![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Consider the following arterial blood gases. (Ref ranges in brackets) pH 7.28 PaCO2 36 Bicarbonate 18 mmol.l-1 (18-25) Base excess -7 mmol.l-1 (-4- +3) Na+ 142 mmol.l-1 (135-145) Cl- 112 mmol.l-1 (98-110) These blood gases are consistent with A. acute renal failure B. diabetic ketoacidosis C. ethylene glycol overdose D. intraoperative infusion of 6 litres of normal saline E. salicylate overdose |
Answer D |
* Anion gap is normal (AG = 142 - 112 - 18 = 12)
* Hyperchloraemia is present * An acidaemia is present (pH<7.36) so there must be an acidosis present * pCo2 is low hence metabolic acidosis * Expected pCO2 = (1.5 x HCO3) + 8 (+/-2) = 27+8 = 35mmHg * Normal Anion Gap Metabolic Acidosis (renal loss of bicarb, GIT loss of bicarb, Dilution of bicarb by saline) * Best answer D but ? would have higher Cl |
|
|
You are performing a peribulbar block for eye surgery. You decide to add hyalase to your local anaesthetic mix. What is the recommended concentration for hyalase? A 25 U/ml B 50 U/ml C 100 U/ml D 150 U/ml E 1500 U/ml |
Answer A 25IU |
25 IU According to product information although with peribulbar anything from 7.5 IU/ml to 150 IU/ML has been recommended |
|
|
A 25 year old male presents for ECT at a free standing facility. He has a life threatening depressive illness that has not responded adequately to medication, however he is still taking tranylcypramine. The most appropriate course of action is A cancel the procedure, cease tranylcypramine and perform the ECT in 2 weeks B proceed with the ECT, but induce with midazolam and remifentanil C proceed with the ECT, but pre treat with esmolol D proceed with the ECT with caution, but with your usual drugs E transfer the patient to a tertiary centre for their ECT |
Answer D proceed with ECT |
CEACCP Fortunately, interactions withanaesthetic drugs (e.g. indirect sympathomimetics causing hypertensivecrises with either tricyclic antidepressants or monoamineoxidase inhibitors; meperidine or tramadol causing serotonin syndromewith SSRIs) are uncommon as the anaesthetic drugs inquestion are not generally required during ECT. |
|
|
A patient has been suffered a cardiac arrest. They are intubated but there is no IV access. Which drug can be given down the ETT? A Amiodarone B Calcium C Lignocaine D Magnesium E Sodium bicarbonate |
Answer C Lignocaine |
VENAL (i.e. horrible) V: vasopression E: epinephrine (adrenaline) N: naloxone A: atropine L: lidocaine |
|
|
A well 65 year old is having a total hip replacement under GA with sevo/nitrous/fentanyl. BP is 130/70 and stable. Before the surgeon commences reaming and cementing, the best thing to do is: A Induce hypotension B Raise BP with vasopressors C Turn off nitrous D Give steroids E Give heparin 5000u |
C turn of nitrous |
Stupid but is in the oxford handbook (allows 100% O2 to be given if emboli) |
|
|
Pt in ICU in their 20s is diagnosed with brain death. History is that of immunosuppression for a renal transplant but otherwise well (although brain dead, go figure). Patient has expressed a desire to be an organ donor. All these organs can be donated except A Bone marrow B Heart C Lung D Liver E Transplanted kidney |
A: Bone Marrow |
All others are possible. No reference found but fox news reports a transplanted kidney being transplanted 3 times |
|
|
What is the IV loading dose of paracetamol for a 16kg child? A <15mg/kg B 15mg/kg C 20mg/kg D >20mg/kg |
B 15mg/kg |
No loading dose in children over 44 weeks. Loading dose in neonates due to higher Vd, but decreased maintenance dose. "the dose of i.v. paracetamol in neonates and infants, when postmenstrual age is between 32 and 44 weeks, should be a loading dose of 20 mg kg−1 (or 2 ml kg−1) followed with a maintenance dose of 10 mg kg−1 (or 1 ml kg−1) every 6 h, ..... In older infants and children, the dose should be 15 mg kg−1 (or 1.5 ml kg−1) every 6 h. The interval between two maintenance doses should be increased up to 12 h if the neonate's postmenstrual age is between 28 and 31 weeks." Br. J. Anaesth. (2014) 112 (2):380-381. oral and rectal loading doses ORAL: 30mg/kg RECTAL: 40mg/kg |
|
|
Intralipid initial dose in mL/kg A 0.5 B 1 C 1.5 D 2 E 5 |
C 1.5ml/kg |
20% intralipid give 1.5ml/kg over 1 minute AND start infusion 15ml/kg/hr, can repeat bolus dose max x2, do not exceed 12ml/kg total can double rate to 30ml/kg/hr after 5 mins |
|
|
MELD score includes INR, Creatinine and: A Albumin B Bilirubin C AST D Fibrin |
B. Bilirubin |
The Model for End-Stage Liver Disease, or MELD, is a scoring system for assessing the severity of chronic liver disease. MELD uses the patient's values for serum bilirubin, serum creatinine, and the international normalized ratio for prothrombin time (INR) to predict survival. |
|
|
Factor V Leiden homozygote. By how much is the risk of post-operative DVT increased? A 2x B 5x C 10x D 20x E 50x |
E: 50x |
Factor V Leiden increases the risk of venous thrombosis 3- to 8-fold for heterozygous and 30- to 140-fold for homozygous individuals |
