![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
Pre-eclamptic woman, BP 170/110, headache, proteinuria 1.2g. Which of the following NOT to use for control of her hypertension: |
A
ANCZA SIG – “Safe agents include methyldopa, labetalol, nifedipine and some β-adrenoceptor blockers (METOPROLOL, pindolol, propranolol). Atenolol is not recommended due to fetal growth restriction. Angiotensin converting enzyme inhibitors (ACE-I) and angiotensin type II receptor blockers are contraindicated (Abalos et al 2006, Level I; Podymow & August 2008, Level IV; Rowe 2008, Level IV)” SNP and GTN not ideal, but can be used for acute hypertension control |
|
|
Male with a Haemoglobin of 8G% and reticulocyte count 10%. Possible diagnosis:
A. Untreated pernicious anaemia B. Aplastic anaemia C. Acute leukaemia D. Anaemia of chronic disease E. Hereditary spherocytosis |
E
Wiki - Spherocytosis: “A cause hemolytic anemia characterized by the production of red blood cells (RBCs), or erythrocytes, that are sphere-shaped, rather than bi-concave disk shaped. Spherocytes are found in hereditary spherocytosis and autoimmune hemolytic anemia” |
|
|
Commonest organism causing meningitis post spinal:
A. Staph epidermidis B. Staph salivarius C. Staph aureus D. Strep pneumoniae |
B |
|
|
Exponential decline / definition of time constant (with various options)
A. time for exponential process to reach log(e) of its initial value B. Time until exponential process reaches zero C. Time to reach 37% of initial value D. Time to reach half if its initial value E. 69% of half life |
C
Time constant is the time taken for the amount of something to fall to 1/e of the initial amount The number "e" equals 2.718281828. 1/e = 0.368. Therefore the time constant is the time it takes for the concentration/amount to fall to 36.8% of the initial value (approx 37%) |
|
|
Relative humidity – air fully saturated at 20 %. What is the relative humidity at 37 degrees ?
A. 20 B. 30 C. 40 D. 50 E. 60% |
C |
|
|
A 50 year old man with multiple fractures. The BEST parameter to monitor volume resuscitation is:
A. Heart rate B. LVEDV C. PCWP D. RVEDV E. Changes in R atrial pressure during inspiration |
B LVEDA does not predict responders well. SVV, pulse pressure variation (systolic-diastolic) and the 'delta down' of systolic pressure variation all perform well.
SVC collapsibility index might be better (also using TOE) |
|
|
Anaphylaxis to rocuronium. Which is most likely to cause coss-reactivity ?
A. Vecuronium B. Pancuronium C. Atracurium D. Cisatracurium E. None of the above -cross reactivity too variable to predict |
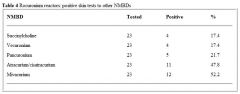
E |
|
|
Hypotension post propofol induction in elderly patient. More pronounced / profound than in younger patient. Reason ?
A. Concentric LVH associated with ageing and therefore preload dependent B. Because of increased lean body mass C. Decreased cardiac output with ageing D. Increased sensiticity to all anaesthetic agents, thus relative overdose is common E. Decreased liver blood flow with ageing, decrease drug clearance and increased drug concentration |
A |
|
|
Predictive factors for mortality in elderly patient (except):
A. Aortic stenosis B. Diabetes mellitus C. Elevated Creatinine D. Cognitive dysfunction E. Type of surgery |
D |
|
|
The best clinical indicator of SEVERE AS
A. Presence of thrill B. Mean Gradient 30mmHg C. Area 1.2 cm2 D. Slow rising pulse and ESM radiating to carotids E. Shortness of breath |
A |
|
|
Elderly patient. Indications for pre Femoro-Popliteal Bypass angiogram include all EXCEPT:
A. Severe heart failure B. Suspicion of L main disease C. Symptomatic tachyarrhythmia D. Unstable angina E. Stable angina with positive thallium |
C |
|
|
How do you minimise risk of intravenous cannulation with epidural insertion ?
