
126. A patient with a head injury is found to have a unilateral dilated pupil with no direct or consensual response to light. What is the most likely diagnosis A. Global injury B. Optic nerve injury C. Horners syndrome D. Transtentorial herniation E. Injury to the pons |
D. |
|
|
127. EM68 In an arterial line system A. Overdamping exaggerates mean pressure B. Underdamping increases mean pressure C. Underdamping underestimates systolic pressure D. Wide range of damping coefficient associated with good performance if system has high natural frequency E. Compliant tubing is good |
D. Miller's Anaesthesia Chapter 40The accuracy of adirectly recorded arterial pressure waveform is determined by the naturalfrequency and damping coefficient of the pressure monitoring system. Optimaldynamic response of the system will be achieved when the natural frequency ishigh, thereby allowing accurate pressure recording across a wide range ofdamping coefficients. |
|
|
128. The commonest postoperative complication in a patient with a neck of femur fracture (#NOF) is A. UTI B. Pneumonia C. Myocardial Infarction D. Delirium E. ? |
D. ANZCA Blue book 2007 Anaesthesia and Hip Fracture: A Review of the CurrentLiterature |
|
|
129. Which of the following is an advantage of a bronchial blocker of a double lumen tube A. Able to isolate separate lobes B. Significantly easier to deflate non-ventilated lung C. Better suited to pneumonectomy D. Less pressure on bronchial tissue E. Lower incidence of tube malpositioning |
A. |
|
|
130. Laser endotracheal tubes A. More resistant to ignition when covered in blood B. Resistant to electrosurgical cautery C. Wont ignite when touched by laser D. Have larger external diameter for same internal diameter relative to standard PVC tubes E. Have double cuffs which are resistant to puncture by laser |
D. |
|
|
131. Pulsus paradoxus in cardiac tamponade, the blood pressure decreases A. Every second beat B. In expiration when increase is normal C. In expiration more than normal subjects D. In inspiration when increase is normal E. In inspiration more than normal subjects |
E. http://www.kerrybrandis.com/wiki/mcqwiki/index.php?title=Pulsus_paradoxus"Under normal conditions, arterial blood pressure fluctuates throughout the respiratory cycle, falling with inspiration and rising with expiration. Therefore, during inspiration the fall in the left ventricular stroke volume is reflected as a fall in the systolic blood pressure. The converse is true for expiration. During quiet respiration, the changes in the intrathoracic pressures and blood pressure are minor. The accepted upper limit for fall in systolic blood pressure with inspiration is 10 mmHg. The “paradox” refers to the fact that heart sounds may be heard over the precordium when the radial pulse is not felt. This is due to an exaggeration of the normal mechanisms mentioned above. Moreover, the clinical method of assessment of this "pulse" is by measurement of the "systolic blood pressure". |
|
|
132. You are anesthetizing a patient for a laparotomy who has a history of pulmonary hypertension. Regarding the patients anaesthetic management A. An alpha-agonist is the inotrope of choice B. Hypothermia is protective against a rise in pulmonary artery pressure C. Isoflurane will tend to decrease pulmonary artery pressure D. Ketamine is an appropriate anaesthetic agent E. ? RHF |
A Paul Forrest Westmeadhandbook states alpha agonists should be avoided Inodilators such as Milrinoneand dobutamine will cause systemic vasodilation and hence reduce coronaryperfusion pressure, which limits their utility. SVR should be maintained toprevent coronary ischaemia to right side of heart. |
|
|
133. In a patient with severe rheumatoid arthritis, which radiological finding is most consistent with severe atlantoaxial instability (? C1/C2 instability) A. A 9mm gap between the anterior arch of C1 and the odontoid peg B. Increased saggital diameter C. Posterior atlantodental interval of > 14mm D. Midpart of C1 over C2 E. Tear drop sign of C2 |
A. PADI is the distancebetween posterior surface of the odontoid and the anterior margin of theposterior ring of the atlas. At all cervical levels cord requires minimum canalwidth of 10mm; CSF 2mm, dura 2mm. Thus, minimum PADI of 14mm is needed to avoidcord compression |
|
|
134. You are called to the labour ward to assist in the manual removal of a retained placenta in a healthy woman. The obstetrician asks you to administer intravenous glycerol trinitrate. An initial safe dose, that you would expect to be effective, would be A. 5mcg B. 50mcg C. 250mcg D. 500mcg E. 1000mcg |
B. |
|
|
135. What is the most accurate method of determining foetal heart rate in a neonate A. Palpation of an umbilical vein pulse B. Auscultation with a stethoscope C. Palpation of the femoral artery D. Pulse oximetry E. ? |
B. |
|
|
136. Definitive evaluation of malignant hyperthermia (MH) susceptibility does NOT include observing A. Abnormalities on magnetic resonance imaging (MRI) spectroscopy B. Calcium release from B lymphocytes in response to caffeine stimulation C. Certain mutations in the ryanodine receptor gene D. Myofibrillar necrosis on muscle biopsy plasma E. Creatine kinase (CK) levels above 800 units/L |
?A or E ANZCA Blue Book 2005 MH Investigation for the Uninitiated Overall, the balance of opinion leads to the conclusion that serum CK levels are not sensitive or specific enough to be useful for diagnosis in individual patients.