|
|
Kessel Blade has the blade coming off the handle at a degree of: A 80 B 95 C 110 D 135 E 150 |
C: 110 |
Various types of blades: * MacIntosh - commonest; blade attaches to handle at 90 degrees* Kessel - like the MacIntosh but the blade attaches at 110 degrees * McCoy - MacIntosh like blade with a moveable distal tip segment, flexed by a lever controlled by the thumb of the hand holding the handle to displace the larynx forwards * Magill - straight blade with U-shaped cross section * Miller and Wisconsin blades (straight blades with curved tips) |
|
|
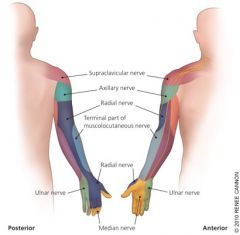
Surgery planned under brachial plexus block performed at axilla. Pain is felt on incision at the anterolateral right forearm. Which nerve has been insufficiently blocked? A Radial B Ulnar C Median D Musculocutaneous E Median brachial cutaneous |
D. Musculocutaneous |
|
|
|
55M ICH, ventilated, paralysed, sedated, ICPs persistently 25mmg A cool to < 35 degrees B give hypertonic saline C dexamethasone D position 45 degrees head up E Ventilate to PaCO2 <30 |
B. give hypertonic saline |

|
|
|
Best method to prolong apnoeic oxygen saturation in obese patient: A position head up B place in sniffing position C prone D lateral |
A. Position Head Up |
CEACCP - physiology of apnoea 2009 For severely obese patients (BMI>40 kg m−2), preoxygenation of these patients in the 25° head-up position achieves oxygen tensions >20% higher than when preoxygenation is applied in the supine position |
|
|
Neonate (born at 40 weeks, now 7 weeks old) why to reduce morphine infusion rate compared with older child A Increased morphine crossing BBB B Increased total body water/decreased fat C Decreased enzymatic hepatic function D Increased morphine-3-glucuronide (definitely M3G) |
C. Decreased enzymatic hepatic function also A seems correct |
CEACCP - Analgesia in neonates Reduced doses of morphine are required in neonates because of an increased effect of the drug due to an immature blood–brain barrier, reduced protein binding (28% as opposed to 50% in the older child) producing a higher free drug level and a long duration of action because of immature liver metabolism and reduced renal excretion |
|
|
Motor evoked potentials are used to monitor spinal cord function in scoliosis surgery. Which drugs affect them the LEAST? A. Non-depolarising muscle relaxants B. Nitrous Oxide C. Opiods D. Propofol E. Volatiles |
C. Opioids |
https://www.openanesthesia.org/evoked_potentials_anesthetic_effects/
MEPs are exquisitely sensitive to anesthetics, especially inhalational agents. Volatiles, therefore, should be avoided during recording of myogenic MEPs. Benzodiazepines, barbiturates, and propofol all depress MEPs, however, adequate recordings can be obtained during propofol anesthesia by controlling serum levels and increasing stimuli rates. Muscle relaxants can affect the recorded EMG response by depressing myoneural transmission. However, adequate MEP recordings can be achieved as long as one or two twitches on TOF can be maintained. |
|
|
At initiation of laparoscopy/pneumoperitoneum which of the following cardiovascular parameters is LEAST likely to increase? A. Cardiac Output B. Mean Arterial Pressure C. Heart rate D. Myocardial filling pressures E. Systemic Vascular Resistance |
E SVR |
Initially VR increases, increasing cardiac filling pressures and cardiac output. SVR won't increase initially, it will later |
|
|
In order to use a 3 lead ECG setup to gain a CS5 view which of the following configurations would you use? A. Lead I, RA lead below the clavicle, LA lead in the V5 position, LL at the hip B. Lead I RA lead below the clavicle, LA lead at the hip LL in the V5 position C Lead II RA lead below the clavicle, LA lead in the V5 position, LL at the hip D Lead III RA lead below the clavicle, LA lead in the V5 position, LL at the hip E Lead III RA lead below the clavicle, LA lead at the hip LL in the V5 position |
A. This mode is designed for anterior wall ischaemia and thus lead 1 is the best to watch |

Central Subclavicular Lead The central subclavicular (CS 5 ) lead (see Fig. 13-3 ) is particularly well suited for the detection of anterior wall myocardial ischemia. The right arm (RA) electrode is placed under the right clavicle, the left arm (LA) electrode is placed in the V 5 position, and the left leg electrode is in its usual position to serve as a neutral lead. Lead I is selected for detection of anterior wall ischemia, and lead II can be selected either for monitoring inferior wall ischemia or for the detection of arrhythmias. If a unipolar precordial electrode is unavailable, this CS 5 bipolar lead is the best and easiest alternative to a true V 5 lead for monitoring myocardial ischemia. |
|
|
According to NAP4 what is the rate of failure for emergency cannula cricothyroidotomy? A 10 B 20 C 40 D 60 E 80 |
D - 60% |