A. Injection saline through epidural needle before catheter insertion B. Lie patient lateral C. Do CSE D. Thread catheter slowly E. |
A
|
|
|
Timing of peak respiratory depression post intrathecal 300 mcg morphine:
A. < 3.5 hours (think it was one hour) B. 3.5 – 7.5 hours (then three hours) C. 7 - 12.5 hours (then 7.5 - 12.5 hrs) D. 12.5 -18 hours E. > 18 hours |
B |
|
|
Patient with aortic dissection. Blood pressure 150/90. Best drug to control BP:
A. Captopril B. Esmolol C. GTN D. Hydralazine E. SNP |
B
eMedicine: • Aggressive management of heart rate and blood pressure should be initiated. • Beta-blockers should be given initially to reduce the rate of change of blood pressure (dP/dt) and the shear forces on the aortic wall. • The target heart rate should be 60-80 beats per minute. • The target systolic blood pressure should be 100-120 mm Hg. |
|
|
Type of dissection – which is classically for NON-operative management:
A. DeBakey Type I B. DeBakey Type II C. Stanford A D. Stanford B E. Stanford C |
D |
|
|
TURP – patient under spinal. Confused. ABG: Na+ 117 / normal gas exchange. Treatment ?
A. 10 ml 20% Saline as fast push IV B. 3% NS 100 ml/h C. Normal saline 200 ml/h D. Frusemide 40 mg IV E. Fluid restrict 500 ml/day |
B
|
|
|
Male undergoing trans-sphenoidal surgery. Now Na+ 155mmol/l and thirsty with polydypsia. Treatment:
A. Desmopressin (DDAVP) B. Fluid restrict C. Aldosterone D. E. |
A
|
|
|
The STRONGEST stimulus for ADH secretion:
A. High serum osmolality B. Low serum osmolality C. Hypovolaemia D. High serum Na E. |
C |
|
|
Stellate ganglion block. Needle entry next to SCM muscle at C6. Which direction to advance needle ?
A. C3 B. C4 C. C5 D. C6 E. C7 |
D
|
|
|
Thermoneutral zone in 1 month old infant ?
A. 26 – 28 degrees Celcius B. 28 – 30 degrees Celcius C. 30 – 32 degrees Celcius D. 32 – 34 degrees Celcius E. 34-46 degrees celcius |
D
|
|
|
A 60 year old man describes orthopnoea. On examination: pansystolic murmur (at LSE)/ displaced apex beat. Likely diagnosis ?
A. Mitral regurgitation B. ? C. D. E. |
A
|
|
|
A 4 year old child with VSD (repaired when 2 years old) for dental surgery. What antibiotic prophylaxis do the guidelines recommend?
A. Amoxycillyn orally B. Amoxycillin IV C. Cephazolin IV D. Amoxycillin / gentamicin E. No antibiotics required |
E
|
|
|
A 4 year old child with Arthrogrophysis multiplex congenita for dental surgery. Jaw rigidity post induction. Likely cause ?
A. Temporomandibular joint involvement/ TMJ rigidity B. Inadequate depth of anaesthesia C. Inadequate muscle relaxation/ inadequate sux D. Masseter spasm E. ? |
A |
|
|
A 78 year old man with past difficult intubation for arm surgery. Supraclavicular block with 25 mls 0.5% bupivacaine. Shortly after begins convulsing. INITIAL management?
A. Midazolam 5mg B. Intralipid 20% 1.5 ml/kg C. Thiopentone 150mg D. Suxamethonium 50mg E. Propofol 50mg |
A |
|
|
Advantages of bronchial blockers over double lumen tubes:
A. Able to achieve lobar isolation B. Lower cuff pressure C. Quicker deflation of isolated lung D. Pneumonectomy E. Lower incidence of malposition |
A |
|
|
Patient for pneumonectomy. Pre op FEV1 2.4. (Predicted 4.5L) FVC given as well. For R lower lobectomy. Postoperative predicted FEV1 ?
A. 1.3 B. 1.5 C. 1.7 D. 1.9 E. 2.2 |
C
19 lung segments in total - 10 on the right (RUL=3, RML=2, RLL=5), and 9 on the left (LUL=3, Lingula=2, LLL=4). Therefore for a right lower lobectomy we will be removing 5 segments, and therefore be left with 14 segments. The ppoFEV1 will be 14/19 x 2.4L = 0.7368 x 2.4L = 1.77L Or, based on the numbers used in Miller there are 42 segments in total: 22 segments (or subsegments) in the right lung (RUL=6, RML=4, RLL=12), and 20 in the left lung (LUL=10, LLL=10). The calculation is the same, but with different numbers: A right lower lobectomy will remove 12 segments, and we will be left with 30. Therefore ppoFEV1 will be 30/42 x 2.4L = 0.7143 x 2.4L = 1.71L |
|
|
Post accidental dural puncture with epidural needle. Headache. Which does NOT fit ?
