![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
127 Cards in this Set
- Front
- Back
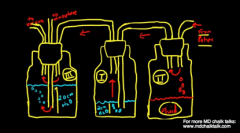
1. Given thefollowing diagram, what does X represent?
A. Amount of drainage since system was connected to patient B. Level of resistance to drainage of pleural cavity C. Level ofunderwater seal applied to pleural cavity D. Maximum pressure in pleural cavity on expiration E. Maximum suction that can beapplied to pleural cavity.
|
E. In this picture III is the suction control chamber I is the one way valve II is the collection chamber.
|
|
|
2. RH28Retrobulbar block. Sign of brainstem spread
A. Atonicpupil B.Unilateral blindness in blocked eye C. Contralateral blindness D. Diplopia-past papers remembered this as dysphagia E. Nystagmus (Question 2was a repeat but with different options) |
RPA say B - Loss of vision in contralateral eye Dsyphagia can also occur due to CN nerve palsy |
|
|
3. Something like: Otherwise healthy 20 yo male undergoes surgery for an ORIF tibia for open tib fracture. The limb is exanguinated and the tourniquet correctly applied at 250mmHg. His SBP is 120. When the surgeons go to start there is a small amount of bleeding. Do you.. A. Accept that a small amount of bleeding may occur with a tourniquet B. Reinflate at a higher pressure C. Check coags D. Take tourniquet down, rexanguinate and reinflate E. Something else |
RPA = D RNS and POW = A. CEACCP on tourniquet management. Intraoperative bleeding Common causes of intraoperative bleeding include incomplete exsanguination of the limb and a poorly fitting or under-pressurized cuff. Intraoperative bleeding may also be caused by blood entering through the intramedullary vessels of long bones.
|
|

4. What's this?
|
Wide mediastinum: Aortic dissection
|
|
|
5. Fatigue during night shifts can be minimized by: A. Avoiding daylight B. not sleeping during day C short naps during shift D use of caffeine or stimulants E. using benzodiazepines for sleep during the day |
C. Ref: ANZCA PS43 Many individuals find it difficult to reset their body time clocks to allow for effective daytime sleep after night duties. Daytime sleep is typically shorter and of inferior quality compared with sleep at night (13). Minimising the effects of night-time shift work may be achieved by taking a two hour afternoon sleep prior to the night duty, taking a 20-30 minute nap during the duty time, ensuring proper meals, and sleeping as soon as possible after the duty(14) |
|
|
6. [New] Patient with Acute Intermittent Porphyria presents to hospital with abdominal pain and requires a general anaesthetic. Which drug for PONV would you avoid?
A. Metoclopramide B. Prochlorperazine C. Tropisetron D. Ondansetron E. Droperidol |
A.
|
|
|
7. A 65 year old man having a total hip placement under general anaesthetic has continued to take his moclobemide. He becomes hypotensive shortly after induction. The best treatment would be judicious use of
A. adrenaline B. dobutamine C. ephedrine D. metaraminol E. phenylephrine F. noradrenaline |
E
Ref: OHA |
|
8. The following capnography trace was observed in an intubated and ventilated patient. The most likely explanation for this respiratory pattern is
A. endobronchial intubation B. endotracheal cuff leak C. gas sampling line leak D. obstructive airways disease E. spontaneous ventilatory effort |
?C
|
|
|
9. When topping up a labour ward epidural to an epidural for lower segment caesarean section, the optimum level of block when assessed for light touch is to:
A. T2 B. T4 C. T6 D. T8 E. T10 |
B.
|
|
|
10. You are in the pre-admission clinic assessing a 60 year old male who is due to undergo total knee replacement in 10 days time. He is taking Dabigatran 150mg BD for chronic atrial fibrillation. He has no other past medical history and normal renal function. He is planned for a spinal anaesthetic. The most appropriate management for his anticoagulation is:
A. Cease dabigatran 7 days prior B. Cease dabigatran 3 days prior C. Cease dabigatran 3 days prior and give bridging anticoagulation D. Cease dabigatran 24 hours prior and measure INR on day of surgery E. Continue dabigatran and withhold on day of surgery |
B
"The Central European Journal of Medicine - Dabigatran in patients with atrial fibrillation: perioperative and peri-interventional management. For Major procedures ie TKR A preoperative laboratory testing is usually not meaningful (Recommendation 3C). A dabigatran-sensitive coagulation test (Hemoclot test or ECT) may help to determine whether haemostasis is still impaired. Dabigatran should be paused the day before the intervention (Day – 1; Recommendation 1C). The therapy should be discontinued 2 days in case of creatinine clearance 50–80 ml/min or interventions associated with a high risk of bleeding. The therapy should be paused 3–4 days before the intervention if creatinine clearance is < 50 ml/min (Recommendation 1C)." |
|
|
11. A 15 yo girl with newly diagnosed mediastinal mass presents for supra-clavicular lymph node biopsy under GA. The most important investigation to perform pre-operativel
A. CXR B. CT chest C. MRI chest D. PET scan E. TOE |
POW = B > C RPA and RNS = B Can't find a reference, but need to assess trachea pre-induction |
|
|
12. A CTG recording with late prolonged decelerations. Cause:
A. GA B. Head compression C. Uteroplacental insufficiency D. Acute asphyxia E. Umbilical cord compression. |
RNS = ?D POW = C. (and E also possible) RPA = C (D and E also possible) Publishes cram mcqs = D |
|
|
13. A new antiemetic decreases the incidence of PONV by 33% compared with conventional treatment. 8% who receive the new treatment still experience PONV. The no of patients who must receive the new treatment instead of the conventional before 1 extra patient will benefit is |
D
NNT = 1/probability(with intervention) - probability(control) 8% with new treatment. Therefore 12% without. So NNT = 1/0.12-0.08 = 1/0.04 = 25 |
|
|
14. You are anaethetising a lady for elective laparoscopic cholecystectomy, who apparently had an anaphylactic reaction to rocuronium in her last anaesthetic. There has not been sufficient time for her to undergo cross-reactivity testing. What would be the most appropriate drug to use:
A. vecuronium B. cisatracurium C. pancuronium D. atracurium E. suxamethonium |
B |
|
|
15. Increase in period bleeding EXCEPT
A. Gingko B. Garlic C. Ginger D. Fish Oil E. Echinacea |
Answer: E
Garlic, ginger, ginko and ginseng: increase bleeding Fish oil: increases bleeding Echinachea: no change |
|
|
16. Post op hip ORIF, commonest periop complication |
C
|
|
|
17. You are anaesthetizing a 50 year old man who is undergoing liver resection for removal of metastatic carcinoid tumour. He has persistent intraoperative hypotension despite fluid resuscitation and intravenous octreotide 50 ug. The treatment most likely to be effective in correcting the hypotension is:
A. Adrenaline B. Dobutamine C. Levosimenden D. Milrinone E. Vasopressin |
E
|
|
|
18. 80 year old female for open reduction and internal fixation of a fractured neck of femur. Fit and well. You notice a systolic murmur on examination. Blood pressure normal. On transthoracic echo, she has a calcified aortic valve, with aortic stenosis with a mean gradient of 40mmHg. How do you manage her:
A. Instigate low dose beta blockade B. Defer, and refer to a cardiologist C. Perform a transoesophageal echo to get a better look at the valve D. Proceed to surgery with no further investigation E. Perform a dobutamine stress echo |
D |
|
|
19 (Repeat) Electrocardiogram in the Cs5 configuration. What are you looking at when monitoring lead I.