There was a high failure rate of emergency cannulacricothyroidotomy, approximately 60%. In contrast a surgical technique for emergency surgicalairway was almost universally successful |
|
|
Arndt bronchial blocker picture what is the straight port on the multi lumen connector for? A Connection of tracheal tube B Passage of nylon guide wire C Passage of fibreoptic D Passage of bronchial blocker E Connect circuit |
C. fibreoptic |

|
|
|
Which would be consistent with deep partial thickness burns? A Pain to deep pressure only, decreased capillary refill or doesn’t blanch B Blanches to pressure, very painful C Painful to air, blanches to pressure with blisters? D Painful to deep pressure, red and weeping/wet E No pain, no CRT |
A - decreased sensation, no capillary refill |

|
|
|
How many vials of dantrolene should (according to guidelines from MH society) be kept at a remote hospital which has general anaesthesia services? A 2 B 6 C 12 D 24 E 36 |
E: 36 vials |
Dantrolene stocks:The mhanz group recommends that a minimum of 24 (20mg) vials of dantrolene are held in any anaesthetising location where triggering anaesthesia is performed. Larger or remote hospitals should carry 36 vials.This stock level represents 2-3 x 2.5mg/kg doses for an average sized adultand is a reasonable compromise between clinical need and economy. |
|
|
Pregnant patient, progressive dyspnoea. Which would most strongly warrant further investigation? A soft 2/6 systolic ejection murmur B elevated JVP C third heart sound D orthopnoea E peripheral oedema at ankles |
D - orthopnea |
A,B,C,E all occur normally during pregnancy |
|
|
How long before return to normal platelet function in chronic diclofenac use. A 12hrs B 1-2d C 4d D 7d E 10d |
C 4 days |
Ex vivo tests of platelet aggregation, such as second-wave aggregation to ADP or epinephrine after a single dose of drug, show prolongation for 3 days after piroxicam, 2 days after naproxen, diclofenac, and indomethacin, and about 1 day after ibuprofen. With chronic administration, the time taken for return of normal platelet function may be considerably longer, due to accumulation of products such as the S(+) enantiomer of ibuprofen in adipose tissue |
|
|
How long after starting a unit of FFP does it have to be completed A 2hrs B 4 C 6 D 8 E 10hrs |
B. 4 hours |
The transfusion should normally be completed within four hours of the product leaving approvedcontrolled storage (or sooner if specified on the pack / transfusion report). |
|
|
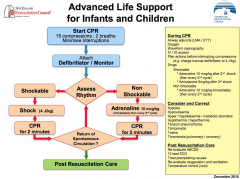
You arrive to a code blue for a 5 year old child 16kg in a shockable rhythm. CPR has commenced, he has had TWO shocks already. What is the next step: A Adrenaline B Amiodarone C Iv fluid bolus D Shock 50j E Shock 100j |
A: Adrenaline 10mcg/kg |
|
|
|
143. FAST scan includes A Pelvis, pericardium, perihepatic, perisplenic B Pelvis, pericardium, perihepatic, paracolic C Lung, pericardium, perihepatic, perisplenic D More combinations of above
|
A: pelvis, pericardium, perihepatic, perisplenic
|
The four classic areas that are examined for free fluid are the perihepatic space (also called Morison's pouch or the hepatorenal recess), perisplenic space, pericardium, and the pelvis
|
|
|
144. You arrive in the emergency department to treat a man with an attempted hanging. He has a LMA in situ, it is easy to ventilate (or something like that) Sa 98% HR 120, BP 130/80 GCS 5 initially. What is the next single most important thing to do. A Apply rigid collar with manual inline stabilisation B Check subcutaneous emphysema C Fibre optic examination of airway D Lateral c-spine xray E Remove LMA and intubate
|
B. Check subcutaneous emphysema
|
Easy to do and major sign of laryngotrachael seperation |
|
|
ou are supplying oxygen from the variable flow meter on the wall at 6L/min. The tubing becomes obstructed. What is the pressure reached in the tubing A 1atm (100kPa) B 2atm (200kPa) C 3atm (300kPa) D 4atm (400kPa) E 5atm (500kPa)
|
D 4 atm
|
Would return to O2 wall supply which is 4atm |
|
|
The adverse event that leads to the most medico legal claims against anaesthetists is: A Dental damage from airway management B Eye injury C Non-obstetric epidural complications D Obstetric epidural complications E Peripheral nerve injury
|
A. Dental damage
|
According to MDA 48% Anaesthesia – dental issues 17% Anaesthesia – CNS/CVS & potential medium/high value matters 12% Anaesthesia – nerve & musculo skeletal injuries – direct /pressure/ positioning 5% Anaesthesia – inadequate pain relief/awareness 3% Medication related 3% Consent issues 1% Diagnosis 1% General duty of care 1% Treatment 9% Other |
|
|
65 year old lady with osteoarthritis, for TKR in 2 weeks time. She has Fe deficiency anaemia, with Hb 105, Ferritin 30mcg/l. The best management would be: A Oral Fe tablets until surgery B Oral Multivitamin containing Fe until surgery C IV Fe infusion D Blood transfusion E Check Hb on day of surgery and don't proceed if <95 |
C IV iron infusion |
|
|
|
What is the expected rise in platelets from one unit of pooled leucodepleted plates in a 70kg patient? A 10-20 B 21-40 C 40-60 D 60-80 E 80-100 |