A. Epidural blood patch 30-50% effective B. Unlikely to be related to epidural if purely occipital headache C. Caffeine mildly effective in reducing headache D. Subdural haematoma can rarely occur with PDPH E. (?something about photophobia) |
A
• A - Epidural blood patch is about 60-70% effective (long-term, higher initially) according to most articles, so I say A=false. • B - Post-dural puncture headache can be frontal, fronto-temporal, or occipital. The BJA CEACCP article from 2001 states that "The headache does not occur in any specific distribution within the cranium". Therefore B=false. • C - Caffeine does have some initial benefit in reducing headache, but this does not seem to be prolonged (see article by Ghaleb). C=True. • D - Subdural haematoma is a rare complication of accidental dural puncture following epidural (see articles from Int J Obstet Anesth and Anaesthesia & Intensive Care). D=True . |
|
|
Cell saver. Which does NOT get filtered ?
A. Foetal cells B. Free Hb C. Platelets D. Clotting factors E. Microaggregates of leukocytes |
A
Cell salvage filters the following substances: • Free haemoglobin • White blood cells • Plasma • Platelets • Heparin • Clotting factors • Complement Foetal cells (particularly fetal RBC's) are NOT filtered/removed, and are spun down with maternal RBC's (ie the process does not differentiate between maternal and fetal RBCs) and then reinfused into the mother. However, the risk of alloimmunisation is thought to be no greater than that occurring during a normal vaginal delivery. The risk of amniotic fluid embolism is also thought to be very low - so much so that cell salvage in obstetrics has been endorsed by the Obstetric Anaesthetists Association, AAGBI, NICE and CEMACH in the UK, as well as the ASA in America. |
|
|
You are on a humanitarian aid mission in the developing world. Drawover vaporiser apparatus described being used. Given 400 mm tubing, OMV or diamedica vaporiser, 200mm tubing attached to self-inflating bag. Which other ONE piece of equipment is ESSENTIAL to make this system functional?
A. Halothane B. In-line Waters' Cannister [1] C. Non-rebreathing valve D. Oxygen source E. Ventilator |
C
The keyword here is "functional". You don't need volatile agent for the circuit to be functional and there are other ways of providing anaesthesia even in 3rd world countries. I was going to go with oxygen, however it also says "self-inflating bag" which means fresh gas flow is not required and flow of gas in the circuit would be promoted by the self inflation of the bag provided there is a unidirectional flow valve on it. The Waters' Canister is a CO2 absorbing canister and is not required for functionality, nor is a ventilator if the anaesthetist has arms and legs to squeeze the bag with. The answer must be C - non-rebreathing valve |
|
|
Regarding post craniotomy pain:
A. Local infiltration proven to reduce long-term pain B. Local more painful than discrete nerve blocks C. Local infiltration more efficacious than discrete nerve blocks D. Local infiltration more efficacious than opioid analgesia E. Local infiltration more efficacious with clonidine included |
A & B
From APMSE book: • "Local infiltration "...reduces incidence of subsequent chronic pain." (Level 2) - so option A is correct. • Nerve blocks are less painful than discrete blocks so option B is correct. • Local infiltration not more efficacious, so incorrect • No difference in anlagesia between scalp infiltration and morphine or fentanyl • There is also a comment in that section in the book that: "Clonidine did not improve analgesia after supratentorial craniotomy", so option E is wrong |
|
|
A 60 year old female is undergoing hysterectomy. Gabapentin reduces postoperative:
A. Nausea B. Vomiting C. Sedation D. Pruritus E. Constipation |
A
Vomiting and pruritis also, but nausea specifically with hysterectomy From APMSE: • Peri-op gabpentinoids reduce the incidence of vomiting, pruritis and urinary retention, but increase the risk of sedation • After hysterectomy and spinal surgery specifically, gabapentin improved pain relief and was opioid sparing, nausea was less in patient with hysterectomy, and there was no difference in sedation |
|
|
Burns dressings. The following is proven to be of analgesic benefit:
A. Morphine gel B. Biosynthetic dressings (the answer per pain book) C. Dexmedetomidine IV D. Lignocaine IV E. Cognitive/Distraction technique |
B & E
Though only B is level 1 evidence According to APMSE: • The use of biosynthetic dressings is associated with a decrease in time to healing and a reduction in pain during burn dressings changes (N) (Level I [Cochrane Review]). • Opioids, particularly via PCA, are effective in burn pain, including procedural pain (S) (Level II). • Augmented reality techniques (N) (Level II), virtual reality or distraction techniques (N) (Level III-3) reduce pain during burn dressings. • Gabapentin reduces pain and opioid consumption following acute burn injury (N) (Level III-3) • PCA with ketamine and midazolam mixture provides effective analgesia and sedation for burn dressings (N) (Level IV). |
|
|
Subtenon’s block. What is the worst position to insert block?