A. anterior ischaemia B. atrial C. inferior D. lateral E. septal |
A
For Cs5: RA placed under R clavicle, LA placed at V5, LL placed as normal Lead ONE is for anterior ischaemia, lead TWO is for inferior / arrhythmia detection |
|
|
20. (Repeat) Pringles procedure for life threatening liver haemorrhage includes clamping of: A. Aorta B. Hepatic artery C. Hepatic vein D. Portal pedicle E. Splenic Artery |
POW and RNS = D RPA = B (portal vein and hepatic artery) It is the hepatic pedicle not the portal pedicle
BJA 2004. 93 (2): 204. Effects of Pringle manoeuvre and ischaemic preconditioning on haemodynamic stability in patients undergoing elective hepatectomy: a randomized trial “During hepatic resection, the risk of severe intraoperative bleeding represents a major risk. To avoid massive blood loss, continuous or intermittent vascular clamping of the hepatic artery and portal vein (‘Pringle manoeuvre’) is an efficient method to reduce haemorrhage.” Portal pedicle contains Hep Artery and Portal vein therefore D is correct. Also referred to as portal triad, which is Hep a., Portal v. and bile duct. |
|
|
21. A 60 y.o. diabetic man has below knee amputation for ischaemic leg. His neuropathic pain is treated with oxycodone 40mg BD and paracetamol 1g QID. He is also on omeprazole 20mg BD for reflux. You decide to start him on gabapentin. Before choosing a dosing regime and starting treatment it is most important that you: |
C
Renal excretion - must dose reduce. Gabapentin is renally excreted unchanged. In overdose it can be removed by dialysis |
|
|
22. The anterior and posterior borders of the 'triangle of safety', the preferred insertion site for an intercostal catheter, are pec major and:
A. Coracobrachialis B. Deltiod C. Lat Dorsi D. Serratius Anterior E. Trapezius |
C |
|
|
23. A 39 yo male brought into ED with a compound fracture of his forearm. Has a history of schizophrenia and depression with uncertain medication compliance. He is confused and agitated with generalised rigidity but no hyperreflexia. Obs - HR 120, BP 160/90, RR 18, Sats 98 Temp 38.8 Likely Dx? A. Heat stress from anticholinergics B. Hypoxic ischaemic encephalopathy C. NMS D. Serotonin syndrome E. Pain from fracture |
C Serotonin sydnrome causes hyperreflexia From DSM-IV Severe muscle rigidity and hyperthermia associated with the use of antipsychotic medication Two or more of the following: diaphoresis, HT, tachycardia, incontinence, dysphagia, mutism, tremor, confusion or altered GCS, leukocytosis, elevated CK. |
|
|
24. CO2 (laser??) penetrates surface tissue so well with little damage to underlying tissue because:
A. Well absorbed by Hb B. Poorly absorbed by H20 C. Widely disseminated in tissue D. Long infrared wavelength E. Short infrared wavelength |
RNS = D POW D > A
|
|
|
25. (NEW) An 80yo man is having a transuretheral bladder resection, the surgeon is using diathermy close to the lateral bladder wall which results in patient thigh adduction. The nerve involved is:
A. Inferior gluteal B. Obturator C. Pudendal D. Scaitic E. Superior gluteal |
B
|
|
|
26. (New) You are involved in research and as part of data collection you collect ASA scores. This type of data is:
A. Categorical B. Nominal C. Non-parametric D. Numerical E. Ordinal |
E |
|
|
27. An otherwise healthy man presents with anaemia. The test that most reliably indicates iron deficiency is decreased
A. MCV B. serum ferritin C. serum iron D. serum transferrin E. total iron binding capacity |
B
|
|
|
28. 54 yearold radical prostatectomy with ongoing blood loss during the procedure. Surgeon complains of ooze and asks if the patient is on aspirin. Thromboelastograph shown below. Most appropriate therapy: A. rFVII B.cryoprecipitate C. FFP D. platelets E. tranexamic acid |
E. ?picture showed fibrinolysis? Life in the fast lane http://lifeinthefastlane.com/education/ccc/thromboelastogram-teg/ TEG AS A GUIDE TO TREATMENT Increased R time => FFP Decreased angle => cryopreciptate ( due to decreased rate of fibrin cross linking/etc. Decreased MA => platelets (consider DDAVP) Fibrinolysis => transexamic acid (or aprotinin or aminocaproic acid) |
|
|
30. The maximal allowable atmospheric concentration of nitrous oxide in Australian and New Zealand operating theatres (in parts per million) is
A. 5 B. 25 C. 50 D. 100 E. 200 |
B |
|
|
31. What is associated with down regulation of nicotinic acetylcholine receptors: |
B |
|
|
32.Rheumatoid arthritis. Most common C-spine abnormality is anterior subluxation.What is next most common direction of subluxation in RA A. lateral B. oblique C. posterior D. rotated E. vertical F. Subaxial |
E. CEACCP 2006 – anterior 80%, vertical 10-20%, posterior 5% Subaxial subluxation is uncommon and occurs below C2
|
|
|
33. MS patient requires GA. Most likely precipitant of deterioration: A. hyperthermia B.hypocarbia C.Non-depolarising muscle relaxant D. TIVA E. volatileanaesthetic agent Choice B mayhave been "decreased cardiac output" |
A. |
|
|
35. A reduction in DLCO can be caused by:
A. Asthma B. Emphysema C. Left to right shunt D. Pulmonary haemorrhage E. Bronchitis |
B |
|
|
36. A healthy 25 year old woman is 18 weeks pregnant. Her paternal uncle has had a confirmed episode of malignant hyperthermia. She has never had susceptibility testing. Her father and siblings have not been tested either. The best test to exclude malignant hyperthermia susceptibility before she delivers is