B 21-40 |
www.transfusion.com.au |
|
|
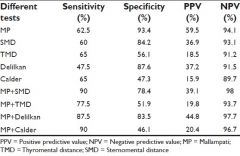
You are assessing a patient for intubation. MP3 and thyromental distance 6cm. Compared with MP, TMD is? More or less specific |
|
|
|
|
You are about the anaesthetise a patient BMI 38 for bariatric surgery. Plan to give 1m/kg of sux. Compared with Ideal body weight, total body weight dosing resulst in: A shorter onset, shorter duration B shorter onset, similar duration C shorter onset, longer duration D similar onset, shorter duration E similar onset, longer duration |
E Similar onset, longer duration |
Lemmens HJ, Brodsky JB. The dose of succinylcholine in morbidobesity. Anesth Analg 2006; 102: 438–42 |
|
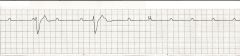
man undergoing transcatheter aortic valve replacement has this ECG. What is the best way of managing this: A Atropine B Transcutaneous pacing C Adreline D Isoprenaline E Transvenous pacing |
e. Transvenous pacing |
CEACCP The transvenous pacing wire can be used in thecase of complete heart block, and this (or epicardial wires aftertransapical approach) is left in situ immediately after operation incase of delayed heart block. |
|
|
A patient presents for THR with a febrile illness, but wishes to proceed despite the risks. You can justify your decision to defer the case based on: A Automony B Beneficence C Non-maleficence D Paternalism E Utilitarianism |
C. Non-maleficence |
|
|
|
You collect ropivacaine levels post-operatively. This type of data is: A Continuous B Numerical C Ordinal D Nominal E Categorical |
A Continuous |
its continuous numerical data |
|
|
Randomised controlled trial means: A Patients randomly allocated to treatment groups B Patients randomly allocated to treatment or placebo C Patients allocated systematically D Neither the patient nor the investigator knows which group the patient is in E ? |
B. randomly allocated to treatment or placebo (control) |
|
|
|
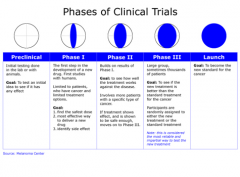
Clinical phase III trial means: A dose finding B In patients WITHOUT the disease C Randomised controlled trial in patients D Post marketing study E ? |
C. RCTs |
|
|
|
Cancer patient on subcutaneous morphine, 70mg in 24 hours. Converting this to an oral dose of long acting morphine. What is a reasonable starting dose? A 25mg bd B 70mg bd C 100mg bd D 150mg bd E 200mg bd |
B. 70mg BD |
3x for reduced bioavailibity then reduce to be safe with variability |
|
|
Neurosurgery in the sitting position. What is the most sensitive way to detect venous air embolism? A Praecordial doppler B PA Catheter C TOE D ET CO2 E ? |
C TOE |
The transesophageal echocardiography is the most sensitive monitoring; it can detect 0.02 ml/kg of air injected by bolus administration or air bubbles as small as 5-10 microns.[35]Precordial doppler ultrasound is the most sensitive non-invasive monitoring which can detect as little as 0.05 ml/kg of air.[36]End tidal nitrogen (ETN2) can show the changes 30-90 seconds earlier than end-tidal carbon dioxide (ETCO2) changes.[37]End-tidal carbon dioxide (ETCO2) is the most common and easily available monitoring, which will reveal sudden decrease in level in event of VAE |
|
|
Modified from previous - CS5 – what are the lead arrangements and lead examined. No information about what you are looking for (ie region or rhythm vs. ischaemia) A RA at R subclavian, LA at V5, LL at L hip, lead I B RA at R subclavian, LA at hip, LL at V5, lead I C RA at R subclavian, LA at V5, LL at L hip lead II D RA at R subclavian, LA at left hip, LL at V5 lead III E RA at R subclavian, LA at V5, LL at L hip, lead III |
A RA at R subclavian and LA at V5, LL lower than this want to monitor V5 for ant ischaemia |
Millers 8th ed Modified chest leads such as CS 5 (the RA electrode is placed under the right clavicle, and the LA electrode is placed in the V 5 position) or CB 5 (the RA electrode is placed over the center of the right scapula, and the LA electrode is placed in the V 5 position) may be suitable for the detection of anterior wall myocardial ischemia; however, these modified leads are currently not recommended for monitoring myocardial ischemia. |
|
|
70kg man , burns to 50% of body, according to parkland, how much fluid in first 8 hours A 2.4 B 3.6 C 4.6 D 7L E 14L |
d 7L |
4x70x50 = 14L in 24 hours 1/2 in 1st 8 hrs = 7L |
|
|
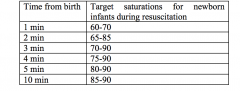
You arrive at the delivery of a term neonate with resuscitation in progress. At 2 minutes, saturations are 70%, child is breathing, has been dried and is warm. A HR was also given which was more than 60. What do you do? A Observe B Mask ventilation C 100% oxygen D ? |
A. Observe |
|
|
|
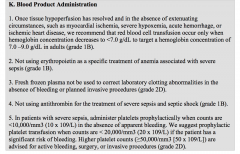
65 male patient in ICU with severe, overwhelming sepsis, Hb 75, INR 1.5, CvSO2 70%. What product do you give? A Nothing B 1 unit red cells C 1 unit red cells and PTx D 1 unit red cells and FFPE 2 bags FFP |
A. Nothing |
|
|