A. Inferonasal B. Inferotemporal C. Superonasal D. Supertemporal E. Medial / canthal |
C
A sub-Tenon's block can be done in any of the 4 quadrants (options A-D above). However: Continuing Education in Anaesthesia, Critical Care & Pain | Volume 5 Number 3 2005 "There is individual variation in the disposition of blood vessels, but they congregate in the apex of the orbit. There is a view that the inferotemporal and medial parts of the orbit are relatively poorly supplied with blood vessels, whereas the superonasal region is relatively vascular." |
|
|
Liposuction. Infiltration of lignocaine with 1:200,000 adrenaline. Peak plasma concentration of lignocaine occurs at:
A. 1 hour B. 3 hours C. 18 hours D. 24 hours E. 30 mins |
C
Different values quoted:: • 5-17 hours postoperatively – sPlasma lidocaine levels and risks after liposuction with tumescent anaesthesia. Acta Anaesthesiol Scand. 2005 Nov;49(10):1487-90 • 11-15 hours postoperatively – eMedicine |
|
|
Child-Pugh score. Components ?
A. Bilirubin / albumen / INR (yes INR, not PT), ascites, encephalopathy B. Various other options including AST/ALT, GGT, PT C. ? D. ? E. ? |
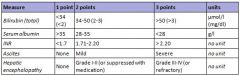
A
The score employs five clinical measures of liver disease. Each measure is scored 1-3, with 3 indicating most severe derangement |
|
|
Which is NOT a disadvantage of drawover vaporiser versus plenum vaporiser:
A. Temperature compensation B. Cannot use sevoflurane C. Small volume reservoir D. Flow compensation E. |
B
All are disadvantages, presuming A is talking about its lack of compensation. Though seems it function ok if temp >1 to <50 degrees Drawover vaporisers are • "simple to assemble and use, and can operate without fresh gas supplies. They are lightweight and portable" • Not well compensated for temperature (ok between 1-50 degrees) • very difficult to use with sevoflurane - "Sevoflurane (Sevorane) has been used in draw-over, but its use is hampered by a need to deliver high percentages which are at the upper limits of simple vaporiser performance capabilities...using additional wicks to maximise output can be helpful, but latent heat of vaporisation rapidly cools the system and lowers performance...two OMV vaporisers are required to provide adequate concentrations for induction” • equipped with a small volume reservoir • variable with regards to flow compensation Advantages: • Simplicity of concept and assembly • No need for pressurised gas supply regulators and flow meters • Minimum FiO2 is 18-21% • Robust reliable and easily serviced • Low cost • Portable Disadvantages: • Decreasing familiarity with technique/equipment • Vaporiser limitations • Filling systems not agent specific (can be an advantage) • Basic temperature compensation affecting performance at extremes (>1 to <50 degrees they maintain their accuracy) • Less easy to observe spontaneous ventilation with self inflating bag • Cumbersome in paediatric use |
|
|
Acute renal failure. Which is not an indication for dialysis ?
A. Hyperkalaemia B. Metabolic alkalosis C. Hypernatraemia D. Uraemic pericarditis E. APO |
B
CEACCP article: Indications for continuous renal replacement therapy Classical: Volume overload Metabolic acidosis (pH < 7.1) Hyperkalaemia (>6.5 mmol litre�1) Symptomatic uraemia (Pericarditis, encephalopathy, bleeding dyscrasia) Dialysable intoxications (e.g. lithium, ethylene glycol, methanol, aspirin, theophylline, vancomycin, procainamide) Hyperthermia (cooling) Alternative: Endotoxic shock Hypothermia (rewarming) SIRS (pancreatitis, ARDS) Nutritional support Hepatic failure Deliberate hypothermia Severe dysnatraemia (<115 mmol litre-1, >165 mmol litre-1) Traumatic rhabdomyolysis Plasmapheresis (Guillain–Barre syndrome, myasthenia gravis, thrombotic thrombocytopaenic purpura) |
|
|
Chronic alcohol use. Which is not an associated complication?