A. Genetic test father B. Genetic test woman C. Muscle biopsy sibling D. Muscle biopsy father E. Muscle biopsy woman |
RNS and RPA = D
From BMHA Not all patients can have a biopsy, these include children less than 10-12yrs (30kgs), pregnant women, and patients on prolonged steroid therapy. If the proband cannot be tested, eg a young child or deceased, then the nearest most appropriate relative is tested. In the case of a young child this would be the parents. |
|
|
37. (New) The size (in French gauge) of the largest suction catheter which can be passed through a size 8 endotracheal tube which will take up not greater than half the internal diameter is size:
A. 6 B. 8 C. 10 D. 12 E. 14 |
Answer: D
Endotracheal tube size refers to internal diameter in mm. French gauge requires a conversion: Fr 1 = 1/3 mm. Therefore Fr 3 = 1 mm So, Fr12 = 4 mm |
|
|
38. (Repeat) Pneumoperitoneum cases a decrease in cardiac output at what pressure (or possibly ABOVE what pressure) |
A
<10 mmHg: increased CO 10-20: decreased CO (unlikely to cause BP effects) >20: greatly decreased CO Miller says > 10. ref: CEACCP Laparoscopic abdominal surgery Initially, owing to autotransfusion of pooled blood from the splanchnic circulation, there is an increase in the circulating blood volume, resulting in an increase in venous return and cardiac output. However, further increases in the IAP result in the compression of the inferior vena cava, reduction in venous return and subsequent decrease in cardiac output. |
|
|
39. 60yo male had total knee replacement. 7 days post-operatively diagnosed with deep venous thrombosis on ultrasound. Was on LMWH. PLT dropped from 300 immediately post-op and now 150x10^9/L. All the following are acceptable treatments EXCEPT- |
RNS and RPA= E POW E or D Warfarin (Vit K antagonist) is contraindicated in acute HIT (or if suspected HIT), as it can cause skin necrosis or venous limb gangrene. |
|
|
40. [Repeat] Maximum dose (with low risk of toxicity) of lignocaine (with adrenaline 1:100000) for liposuction with tumescence technique:
A. 3 mg/kg B. 7 mg/kg C. 15 mg/kg D. 25 mg/kg E. 35 mg/kg |
E
"Tumescent technique for regional anesthesia permits lidocaine doses of 35 mg/kg for liposuction. JA Klein - Dermatol Surg, 1990" CEACCP: "Doses as high as 22–57 mg kg−1 of lidocaine7–9 have been used in the context of tumescent techniques and have been shown to have safe plasma concentration profiles. Addition of non-steroidal anti-inflammatory drugs and steroids has also been used to try to improve the quality and length of analgesia." |
|
|
41. 6 yearold 20kg anaesthetised and paralaysed for appendicectomy. First attempt- vocal cords seen. size 5.5 uncuffed. 2nd attempt with 4.5. Next appropriate step A.administer nebulised adrenaline B. attempt 4.0 tube C. examine trachea with fibreoptic bronchoscope D. LMA E. soften 4.5 tube and attempt reinsertion |
RPA = C RNS = B KSMC POW = D or E Would depend on wording. Child is appropriate wt for age so 5.5 should fit. If not then 5. Very strange that a 4.5 would be too big… do they mean a leak on a 4.5? or laryngospasm? In any event need to not waste time and risk aspiration
|
|
|
43. Drug to facilitate clip placement during cerebral aneurysm surgery;
A. nimodipine B. mannitol C. adenosine D. hypertonic saline E. thiopentone |
C
|
|
|
44. Which drug should be avoided both intra- and post operatively in a woman having surgery who is breast feeding a 6 week old baby? A. codeine B. morphine C. paracetamol D. parecoxib E. tramadol ??F. pethidine |
RPA = A or F POW = A RNS = A -can cause deaths. Pethidine not included in some remembered sets of options.
From Acute Pain Management Scientific Evidence 2010: A. There has been a death in a child of a rapid metaboliser, and other babies have shown decreased alertness, poor feeding, and lethargy B. Morphine: Safe (The recommended opiod for use in breastfeeding mothers) C. Paracetamol: Safe D. Parecoxib MIMS says avoid. Celecoxib and most other NSAIDs: Safe (Ibuprofen safest) E. Tramadol is concentrated in breast milk, but appears to be safe F. (If this was even an option): Infants are detectably more drowsy, and norpethidine excretion in neonates is slow. Pethidine is not recommended. Aspirin: Unsafe Indomethacin: Associated with maternal psychosis in the post-natal period. Fentanyl, Midaz, propofol: so safe that mothers probably don't need to discard breast milk after a GA. |
|
|
45. A three year old girl for an elective hernia repair is seen immediately prior to surgery. It is revealed she had 100mL of apple juice 2 hours ago. The best course of action is to:
A. Postpone surgery for 2 hours B. Postpone surgery for 4 hours C. Postpone surgery for 6 hours D. Cancel surgery E. Continue with surgery |
E
From ANZCA PS15 Healthy adults * solids 6 hours * clear fluids <200mL up to 2 hours Healthy children > 6/52 for elective * Solid food and formula up to 6 hours * Breast milk up to 4 hours * Clear fluids up to 2 hours Healthy infants <6/52 for elective * Formula and breast milk up to 4 hours * Clear fluids up to 2 hours Consider PPI for patients with GORD |
|
|
46. In accordance with their belief that blood transfusion is wrong, a Jehovah's Witness may consent to all of the following except: A. Cryoprecipitate B. Immunoglubulins C. Fresh Frozen Plasma D. Factor VIIa E. Prothrombinex |
RPA + POW = C RNS = D only synthetic If question was all except..