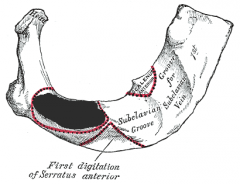
what is the structure that attaches to the shaded area: A Scalenus medius B Saclenus anterior C SCM D Parietal pleura E Articular surface with clavicle |
A. Scalenus medius |
|
|
|
Praecordial thump indicated when A Witnessed, monitored: VT B Witnessed monitored VF C Witnessed but unmonitored arrest D Witnessed monitored asystole |
A: Witnessed, monitored VT |
http://resus.org.au/guidelines/ |
|
|
85 F for fracture hip, otherwise well, normal ECG day prior, electrolytes normal. Otherwise well other than now in AF with HR 110-145, BP 130/80 what do you do: A Amiodarone B DC Cardioversion post induction GA C Digoxin D Metoprolol E Anticoagulate |
D. Metoprolol |
Rate control with B-blocker unless LV impairment then use diltiazem or amiodarone |
|
|
How many weeks of anticoagulation prior to elective DCR per AHA/ACC A 1 week B 2 weeks C 3 weeks D 4 weeks E 5 weeks |
C. 3 weeks |
For patients with AF or atrial flutter of 48 hours’ duration or longer, or when the duration of AF is unknown, anticoagulation with warfarin (INR 2.0 to 3.0) is recommended for at least 3 weeks before and 4 weeks after cardioversion |
|
|
Child for elective procedure, maternal GREAT-grandfather had MH. What is the most reassuring that he doesn’t have MH A Exposure to halothane age 2 without incident B Maternal grandfather negative IVCT C Mother negative genetic test D No other reports in family despite multiple exposure E Normal serum CK |
B. Maternal grandfather negative IVCT |
A. incorrect as many have normal anaesthetics prior to MH C. incorrect as not or genes known |
|
|
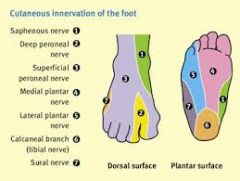
Ankle bock what supplies plantar foot A deep peroneal B posterior tibial C superficial peroneal D sural E saphenous |
B. posterior tibial |
|
|
|
Interscalene block – what is most likely to be missed: A Medial cutaneous nerve of forearm B Radial nerve C Median nerve D Axillary nerve |
A. Medial cutaneous nerve of forearm |
interscalene misses C8 T1 and inferior trunk - sole supply of MCN forearm |
|
|
Pregnant woman, 33 weeks, thyroid storm for an urgent caesarean section, already been treated with steroid. What next? A Carbimazole B Esmolol C IV magnesium D Propothyiouracil E Potassium Iodide |
D PTU |
|
|
|
65 year old, 3 days postop, hypoxia, VQ scan shows non-segmental, matched perfusion and ventilation defects. A Asthma B Emphysema C PE D Atelectasis E Pulmonary infarction |
D Atelectasis |
low likelihood of PE, infarction more likely to be segmental if pneumonia is an option choose pneumonia |
|
|
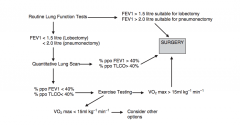
45 year old man with left lung cancer. Otherwise well and CT shows no metastasis. FEV1 2.3 L and FVC 3.4 L. Do you? A Proceed with either pneumonectomy or lobectomy B Lobectomy only C Assess split function (Refer for V/Q scanning) D Formal cardiopulmonary exercise testing E cancel all surgery |
A. Proceed with either pneumonectomy or lobectomy |
|
|
|
You are called to the cardiac catheter lab to assist when a 55-year-old man with unstable angina becomes restless during difficult placement of a right coronary artery stent. When you arrive he is conscious and responding to voice. He is sweating with a pulse of 60 beats per minute in sinus rhythm, blood pressure measured from arterial catheter of 80/50 mmHg and Sp02 of 97%. The arterial pressure wave has an exaggerated fall with inspiration. The most appropriate next clinical intervention would be to A. administer atropine B. commence an adrenalin infusion C. perform a quick transthoracic echocardiograph D. sedate and intubate E. transfer to operating theatre immediately |
C perform a quick TTE |
?pericardial effusion / tamponade |
|
|
Lithotomy position for laparoscopy. What is not a risk factor for compartment syndrome lower leg? A) obesity B) male gender C) lithotomy stirrups D) pmh hypertension E) intraoperative hypotension |
C. lithotomy stirrups vs full calf supports have been shown to have no difference |
|
|
|
You are called to review a patient in recovery who is short of breath after resection of a lung SCC. He is weak, cannot flex hips or lift arms. He was given atracurium (35mg) which was reversed 90 minutes ago. This is most consistent with: A Eaton lambert B Myasthenia gravis C Steroid induced myopathy D Limb girdle muscular dystrophy E Myotonic dystrophy |
A Eaton Lambert |
Eaton–Lambert syndrome (myasthenic syndrome) is proximal myopathy associated with small cell carcinoma. Reduction in acetylcholine released from presynaptic motor nerve terminals in these patients causes increased sensitivity to all neuromuscular blocking drugs. In contrast to myasthenia gravis, the muscle weakness improves with exercise and is not reversed by acetyl cholinesterase inhibitor therapy |
|
|
According to ANZCA professional standards, a LEVEL 2 machine check includes: A: Ensuring that there are no leaks both when the vaporisers are being used and when they are not being used. B: Checking the breathing circuit if it has been changed C: Checking the inspiratory and expiratory valves D: Checking the (?external) scavenging system E: Checking the reserve oxygen cylinder is adequately filled for its intended purpose |