|
|
|
137. A 60 year-old man with anterior mediastinal mass, is having a mediaastinoscopy. During induction they lose cardiac output, desaturate and drop their ETCO2. What is the best management strategy A. Adrenaline B. CPR C. CPB D. Place prone E. ? |
D. |
|
|
138. Which is true of Eaton-Lambert syndrome that differentiates it from myasthenia gravis? A. Immune antibodies against post-synaptic ion channels B. Associated with thymoma C. Repeated exercise causes weakness to initially improve D. Good response to edrophonium E. Resistant to non-depolarizing muscle relaxants |
C. The Eaton-Lambert Syndrome (ELS) is a rare condition in which weaknessresults from a pre-synaptic abnormality of ACh release at the neuromuscularjunction. It is classically associated with small cell carcinoma of the lung althoughrecent evidence suggests up to 50% may be free from underlying malignancy. The clinical presentation is that of proximal weakness with absentreflexes, sometimes with bulbar and facial muscle involvement. Importantly the weakness tends to improve with muscle contraction, unlikeMG. ELS treatment consists of treatment of underlying malignancy if present,improving neuromuscular transmission with drugs, and immunosuppression. |
|
|
139. A 55 year-old man presents to the emergency department with an obviously infected heel ulcer - BP 100/60, PR 110/minute, temperature 35.8, Na 125, K 2.7, BSL 55, Creatinine 180. Which do you give first/most urgently? A. Antibioitcs B. Crystalloid C. Insulin D. Potassium E. Adrenaline |
A>B surviving sepsis is give antibiotics. Likely HONK |
|
|
140. A new test has been developed to diagnose a disease. To determine the SPECIFICITY of this new test it should be administered to A. A mixed series of patients i.:E. some known to be suffering from the disease and some known to NOT be suffering from it B. A series of patients known to NOT be suffering from the disease C. A series of patients known to NOT be suffering form the disease and an estimate of the prevalence of the disease in the population obtained D. A series of patients known to be suffering from the disease E. A series of patients known to be suffering from the disease and an estimate of the prevalence of the disease in the population obtained |
B. |
|
|
141. During one lung ventilation, hypoxaemia can occur. The cause for this is: A. Loss of hypoxic pulmonary vasoconstriction B. Perfusion of the unventilated lung C. Ventilation perfusion mismatch of the ventilated lung D. Atelectasis of the ventilated lung E. Upper lobe collapse of the ventilated lung |
B. |
|
|
142. A child with intra-operative blood loss. A cardiac arrest is most likely because of A. A delay in delivery of blood from the blood bank B. Inadequate intravenous access C. Underestimated intra-operative blood loss D. Underestimated pre-operative hypovolaemia E. Complication of transfusion |
C. |
|
|
143. The lumbar plexus supplies all of the following EXCEPT: A. Subcostal nerve B. Obturator nerve C. Lateral cutaneous femoral nerve D. Long saphenous nerve E. Iliohypogastric nerve |
A. |
|
|
144. The symptom indicating poorest prognosis in an adult patient with aortic stenosis A. Chest pain B. Malaise C. Palpitations D. Paroxysmal nocturnal dyspnoea E. Syncope |
D (NB:This is the SAME question as the one numbered 109.)
|
|
|
145. A 50 year old male in recovery after an anterior cervical fusion, developing increasing respiratory distress, bulge under original incision, combative, repeatedly removing oxygen mask, SpO2 96%. What is the most appropriate management A. Aspirate the collection with a 19G needle and syringe B. Awake fibreoptic intubation with minimal sedation C. Direct laryngoscopy and intubation after sevoflurane/O2 gaseous induction D. Direct laryngoscopy and intubation after propofol/suxamethonium induction E. Intubation via intubating LMA |
RPA, LVP, POW = C. |
|
|
146. RB67 Regarding post dural puncture headache, all of the following are true, EXCEPT: A. If puncture with the tuohy needle during epidural insertion, subsequent blood patch is 30-50% effective B. Caffeine is often used to treat mild headache C. Subdural haemorrhage can occur rarely D. ? E. Unlikely to be post dural puncture headache if the headache is only in the occipital area |
E>A blood patch is only 30-50% effective |
|
|
147. A 70 year-old male presents for right lower lobectomy. Preoperative spirometry shows FEV1 2.4L (4.2L predicted), FVC 4L (5L predicted). The predicted post-operative FEV1 is: A. 1.0L B. 1.3L C. 1.7L D. 1.9L E. 2.2L |
C. |
|
|
148. What is the most important immediate treatment for a cardiac arrest due to ventricular fibrillation in a patient with hypertrophic obstructive cardiomyopathy? A. Adrenaline B. Amiodarone C. Defibrillation D. Intubation, ventilation and oxygenation E. Precordial thump |
C. |
|
|
149. Hypercalcaemia due to hyperparathyroidism is associated with A. A shortened PR interval B. A prolonged QTc interval C. Muscle rigidity D. Polyuria and polydipsia E. Increased glomerular filtration rate |
D. |
|
|
150. The cause of early mortality (early - within 30 minutes) in a pregnant women with amniotic fluid embolism is A. Bronchospasm B. Hypovolaemia C. Malignant arrhythmia D. Pulmonary hypertension E. Pulmonary oedema |
D. |