Blue Book 2011: Acceptable: cryo, Hb, Ig, Albumin, clotting factors, EPO, interferon. |
|
|
47. 80 year old lady with fractured NOF needing ORIF. On examination had a systolic murmur. Arranged TTE which showed a calcific aortic valve with peak velocity of 4 m/s. Using the simplified Bernoulli equation, what is the peak pressure gradient across the valve:
A. 16 mmHg B. 32 mmHg C. 48 mmHg D. 64 mmHg E. 80 mmHg |
D
P1-P2 = 4V^2 4 * 16 = 64 mmHg |
|
|
48. You have developed a new cardiac output monitor called WaCCO. You want to compare the readings with the gold standard, a pulmonary artery catheter. What is the best statistical method to present the data/results:
A. Funnel plot B. Bland-Altman plot C. Forest plot D. Galbraith plot E. Partial regression plot |
B
|
|
|
49. 40 yearold, pulmonary artery hypertension 80/60 pre-op. Lap cholecystectomy. SuddenSPO2 87, sBP 80/40, etPCO2 45. Cause? A. gasemboli B. Leftheart failure C.myocardial ischaemia D.pneumothorax E. right heart failure |
E. PaCO2 would be in the 50 or more, so that will put the PA pressures up and strain the right heart. Would expect low rather than high ETCO2 with air embolus. |
|
|
50. A 60 year old, triple vessel disease normal LV Post CABG hypotensivem ST elevation II, avF, CVP 15 PCWP 25. Normal SVR. Echo shows:
A. A early diastolic mitral inflow dynamic with atrial systole B. Left inferior hypokinesis C. Left ventricle collapse in systole D. Right ventricle dilation and TR E. Severe Mitral Regurg |
B
|
|
|
51. Maximum amplitude from TEG or ROTEM decreased give |
C
|
|
|
52. Young male, previous IVDU, now on 100mg Methadone per day has a laparotomy with an effective epidural. Amount of IV Morphine needed per HOUR: A. 1mg B. 2mg C. 4mg D. 8mg E. 16mg |
RPA and RNS= C POW, Marc = B
Med Calc: 100mg methadone = 300 mg morphine oral = 100m morphine IV 100/24 = 4.1mg/hr But for safety usually decrease dose by 50% due to incomplete cross tolerance therefore 2mg |
|
|
53. A healthy 25 year old woman is 18 weeks pregnant. Her paternal uncle has had a confirmed episode of malignant hyperthermia. She has never had susceptibility testing. Her father and siblings have not been tested either. The best test to exclude malignant hyperthermia susceptibility before she delivers is A. Genetic test father B. Genetic test woman C. Muscle biopsy sibling D. Muscle biopsy father E. Muscle biopsy woman |
D |
|
|
54. Fluoroscopy in the operating theatre increases the exposure of theatre personnel to ionising radiation. Best method to minimise one's exposure to such radiation is to A. have dosimeter checked at least 6-monthly B. limit exposure time to radiation C. maximal distance from radiation source D. stand behind transmitter of C arm E. wear protective garments |
RNS and RPA = C POW E>B
Bernies notes - STG boys think E, Im not convinced… hard to go past B
Published cram cards say C
Because the intensity of scattered radiation is inversely proportional to the square of the distance from the source, the best protection is physical separation. A distance of at least 3 feet from the patient is recommended. Six feet of air provides protection the equivalent of 9 inches of concrete or 2.5 mm of lead. |
|
|
55. 10L/min via facemask. Cylinder C 15 000kP lasts A. 10min B. 15min C. 30min D. 45min E. 60 min |
D True Size C cylinder contains 400-490L |
|
|
56. 23 year old. TCA . A. adrenaline B. amiodarone C. lignocaine D. magnesium E. phenytoin |
C - can be used in VT Avoid amiodarone Phenytoin - true for seizures (after you give benzo to terminate seizures) |
|
|
57. Ibuprofen dose for one year old child tds regular post-op dose |
B
MIMS 5-10mg/kg Q6-8H |
|
|
58. AICD, what does a magnet do A. Maintain defib activity & activate asynchronous pacing B. maintain anti tachycardia pacing & deactivate asynchronous pacing C. Deactivate anti tachycardia pacing & activate asynchronous pacing D. Deactivate defib & activate asynchronous pacing E. Deactivate defib & deactivate asynchronous pacing |
?E seems the closest
RPA answers say - Antitachycardia detection is suspecnded and PACING is unaffected.
"With the ICD, approximately 99% of them are programmed to have their anti-tachycardia function disabled in the presence of a magnet without affecting their bradycardia pacing." |
|
|
59. ?To prevent transmission of CJD? Airway-contaminated equipment A. autoclave B. protected plastic covers C. sterilise in ethylene oxide D. 134degreesC for 3 min E. thrown away |
RPA = D directly from health document! Instruments should not be allowed to dry, and should be kept separate from all other instruments for cleaning and for use. Airway equipment (saliva) is low infectivity as compared to CNS material.
POW and RNS = E |
|
|
60. A 35yo man collapses in shopping mall and is resuscitated by bystanders using an AED. On admission to hospital his ECG was as below;
ECG - sinus, rate ~60, normal axis, borderline PR interval, RSR' in V1 and V2 with ST elevation and inverted T waves (Brugada sign) A. Acute pericarditis B. Brugada C. Cocaine intoxication D. Coronary artery spasm E. Long QT syndrome |
B
Incomplete RBBB, ST elevation V1-V3. T-wave inversion. Positive family history. More common in SE Asians. |
|
|
61. A 58yo with solitary hepatic metastasis from colon cancer scheduled for resection of R lobe of liver. Inorder to manage the risk of intra-operative haemorrhage, it is most important to maintain:
A. High CVP in anticipation of heavy blood loss B. Decreased MAP to reduce arterial bleeding C. Decreased CVP to reduce venous bleeding D. Normal MAP in anticipation of heavy blood loss E. Normal CVP to ensure adequate filling of the heart. |
C |
|
|
63. A man is admitted to ICU with a Sodium of 105 mmol/L. What is the maximum his sodium should be raised in the next 24 hours A. 5 mmol B. 10 mmol C. 15 mmol D. 20 mmol E. 25 mmol |
Cram = B POW = B RPA = A RNS = B
OHA: Says <12mmol in 24 hours.
Because a 4 to 6 meq/L increase in serum sodium concentration appears to be sufficient to reverse the most severe manifestations of acute hyponatremia and because actual correction often exceeds what is intended, an increase of 4 to 6 meq/L in 24 hours is a reasonable therapeutic goal for all patients. Every effort should be made so that the increase in serum sodium is less than 9 meq/L in any 24-hour period.