A. check for leaks |
|
|
|
Rate of CO2 rise with apnoea in normal adult. |
12mmHg in first minute, then 3.4mmHg per minute after |
|
|
|
Which is least likely to have a difficult airway? A: Apert syndrome B: Downs syndrome C: Treacher Collins syndrome D: Hurler E: ? |
Downs |
Hypoplastic mandible (micrognathia) – difficult intubation * Pierre Robin sequence
* Treacher Collins * Hemifacial microsomia (Goldenhar syndrome) * Apert syndrome * Crouzon syndrome * Pfeiffer syndrome * Saethre-Chotzen syndrome * Hurler’s/Hunter’s syndrome (mucopolysaccharidoses) * Beckwith-Wiedemann syndrome * Down’s syndrome |
|
|
When to send tryptase after suspected anaphylaxis: A. 1 hr B. 4 hrs C. ? D. ? E. 24 hrs |
A 1hr |
|
|
|
Patient unstable with PE after joint replacement (tachycardiac and hypotensive), already heparinised. A: Thrombolysis B: Referral for thrombectomy C: Supportive care including fluids and inotropes D: E: |
B. referral for thrombectomy |
|
|
|
Prothrombinex is relatively contraindicated in a bleeding patient with: |
A past history of HITS |
|
|
|
Subtenon is relatively contraindicated in: A: Long axial length B: Previous scleral band which remains in situ C: Inferonasal pterygium D: E: |
B. Previous scleral band |
The technique is relativelycontraindicated where there is a history of scleral diseasewith possible scarring and friability of the sclera. Previousretinal detachment surgery can be associated with scleralbuckles and adhesions, which may hinder dissection orspread of anaesthetic solution, and increase the risk of globeperforation in the quadrant dissected. |
|
|
On CPB. MAP drops very low after first dose cardioplegia. Mixed venous sats 80%. What to do? A: Metaraminol B: Start an adrenaline infusion C: Give fluid D: Change pump flow rates E: |
A. Metaraminol |
Adjusting blood pressure • Vary pump flow rate – not commonly used. Low flows compromise perfusion. High flows increase blood trauma. Can be used briefly for periods of very low or high blood pressure. • Increasing SVR – the primary control of BP in most cases. Phenylephrine or metaraminol boluses. Norepinephrine (noradrenaline) or vasopressin can be used when SVR becomes less responsive to these. Vasopressin therapy is currently popular for ‘vasoplegia’ secondary to cardiopulmonary bypass. • Decreasing SVR – anaesthesia. Within reason! It is easy to use vasodilators and vasoconstrictors. Dialling up very high or very low volatile agents produces a slow response and does not treat the cause if adequate anaesthesia is assured. Opioids are quite useful – remifentanil produces particularly stable conditions. Vasodilators – GTN boluses or infusions, phentolamine, sodium nitroprusside. |
|
|
According to the current (2010) ARC ALS guidelines, what is the correct dose for the first three shocks of a shockable rhythm? A: Biphasic 50, 100, 150 B: Biphasic 100, 150, 200 C: Biphasic 100, 200, 200 D: Monophasic 120, 240, 360 E: Monophasic 360, 360, 360. |
E. monophasic 360 360 360 |
All others are incorrect Biphasic 200 200 200 |
|
|
What is not a sign of damage to a part of the sympathetic system? [In the context of surgery where something sympathetic related could be damaged] A: Blepharoptosis B: Exopthalmos C: Facial flushing D: Miosis E: |
B exopthalmus |
Enopthalmus is a sign of sympathetic trunk damage Miosis, ptosis, anhidrosis |
|
|
Providing sedation for endoscopy. What must you have? A: Anaesthetic machine B: Suxamethonium C: Mechanical ventilator D: Defibrillator E: Laryngoscope |
D. Defibrillator |
?laryngoscope as well (states need for advanced airway equipment) |
|
|
Abdominal compartment syndrome is diagnosed when intra-abdominal pressures are consistently greater than A: 12mmHg B: 20mmHg C: 24mmHg D: E: |
B 20mmHg |
|
|
|
Patient with respiratory failure, low PaO2/FiO2 ratio, cardiac index of 1.7, PCWP of 25. Which mode of ECMO would be most appropriate? A: VA B: VV C: AV D: E: |
B:VV |
VA-ECMO can be considered in patients with systolic arterial pressure lower than 85 mm Hg, cardiac index lower than 1.2 litre min−1 m−2, despite adequate preload, more than two inotropes in use, intra-aortic balloon counterpulsation, and systemic signs of low cardiac output |
|
|
When to stop dabigatran (for non valvular AF) in a patient with normal renal function prior to THR planned to be done under spinal? A: 7 days B: 3 days C: 3 days, bridge with clexane D: 5 days E: Continue until day of surgery |
C. 3 days Bridge with clexane |
2-3 half lives is lower recommendation 6 half-lives is safer BJA article suggests 5 halflives with bridging (4 days) |
|
|
What do you expect to happen if you put a magnet over an AICD?A: Turn off antitachycardia feature, no change to pacing B: Turn defib off, asynchronous pacing C: Turn defib off, no change to pacing (or, continue synchronous pacing) D: No change to defib, asynchronous pacing E: |