A. AF B. hypertriglyceridemia C. Macrocytosis D. Nephrotic syndrome E. Pancreatic Ca |
D |
|
|
Chest xray shown of patient post Left pneumonectomy with heart swung to left side. Management:
A. Increase PEEP B. Roll onto right side C. Turn on suction to left pleural catheter D. Lung biopsy E. |
B |
|
|
Salicylate poisoning:
A. Respiratory acidosis B. Metabolic acidosis (/ don’t think this was an option - ak )(yep i think it was- mm) C. Increased CO2 (production) D. High output renal failure E. Hyperthermia (/ pretty sure this option was HYPOthermia - too late) |
B |
|
|
New onset atrial fibrillation in a 10 week pregnant lady. BP 150/90, HR 160, SaO2 92%. Moderate mitral stenosis on TTE, no thrombus seen. Emergency doctor gave her anticoagulant (not specified what). Most appropriate management:
A. Verapamil B. Labetalol 20mg iv to 300mg C. Amiodarone 300mg IV D. Synchronised biphasic cardioversion with 70-100 Joule E. Oral digoxin -1000mcg then 500mcg 6 hrs later |
D
|
|
|
Patient post anterior cervical fusion. Patient in recovery. Confused and combative. Nurse concerned about haematoma Taken to theatre: Most appropriate way of securing airway:
A. Gas induction / laryngoscopy / intubate B. Awake tracheostomy C. Awake fibreoptic intubation using minimal sedation D. Thiopentone, suxamethonium, direct laryngoscopy and intubation E. retrograde intubation |
A
Awake fibreoptic would be safe, but probably impossible in an awake patient Awake tracheostomy seems extreme, and would presumably also be difficult I think A is a safer option than D, though could potentially be difficult in the combative patient |
|
|
Young asthmatic male in emergency department. RR 26, pCO2 27, SAO2 92%, struggling talking in sentences. Given nebulised salbutamol, and ipratropium, 200mg IV hydrocortisone. After 30 minutes - no improvement. Further management:
A. IV salbutamol B. IV aminophylline C. IV magnesium D. Intubate and ventilate E. ? |
C |
|
|
Called to emergency department to review a 20 y/o male punched in throat at a party. Some haemoptysis / hoarse / soft voice. Next step in management:
A. CT to rule out thyroid cartilage fracture B. XR to rule out fractured hyoid C. Rapid sequence induction / laryngoscopy / intubation D. Awake fibreoptic intubation E. Nasendoscopy by ENT in emergency department |
A |
|
|
How quickly does the CO2 rise in the apnoeic patient?
A. 1 mmHg per min B. 2 mmHg per min C. 3 mmHg per min D. 4 mmHg per min E. 5 or ?8 mmHg per min |
C
From Miller, 1st minute Co2 increases by 6 mm Hg all subsequent minutes 3 -4 mm Hg |
|
|
Long-standing T6 paraplegia. All present EXCEPT ?
A. Flaccid paralysis B. Poikilothermia C. Autonomic hypereflexia D. Labile BP E. Hyperkalaemia with suxamethonium |
A
|
|
|
Young female patient for tonsillectomy with history of bleeding tendency. Which is the most likely cause?
A. Factor V Leiden B. Protein C deficiency C. Haemophilia B (Christmas disease) D. Antithrombin III deficiency E. Lupus anticoagulant |
C |
|
|
Amniotic fluid embolism. Cause of death in first half hour ?
A. Pulmonary hypertension B. Malignant arrhythmia C. Pulmonary oedema D. Hypovolaemic shock E. |
A
|
|
|
Hypocalcaemia – earliest sign:
A. Tingling of face and hands B. Chvostek’s sign C. Carpopedal spasm D. E. |
A
Wikipedia page on hypocalcaemia says this is the earliest sign |
|
|
Elderly COAD patient. On home oxygen. 24 hours of worsening condition. Various blood gases given:
A. paO2 > 50, paCO2 70 HCO3 30 etc… B. C. D. E. |
A
|
|
|
Visual loss with pupillary reflexes retained. Likely cause ?
A. Retinal detachment B. Occipital mass C. Frontal mass D. Chiasmal mass E. Optic neuritis |
B
Cortical blindess = visual loss but with retained pupillary reflexes and normal fundoscopy. Caused by pathology in the occipital lobes |
|
|
Nerve block for anaesthesia over anterior 2/3 of ear?
A. C2 B. Mandibular nerve C. Maxillary nerve D. Ophthalmic nerve E. Vagus |

B |
|
|
Complex regional pain syndrome. What proportion of patients have motor involvement ?