For patients with severe symptoms, the first day's goal may be achieved in the first few hours since the daily rate rather than the hourly rate of correction is associated with osmotic demyelination. |
|
|
64. What is the distance from lips to carina in a 70 Kg man?
A. 21 cm B. 23 cm C. 25 cm D. 27 cm E. 29cm |
RPA = C POW = C>D Cram =D RNS = D
There are other answers going around that reference an Indian paper. These are wrong - the Indian paper was done to demonstrate the difference between the caucasian values given in Miller, and the general Indian population. |
|
|
65. The action of which laryngeal muscle opens the cords? A. Cricothyroid B. Posterior cricoarytenoid C. Lateral Cricoarytenoid D. Thyroarytenoid E. Vocalis |
B
Lee's synopsis:
Posterior cricoarytenoids: open glottis Lateral cricoarytenoids: close glottis Interarytenoid: close glottis Cricothyroid: tense cords Thyroarytenoid: Relax cords Vocales: relax cords |
|
|
66. Induction of a 4yr old child with Arthrogrophysis multiplex congenita, however you find it difficult to place the laryngoscope. What is the concern? (paraphrased question here, can’t remember all possible answers)
A. MH B. Neuroleptic malignant syndrome C. ? D. opioid induced rigidity E. TMJ rigidity |
E |
|
|
70. A patient is suffering from aortic dissection with acute aortic regurgitation. BP 160/90, HR 100 & evidence of acute pulmonary oedema. What is your immediate management? A. Beta-blockers B. Dopamine C. Dobutamine D. Sodium nitroprusside E. Intra-aortic Balloon Pump |
RPA = A POW = A>D RNS = A (D as second line)
A because Ceaccp Aortic dissection: esmolol, metoprolol, labetalol, SNP, GTN or hydralazine. Beta blockers before vasodilators as reflex catecholamine release secondary to vasodilation may increase LV contraction
D because of the APO and AR. If there was no AVR and APO then A would be a better answer. The primary goal is to reduce the force of left ventricular con- traction without compromising perfusion, thus reducing shear forces and preventing further extension of the dissection or poss- ible rupture. Beta-blockers (e.g. esmolol, metoprolol) and labetalol (beta- and alpha-blocker) can be used. If further reduction in BP is required, sodium nitroprusside, glyceryl trinitrate, or hydralazine are appropriate. Beta-blockers should be given first before vasodi- lators, as the reflex catecholamine release due to vasodilatation may increase left ventricular contractions. |
|
|
71. Presented are a femoral arterial line trace & a central venous line (JVP) trace - looked like it was demonstrating elevated right atrial pressures... What is demonstrated by these pressure waveforms? A. Aortic Stenosis B. Aortic Regurgitation C. Pulmonary Regurgitation D. Tricuspid Regurgitation E. Mitral Regurgitation
71. Given the following femoral AL and CVP traces, what is the most likely cause? [diagram] A. Pulmonary stenosis B. Left Ventricular Failure C. Tricuspid Regurgitation D. Aortic Stenosis E. Mitral Stenosis
71. Trace of an Arterial line and RA venous pressure. The venous pressure started escalating prior to the onset of the arterial pressure rise (all 4 regurg options, one stenotic option) |
Who knows, but probably tricuscpid regurg? POW = C or D RPA and RNS = no answer |
|
|
72. The MELD score is calculated using INR, Bilirubin & what?
A. Creatinine B. Albumin C. Urea D. AST E. Ammonia |
A
INR, bilirubin and creatinine |
|
|
73. In resuscitating a newborn infant after delivery, the time at which you would like to achieve arterial oxygen saturation of 85-90%: A. 2mins B. 3mins C. 4mins D. 5mins E. 10mins
73. Aim for saO2 of 85-90% in neonatal resuscitation by- A. 1min B. 2min C. 3min D. 5min E. 10min |
E
ARC guidelines: 10 mins
Measured off R arm because of PDA |
|
|
74. (repeat): You inserted a central venous line and peripheral arterial line for a patient who is having a tumour removed via craniotomy. The transducers of both the lines were placed at the level of the right atrium 13cm below the level of the external auditory canal. MAP is 80mmHg, CVP 5mmHg. What is the CPP? A. 62mmHg B. 65mmHg C. 70mmHg D. 75mmHg E. 80mmHg |
RPA, RNS = C POW = B if the skull is open both CVP and ICP = 0 at the level of the brain, all neuro bosses agree |
|
|
75. What proportion of the population are heterozygous for plasma cholinesterase deficiency?Having a Dibucaine number of 30-80. |
C
Peck & Hill p183 |
|
|
76. You are putting in a internal jugular central venous line. Which maneuvre causes maximal distension of the internal jugular vein? |
E
Valsalva - probably gives maximal distention |
|
|
82. A 40 yo woman for laparotomy to remove phaeochromocytoma under combined epidural and general anaesthesia. Pre-operatively treated with phenoxybenzamine and metoprolol. Intra-operatively, blood pressure is 250/130 despite high dose phentolamine and SNP. HR is 70/min and SaO2 are 98%. The next most appropriate treatment is: |
RPA = D>E RNS E (because D is slow onset) POW = D > E Cram = D
CEACCP: Adequate pre-operative care aims to limit the severity of these episodes but vasodilators must be prepared and close at hand. Such agents include boluses of phentolamine 1–5 mg and labetalol 5–10 mg or sodium nitroprus- side, GTN and nicardipine infusions. Sodium nitroprusside has a rapid onset and offset of action; it is not associated with toxicity when used in recommended doses. Nicardipine is a calcium chan- nel blocker which has been used as an infusion for fast titration of blood pressure. The use of isoflurane as an antihypertensive agent is a practical alternative. Magnesium sulphate infusions have recently been described (inhibits catecholamine release, exerts a direct vasodilator effect and reduces α-receptor sensitivity). |
|
|
83. Best option to reduce risk of Ventilator induced pneumonia? A. Nurse in supine position B. Early spontaneous ventilation through ETT C. Oral hygiene D. Use antacids E. Regularly change breathing circle |
POW = B or C RNS = C RPA = C Minimise tine ventilated, reduce airways colonisation (by aspiration of gastric contents, nurse semi rec, maintain ett cuff pressure, oral care wit chorhex), hand hygiene |
|
|
85. 37 female presents to ED with headache and confusion. She is otherwise neurological normal and haemodynamically stable. Urine catheter and bloods takes. UO > 400ml/hr for 2 consecutive hours, Serum Na 123 mmol/l, Serum Osmolality 268, Urine Osmolality 85 The most likely diagnosis is A. Central diabetes insipidus B. Nephrogenic diabetes insipidus C. Psychogenic polydipsia D. Cerebral salt wasting E. SIADH |
C
Hyponatraemic |
|
|
89. A 63 year old woman with chronic AF has a history of HTN, T2DM and has had a previous CVA. Her annual risk of stroke without anticoagulation is A. <1% B. 1.9% C. 2.8% D. 4% E. 8.5% |
E |
|
|