A |
|
|
|
Young patient, recently diagnosed with phaeochromocytoma. Not on any medications. Presents to ED tachycardic (~140) with SBP 220. Best initial treatment: A: Phenoxybenzamine B: Phentolamine C: Esmolol D: GTN E: |
B. phentolamine |
phenoxybenzamine takes to long to work. esmolol contraindicated until alpha blockade established. GTN or SNP also options (2nd line) |
|
|
Technique to minimise absorption of irrigation fluid during TURP: A: Fluid no more than 60cm above the patient B: Use NS rather than glycine C: Use laser D: Limited resection of gland only if gland <200g E: |
A. bag height <= 60cm |
|
|
|
Recent case with LMA. Now has hoarse voice. Nasendoscopy shows one vocal cord in the paramedian position. What is the site of injury? A: Lingual n.; B: Vagus n.; C: Superior laryngeal n.; D: Recurrent laryngeal n. E: |
D Recurrent laryngeal nerve |
|
|
|
A 34 year old primigravida collapses soon after delivery of her baby, the presumptive diagnosis is amniotic fluid embolus. Which ONE of the following supports this diagnosis? A markedly raised serum tryptase B decreased C3-C4 levels C thrombocytosis D raised CRP E hyperfibrinogenemia |
B decreased C3-C4 levels |
|
|
|
A 30 year old woman is admitted to ICU after a 500mg/kg aspirin overdose. What is the most effective therapy to enhance her elimination of the aspirin? A. Frusemide B. Haemodialysis C. Mannitol D. 0.9% sodium chloride E. Sodium bicarbonate |
B. Haemodialysis |
|
|
|
Endovascular coiling of cerebral aneurysm under GA, patient suddenly develop hypertension. What is the most likely cause? A. Acute hydrocephalus B. Rupture of aneurysm C. Contrast reaction D. Cerebral embolism E. Nothing |
B. Rupture of aneurysm |
|
|
|
A 70 year old is is intubated and ventilated post-laparotomy. He has CSL running @60ml/hr, with an NGT on suction with continuing high output. His ABG shows an appropriate pO2, pCO2 32, pH 7.66, Na 144, K 3.5, Cl 76. He has a normal creatinine and raised urea. How should you improve his acid base status? (Had a very very very long stem, with very long answers, but this was the gist, and I'm pretty confident with the answers except the first 2 fluid options). A Leave minute ventilation unchanged, (?leave fluids unchanged), commence PPI B Leave minute ventilation unchanged, (?leave fluids unchanged), commence acetazolamide C Increase minute ventilation, change IVF to normal saline, commence PPI D Increase minute ventilation, increase the fluid rate, commence acetazolamide E Increase minute ventilation, leave fluids unchanged, commence acetazolamide |
A. PPI to decrease gastric acid, unchanged minute ventilation |
|
|
|
Risk of bone cement implantation syndrome increased with A: Increasing age B: Male gender C: ? D: ? E: Previous exposure to cement |
Increasing Age |
Patient risk factors that have been implicated in genesis of BCIS after cemented THRs include grade III and IV ASA levels, old age, poor pre-existing physical reserve, impaired cardiopulmonary function, pre-existing pulmonary hypertension, osteoporosis, bony metastases, and concomitant hip fractures, particularly pathological or intertrochanteric fractures. |
|
|
Sux left out of fridge for 1 week. How much has its efficacy reduced A: 2% B: 5% C:10% D: 0.5% E: ? |
D 2.1% degredation per month |
|
|
|
Risk of blood transfusion reaction with group specific ABO + Rh matching, but not cross matched A: B: C: D: 98.? E: 99.8 |
E |
|
|
|
Best way to reduce chance of auto-PEEP occurring is to increase A: Expiratory time B: Inspiratory time C; Respiratory rate D: ? E: Amount of positive pressure ventilation |
A |
|
|
|
Patient having a laparotomy. What is the best method for intraoperative optimisation of fluid therapy? A. Arterial pulse pressure contour analysis B. EF on a TOE C. CVP (or PCWP) D. BP E. HR |
A |
|
|
|
In tetralogy of fallout, the degree of cyanosis is associated with: A: The size of the VSD B: The position of the VSD C: The degree of RV outflow obstruction D: E: |
C: The degree of RV outflow obstruction |
The physiologic consequences of TOF are largely dependent upon the degree of right ventricular outflow obstruction. Since the VSD is typically large and unrestrictive, the pressure in the right ventricle reflects that of the left ventricle. As a result, the direction of blood flow across the VSD will be determined by the path of least resistance for blood flow, not by the size of the VSD. If the resistance to blood flow across the obstructed right ventricular outflow tract is less than the resistance to flow out of the aorta into the systemic circulation, blood will naturally shunt from the left ventricle to the right ventricle and into the pulmonary bed. In this situation, there is predominately a left-to-right shunt and the patient will be acyanotic.As the degree of right ventricular outflow obstruction increases, the resistance to blood flow into the pulmonary bed also increases. If the right ventricular obstruction is significant enough to increase resistance, it will be easier for blood to cross the VSD from the right ventricle into the left ventricle and go out the aorta, which now becomes the path of least resistance. This right-to-left shunt across the VSD will result in a large volume of desaturated blood entering the systemic circulation and cyanosis and polycythemia will ensue |