A. 0 % B. 25 % C. 50 % D. 75 % E. 95 % |
D |
|
|
Malignant hyperthermia. The number of people in the community at any given time with a predisposition is called the:
A. Prevalence B. Incidence C. D. E. |
A
Incidence measures the rate of occurrence of new cases of a disease or condition. Prevalence measures how much of some disease or condition there is in a population at a particular point in time |
|
|
Patient with Hx COAD and suspected pneumonia – clinical findings supporting R pneumonia on examination:
A. R Dull percussion note & increased vocal resonance B. R Dull percussion note & decreased vocal resonance C. R Decreased air entry D. Tracheal deviation to left E. Tracheal deviation to right |
A
|
|
|
Thallium scan:
A. High negative predictive value B. High positive predictive value C. Not as good as a dobutamine stress echocardiography D. E. |
A |
|
|
A 50 y/o male diabetic admitted to intensive care with pneumonia. Intubated and ventilated. Extensive results given. BP 80/-, HR 120, CVP 4, PCWP 6, SvO2 69% PaO2 80, BE -4 pH 7.2. Management:
A. Blood transfusion B. Bicarbonate infusion C. Fluid resuscitation D. Adrenaline infusion E. Insulin infusion |
C
Haemodynamic variables suggest hypovolaemia |
|
|
Young female having cholecystectomy. Venous air embolus:
A. Mechanical ventilation and PEEP is part of treatment strategy B. Most likley to occur at initial gas insufflation, but can occur at any time C. Inert gas (argon, xenon) is safer D. E. |
B |
|
|
LUSCS for failure to progress. Spinal is inserted uneventfully. Next day the patient has foot drop. The most likely cause is?
A. epidural haematoma B. lumbosacral palsy C. sciatic nerve palsy D. common peroneal palsy E. |
B
|
|
|
Severe pre-eclampsia. WORST treatment option:
A. Magnesium B. Nifedipine C. Metoprolol D. SNP E. |
D
|
|
|
In pregnancy the dural sac ends at:
A. T12 B. L2 C. L4 D. S2 E. S4 |
D
BJA 1995 75: 6-8 Anatomical configuration of the spinal column in the supine position. Confirms in both pregnant and non pregnant it ends at S2 |
|
|
Septic elderly man. Given lots of obs but essentially mixed venous oxygen sat 65%, lactate 4, MAP low. Mx.
A transfuse B fluid bolus C Noradrenaline |
B |
|
|
Another pregnant woman with ?MS. Develops SVT. Try vagal manouveres without success.
A. Adenosine B. ? C. ? |
A
|
|
|
Pregnant woman presents with narrow complex tachycardia HR 190, stable BP 100/60. No response to vagal manoevures. Management?
A. Adenosine 6mg B. DCR C. Amiodarone D. Atenolol E. ? |
A
|
|
|
Which gives the BEST seal?
A LMA classic B Proseal C Intubating LMA D. ? E. ? |
B |
|
|
The MAIN indication for biventricular pacing is
A. complete heart block B. congestive cardiac failure C. VF D. E. |
B |
|
|
What's the area burnt in the following man? Half of left upper arm, all of left leg and anterior abdomen.
A. 27% B. 32% C. 42% D. |
A
|
|
|
The intercostobrachial nerve:
A. Arises from T2 trunk B. Is usually blocked in brachial plexus block C. Supplies antecubital fossa D. can be damaged by torniquet E. Arises from inferior trunk |
D
|
|
|
IV paracetamol:
A. late plasma levels around the same as oral B. highly protein bound C. ?30%? renally excreted D. VD 10L/kg E. |
A
True. “plasma concentrations of intravenous propacetamol were significantly higher and obtained earlier, compared to oral administration, however after the first hour and up to 24 hours the plasma concentrations remained similar” MIMS False. It is not extensively protein bound. False. 90% excreted in 24 hours. False. VD 1L/kg |
|
|
Patient with diastolic dysfunction. Is it caused by:
A. Restrictive cardiomyopathy B. Dilated cardiomyopathy C. D. E. |
A
|
|
|
Management of rhabdomyolysis – best option?
A. Haemodialysis B. Bicarbonate C. Frusemide D. IV fluids E. |
D |
|
|
The average expected depth of insertion of an oral endotracheal tube, from the lip, in a normal newborn infant is
A. 7.5 cm B. 8.5 cm C. 9.5 cm D. 10.5 cm E. 11.5 cm |
C |