90. An 85y.o for an open AAA repair. Refuses blood because of risk vCJD. You tell him you won't anaesthetise him as the risk is too high. This is an example of A. Autonomy B. Beneficence C. Justice D. Coercion E. Paternalism |
RPA, RNSH = E POW = A |
|
|
91. The American Heart Association (AHA) guidelines for preoperative cardiac risk assessment define a poor functional capacity as only able to exercise at a level of less than 4 metabolic equivalents (METs). Exercise capacity of 4 METs corresponds to |
RPA and RNS = A POW = D A = 1-4 METS D = 4-10 METS |
|
|
92. Pneumoperitoneum for laparoscopy is commonly associated with each of the following EXCEPT |
C
Miller table
A - Up B - Up C - Correct - decreases D - Up E - Up |
|
|
93. 7 year old with closed head injury. Intubated and ventilated in ICU. Serum sodium 142. Most appropriate maintenance fluid is: |
C
(Because head injury -> want isotonic solution) |
|
|
94. Patient with Marfan's syndrome. Thoracoabdominal aortic aneurysm repair. 24 hours later in ICU noted to be blood in CSF drain and patient obtunded. Most appropriate urgent management: |
A |
|
|
99. (new) The respiratory pattern most likely seen in an acute C5 spinal cord injury: A. increased respiratory rate B. arterial hypoxaemia C. chest wall immobility D. ? E. ? |
RPA, POW, RNS = A |
|
|
100. (new) Afterload reduction is most useful in which of the following: A. aortic stenosis |
RPA = E POW = E > D RNS = ? MS would benefit most as aortic root pressure already reduced in AR AS - worse Tetralogy of fallot - reduced afterload increases R => L shunt AR + MR - benefit Tamponade - benefit |
|
|
101. A 20 year old man was punched in the throat 3 hours ago at a party. He is now complaining of severe pain, difficulty swallowing, has a hoarse voice and had has some haemoptysis. What is your next step in his management? A. Awake Fibreoptic Intubation B. CT scan for laryngeal fractures C. Direct laryngoscopy after topicalising with local anaesthetic D. Nasopharyngoscopy by an ENT surgeon E. Soft tissue xray of the neck |
RPA = D or E RNS, POW and Cram = D Marc
Blue book 2005 CXR+Neck then nasoendoscopy then CT larynx |
|
|
102. Preferred method for treating raised INR A. FFP B. FFP + prothrombinex C. FFP + vitamin K D. prothrombinex E. prothrombinex + vitamin K |
RPA, RNS =E
Prothrombinex + vit K for all Add FFP if life-threatening severe bleeding |
|
|
103. Regarding PS31, Level II check includes: |
Service Label High pressure system - O2 cylinder, pipeline supply Low pressure system - rotatmeters, vaporizers Leak Test CO2 absorbtion Ventilator Scavenging Emergency ventilation
Level three: Changed circuit Changed vaporizer IV anaesthetic devices Intubation / LMA gear Suction Gas analysis Monitoring and alarms Humidifiers Filters
|
|
|
104. Anaphylaxis, when to check tryptase A. Within 15 minutes of event B. Between 1 hour and 3 hour C. Between 4 hour and 6 hour D. Between 6 hour and 12 hour E. After 24 hour |
B |
|
|
107. [New] A 53 yo man with severe Parkinson’s Disease is scheduled for L) Total shoulder arthroplasty. He has a Deep Brain Stimulator (DBS) in situ which is functioning normally. On the day of surgery, optimal management is to: A. ensure placement of the diathermy return pad to direct current spread away from the DBS B. leave the DBS as it can safely be left activated throughout surgery. C. turn off the DBS and cover with oral levodopa D. turn off the DBS for the duration of surgery but reactivate prior to emergence from anaesthesia. E. use bipolar diathermy as it’s the only safe option
|
POW = A and D RNS = E RPA = C
From Bernies notes: CEACCP Themanufacturers of the DBS state that diathermy is contraindicated in patientswith a DBS in situ. This is unfortunately misleading asthey are referring to shortwave diathermy, microwave diathermy, and therapeuticultrasound diathermy, which are used by a number of physical therapists for thetreatment of joint and muscle complaints. These modalities induce heating atthe tissue–electrode interface leading to potential tissue damage.Surgicaldiathermy (electrocautery) can damage the DBS leads and can also causetemporary suppression of the neurostimulator, reprogramming of theneurostimulator, or both, but is not contraindicated. When diathermy is necessary, the following precautions shouldbefollowed: (i) use bipolar diathermy wherepossible; (ii)if unipolar diathermy is necessary: (a) use only a low-voltage mode; (b) use the lowest possible powersetting; (c) keep the current path (groundplate) as far from the neurostimulatorand leads as possible (usuallylocated in thesubclavicular space with the leadsrunning up the neck, posterior to the ear, to the crown ofthe head). After using diathermy, confirm that the neurostimulator is functioning as intended.
Emedicine Potential problems include thermal injury to brain tissue, reprogramming, and damage of the device and its leads. Manufacturer recommendation and literature review[56,59,93] encourages preoperative pulse generator adjustment and postoperative interrogation. If the patient can tolerate the tremor and it does not interfere with surgery, thepulse generator can be safely turned off before the operation. Bipolar electrocautery may reduce the potential for electromagnetic interference. If amonopolar device is necessary, haemostasis can be obtained with the aid of a battery-operated heat-generating handheld electrocautery device or with the useof a dispersive plate to direct the current away from the pulse generator andlead system. Surgeons should be reminded to use the lowest diathermy energy possible in short irregular bursts.
|
|
|
108. (New) A postpartum woman presents with numbness over posterior thigh, lateral leg and foot. There is weakness on flexion of the knee. An epidural was sited for labour and she underwent an instrumental delivery. The most likely site of the injury is A. Femoral neve B. Lateral femoral cutaneous nerve. C. Lumbosacral plexus D. Obturator nerve E. Sciatic nerve
|
RNS, RPA = C POW = B and E
|
|
|
109 - something like this one: 41. A patient with known metastatic lung cancer is found to have hypercalcaemia, all of the following would help excretion of calcium except |
Answer: A |
|
|
110. (New, long stem taking up half the page) Male in 60's one day post laparotomy. Management includes: IVH @40ml/hr, 2L oxygen via nasal prongs, and a morphine PCA. Observations: t38.8C, RR14, Sats 88% Examination: mildly sedated, bibasal creps. In addition to increasing the FiO2 what would be your initial management? A. Incentive spirometry B. Diuresis C. Broad spectrum ABs D. Naloxone 100mcg increments E. ? |
POW, RNS, RPA = A |
|
|
111. A patient is coming for an operation on his upper limb. 5mls of 0.75% ropivacaine is placed around the structure seen below. What is the most likely consequence of this?