|
|
You area trialling a new drug for hypertension in one group of patients and comparing it to placebo (given to another group). In three months time you will measure the blood pressure and want to compare the two groups. Which test would be most appropriate? A: Chi squared B: Fishers exact test C: Student's t-test D: Mann-whitney U test E: Bland Altman test |
A. Student's T Test |
|
|
|
In an adult, the spinal cord ends at the caudal end of which vertebral body? A: L1 B: L2 C: T12 D: S2 E: |
A L1 |
|
|
|
SAH, all associated with poor prognosis except: A: Pulmonary oedema B: Stunned myocardium C: Fever D: Delayed ischaemia E: |
B. Stunned Myocardium |
|
|
|
What is the smallest ETT that can be railroaded over an aintree catheter? A: 5.5 B: 6.0 C: 6.5 D: 7.0 E: 7.5 |
C 6.5 |
manufacturer says 7.0, but you can fit a 6.5 (??which one do they want) |
|
|
Which nerves need to blocked to anaesthetise the hard palate ? A. Superior labial nerve and greater palatine nerve B. Greater palatine nerve and nasopalatine nerve C. Inferior orbital nerve and nasopalatine nerve D. Glossopharyngeal nerve and…E. Anterior ethmoidal nerve and… |
B. Greater palatine nerve and nasopalatine nerve |
|
|
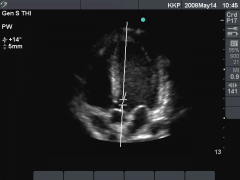
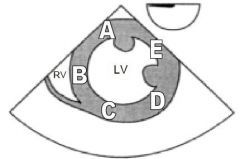
TTE with 5 chamber view. What is the marker on? A Aortic valve B Mitral valve C Pulmonary valve D Tricuspid ValveE |
A Aortic Valve |
|
|
TOE transgastric short axis view of LV. Label on D What coronary territory is it? A LCx B LAD C PDA D RCA E ? |
A. LCX |

|
|
|
RFTs – No clinical stem, just RFTs with FEV normal, FVC normal, FEV/FVC ratio 89%, DLCO 44%, RV and TLC both 80-90% A Asthma B COPD C Pulmonary haemorrhage D Pulmonary fibrosis E Pulmonary arterial hypertension |
E Pulmonary arterial hypertension |
Pulmonary vascular disease — An abnormal DLCO may be due to pulmonary vascular disease in those patients with chronic dyspnea but normal spirometry and lung volumes |
|
|
Pre-operative bowel prep: A Reduces Mortality B Reduces wound infection rates C Reduces anastamotic leak rates D Reduces re-operation rates E Facilitates colonoscopy |
E Facilitates colonoscopy |
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2993029/ |
|
|
Propofol infusion syndrome involves all of the following except: A Rhabdomyolysis B Hepatomegaly C Splenomegaly D ST elevation |
C Splenomegaly |
Also metabolic acidosis and hyperlipidemia |
|
|
Awareness incidence rate with GA under muscle relaxant from NAP5 A 1:1000 B 1:3000 C1:8000 D 1:10,000 E 1:50,000 |
C 1:8000 |
|
|
|
Question about most common symptom associated with post-op neurological dysfunction A Short term memory loss B Agitation C Hallucinations D Decreased executive function E Delirium |
A Short term memory loss |
|
|
|
Patient with a large anterior mediastinal mass, develops hypoxia on induction, best management? A Prone position B Intubate and ventilate with IPPV C Intubate and try to keep spontaneously breathing D Deliver CPAP |
A Prone position |
|
|
|
72 year old has had hip replacement surgery and 3 days postop has a pulmonary embolus. He is fully heparinised, but still dyspnoeic, clammy, BP 80/40, pulse 120 and CVP 18. The most appropriate next step is A. IVC filter B. Refer him for a pulmonary embolectomy C. Supportive (fluids and inotropes) D. Thrombolysis E. Warfarin |
B. Refer for a pulmonary embolectomy |
|
|
|
You are about the anaesthetise a patient BMI 38 for bariatric surgery. Plan to give 1m/kg of sux. Compared with Ideal body weight, total body weight dosing resulst in: A shorter onset, shorter duration B shorter onset, similar duration C shorter onset, longer duration D similar onset, shorter duration E similar onset, longer duration |
E |
The Dose of Succinylcholine in Morbid Obesity. A & A February 2006 vol. 102 no. 2 438-442• No difference in time of onset between IBW, LBW or TBW• Recovery intervals shorter for patients dosed based on IBW and LBW rather than TBW |
|
|
How many weeks of anticoagulation prior to elective DCR per AHA/ACC A 1 week B 2 weeks C 3 weeks D 4 weeks E 5 weeks |
C |
For patients with AF or atrial flutter of 48 hours’ duration or longer, or when the duration of AF is unknown, anticoagulation with warfarin (INR 2.0 to 3.0) is recommended for at least 3 weeks before and 4 weeks after cardioversion, regardless of the CHA2DS2-VASc score and the method (electrical or pharmacological) used to restore sinus rhythm(From AHA guidelines) |
|
|
Chronic pain after mastectomy is not related to: a. age b. low levels of anxiety before c. intercostal injury d. blocks |
A |
|