Picture was of probe on posterior upper arm |
??radial nerve block
B |
|
|
112. A 40 year old man suffered a traumatic brain injury 2 days ago. He does not meet the criteria to be certified brain dead. What investigation will be most useful to assess cerbral function prior to organ donation. |
A To exclude status |
|
|
113. Isoflurane is administered in a hyperbaric chamber at 3 atmospheres using a variable bypass vapouriser, at a constant fresh gas flow and vapour dial setting, the vapour produced will be: |
D |
|
|
114. What is most likely to occur if the earth/grounding plate that is attached to a patient for use with monopolar diathermy malfunctions? |
C |
|
|
115. A 24yo primigravida, 25/40 gestation, BP 150/90 on 4 occasions. No signs of pre-eclampsia. Which antihypertensive is inappropriate? |
C |
|
|
116. Post-spinal surgery, patient notices paraesthesia of R arm, surgeon thinks this is an ulnar nerve palsy due to poor positioning. What sign will distinguish a C8-T1 nerve root lesion from ulnar nerve neuropathy? A. paraesthesia in little finger B. paraesthesia in the distribution of the interscalene nerve C. weakness in adductor digiti minimi D. weakness in the abductor pollicis brevis E. weakness in lateral interosseus |
D Median nerve supplies LOAF Hint: "brevis" sounds like "bread" hence "LOAF".
Lumbricalsx2 Opponens pollicis Abductor pollicis brevis Flexorpollicis brevis
|
|
|
119. According to PS09, the minimum requirement for administering propofol for conscious sedation is |
A |
|
|
122. Reasons infants desaturate faster than adults on induction (?did it say rapid sequence?) |
C |
|
|
125. Adenosine can be used to treat |
RPA = C POW = B RNS = say adenosine is diagnostic in A and B and that it can be used for SVT in WPW Cram - D Kerry = C (IF the person has SVT which is not stated) otherwise i would be inclined to go for B. |
|
|
126. Induction with thio 5mg/kg, scoline 2mg/kg, Difficult to open mouth, Finally intubated. Next step |
RPA = B POW, RNS = A Cram = A
OHA:
Switch to MH safe anaesthetic Wait 15 mins and monitor for increasing heart rate / CO2 |
|
|
127. In a patient with an intra-orbital haemorrhage, following local anaesthetic injection, the adequacy of ocular perfusion is best assessed by A. angiography B. direct ophthalmoscopy C. indirect ophthalmoscopy D. intra-ocular pressure tonometry E. palpation of the globe by an experienced clinician |

POW, RNSH, Marc = C RPA = B -- says the opthal. Anaesthetist at the Melbourne course
Royal college of anaesthetists and opthalmologists consensus document |
|
|
128. A patient is in Class IV Haemorrhagic Shock, secondary to a gunshot wound to the abdomen. He is clinically coagulopathic 30 minutes later. He has received intravenous Hartmann's 1L. The coagulopathy is likely related to: |
E
Causes of coagulopathy: Tissue injury / hypoperfusion Consumption of clotting factors Acidosis Hypothermia Dilution of clotting factors Hyperfibrinolysis |
|
|
129. (Repeat) A 20 kilogram child suffered 15% full thickness burns 6 hours ago. Optimum crystalloid resuscitation for the first hour is: |
C
4 * 20 * 15 = 1200 mL So 600mL first 8 hours, 600mL next 16 So 300mL/h for next 2 hours, then 600/16.
40+20 = 60mL/h maintenance.
4ml/kg * BSA burns over 24/hours, with 1/2 in the first 8 hours and the rest over the next 16, plus maintenance. |
|
|
130. You’re anaesthetizing an otherwise well 40 yo male for a craniotomy. Propofol and remifentanil TIVA. Using entropy. The MAP is 70 mmHg, heart rate is 70 bpm, Sats are 98%, state entropy is 50 and the response entropy 70. Most appropriate next step is A. give 0.5 mg metaraminol iv B. use NMT to assess train of four ratio C. change to volatile anaesthetic D. do nothing E. increase propofol TCI concentration by 0.5 |
B
Patient is likely not paralysed. B seems appropriate. Other options: increase analgesia.
BiS: bispectral index: analyses EEG
Entropy: Sate entropy: 0.8-32Hz (primarily EEG) Response entropy: 0.8-47Hz (Includes EMG dominant frequencies)
RE - SE difference indicates upper facial EMG activation in response to an external stimulus. Usually pain. Requires a non-paralysed patient.
Elevations in RE are generally followed by elevations in SE.
From CEACCP article: "During anaesthesia, state entropy and response entropy normally have the same value, but if response entropy diverges by more than 10 points from the state entropy value the ‘analgesic’ component of the anaesthetic may be inadequate."
Roger Traill agrees |
|
|
131. The normal physiological response following ECT is |
B
From CEACCP: |
|
|
132 (repeat) ->also recalled as Q148 so one must be a mistake –see below Aspirin Overdose. What will enhance her elimination most effectively? |
Cram, RNS, RPA =B POW = B or E
From Oh's |
|
|
133. A 50 year old male is having an aortic valve replacement for aortic stenosis. He is stable on bypass initially but after the first dose of cardioplegia his MAP falls to 25mmHg, CVP 1 and his mixed venous oxygen saturation is 80%. What is the best management in this situation. A. Metaraminol bolus B. Commence an adrenaline infusion C. Increase oxygen flow rate D. Increase pump flow rate E. IV crystalloid bolus |
POW = A Marc, Michael p RNS = D RPA = D and ?A Cram D
|
|
|
134. An eighty year old man presents to the emergency department with two hours of severe abdominal pain. On examination he has a tender pulsatile 8cm mass. His GCS is 12, heart rate 104, blood pressure 80/49, Temp 35 degrees, SpO2 92%, respiratory rate is 30/min. What is the next appropriate step. |
B
Likely leaking AAA Needs emergency laparotomy PPV may worsen venous return and BP Increasing BP may result in more bleeding Ideally do as little as possible until in OT
|
|
|
137. A PiCCO monitor may be used to measure cardiac output through use of: |
C
Swan-Ganz pulmonary artery catheter (PAC) - gold standard, but also most invasive. Uses thermodilution |
|
|
138. A tablet containing OxyContin 40mg and naloxone 20mg offers the following advantage over OxyContin alone. |
POW = A > B Cram, RNS, RPA = B
MIMS: "The naloxone component in a fixed combination with oxycodone is indicated for the therapy and/or prophylaxis of opiod induced constipation." |
|
|
141. Immunity to Hepatitis B is demonstrated by the presence of |
C
http://www.cdc.gov/hepatitis/hbv/pdfs/serologicchartv8.pdf |
|
|
142. In an adult with advanced liver cirrhosis, the best predictor of bleeding is |
E |
|
|
143. 65 year old lady with acute cholecystitis presenting for cholecystectomy. Has known hyperparathyroidism. Calcium 2.2mmol/L (normal values given). Initial treatment with: |
Answer: C |
|
|
144. SG67 20 year old male 80kg presents post house fire with 30% burns. Using the Parkland formula how much fluid should he have replaced in the first 8 hours. |
E
4 * 80 * 30 = 9600 over 24 hours. 4.8L CSL in first 8 hours. |
|
|
145 The thoracic paravertebral space is continuous down to |
B |
|
|
146. To best visualise a superficial peripheral nerve you should use a |
B
USRA http://www.usra.ca/transducer.php
For superficial structures (e.g. nerves in the interscalene, supraclavicular and axillary regions), it is ideal to use high frequency transducers greater than or equal to 7 MHz. Transducers in the range of 10-15 MHz are preferred but depth of penetration is often limited to 2-3 cm below the skin surface. |
|
|
149 You have administered a regional anaesthetic to a primiparous woman for an emergency caesarean section. Soon after delivery of the baby, the woman complains of chest pain and dyspnoea, then loses consciousness. What is the most likely cause of her loss of consciousness? |
POW C>D Cram, RNS, RPA =C
There are a few papers that mention AFE occuring within 30 minutes of delivery. |
|
|
150. The faster rate to desaturation observed in morbidly obese patients is due to: |
B |
|
|
[Nonum 1] In preadmission clinic with patient with a tracheostomy. To enable patient to talk you would- |
A
CEACCP management of tracheostomy:
If the tube is cuffed, the fenestration lies above the cuff. Deflation of the cuff during spontaneous respiration (with the fenestrated inner tube in place) allows air to pass caudally through the tracheostomy lumen and fenestration, as well as around the tracheostomy tube, and up through the larynx. This encourages maximal airflow through the upper airways during speech. A one-way speaking valve can also be used with the tracheostomy tube to maximize speech. This allows air to be entrained through the tube during inspiration. The valve then closes during expiration such that exhaled air must pass through the natural airway and vocal cords to exit the lungs, thus aiding phonation. |
|
|
[Nonum 2] Rheumatoid arthritis. Most common C-spine abnormality is anterior subluxation. What is next most common? A. Posterior B. Vertical C. Lateral D. Subaxial E. ? |
B
CEACCP http://ceaccp.oxfordjournals.org/content/6/6/235.full.pdf+html
Anterior 80% Vertical 10-20% Posterior 5% Lateral no number, presumably rare |
|
|
[Nonum 3] A 13kg child booked for elective procedure. Has had 100mL of clear fluid 2 hours ago. Management? A. Delay surgery for 2hours B. Delay surgery for 4hours C. Delay surgery for 6hours D. Proceed with surgery E. Cancel surgery |
D
PS15 |
|
|
[Nonum 4] Radical prostatectomy. Long operation and constant ooze. Surgeon asks if patient on 'aspirin'. You do a TEG. Shown TEG- fibrinolysis but also long r time. What treatment? A. FFP B. Cryoprecipitate C. Desmopressin D. Tranexamic acid TEG, think it was picture of low fibrinogen |
?D Check TEG pictures
if long r time = give FFP, if hyperfibrinolysis = give TXA |
|
|
[Nonum 5] Which is least likely to fraudulent research reduction strategy? |
POW = B RNS = D RPA = ?A Cram = ???A |
|
|
[Nonum 6] With respect to the triangle of safety and intercostal chest drain (ICC) insertion, if pectoralis major and the 4th - 5th intercostal space form two borders what forms the other? A. Latissimus dorsi B. Serratus anterior C. Midaxillary Line (maybe wasn't an option) D. Posterior Axillary Line (maybe wasn't an option) E. Trapezius |
A
http://thorax.bmj.com/content/58/suppl_2/ii53.full
Insertion should be in the “safe triangle” illustrated in fig 3⇓. This is the triangle bordered by the anterior border of the latissimus dorsi, the lateral border of the pectoralis major muscle, a line superior to the horizontal level of the nipple, and an apex below the axilla. |
|
|
[Nonum 7] Small picture trying to show USS probe on inferio-posterior R arm of a teenager's arm with an associated USS image of a very triangular looking peripheral nerve between two muscle fascia (radial N). |
D |
|
|
[Nonum 8] USS picture of an axillary brachial plexus nerve block with all four nerve unlabelled, the humerus, brachioradialis and biceps brachii marked. |
Review images |
|
|
[Nonum 9] Patient with known PAH with pulmonary pressures of 80/60 undergoing a lap cholecystectomy. About 20mins into case there is a sudden acute drop in SpO2 88%, hypotension. This is most likely to be? |
C
Pulmonary Hypertension is defined as a mean pulmonary artery pressure (PAP) >25mmHg at rest with a pulmonary capillary wedge pressure <12mmHg. Pulmonary hypertension is considered moderately severe when mean PAP >35mmHg. Right ventricular failure is unusual unless mean PAP is >50mmHg. Raised pulmonary vascular resistance (PVR) places an additional pressure load on the right ventricle. The right heart is poorly designed to deal with these increases in afterload. A rise in PVR and hence right ventricular afterload can put the right heart into failure. Left ventricular failure can then ensue, due to both reduced volume reaching the left heart, and septal interdependence. |
|
|
[Nonum 10] Paediatric intubation of 20kg, 5.5 doesnt fit, 4.5 doesn't fit, what next? |
?A
Pedisafe estimates 5mm tube should fit
ETT size (age/4)+4 Weight = (age+4) x 2 |
|
|
[Nonum 11] Trauma patient undergoes delayed ORIF tibia. Nerve block given. Induction consists of suxamethonium, propofol and an ETT. Cephalozin is given and rocuronium also given (long stem to confuse us). Suddenly bradycardic, ETCO2 45, MAP 50mmHg. This is most likely to be? |
E
(Bradycardia not likely with other causes) |