![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
|
Muscarinic Agonists |
AcetylCHOLine BethaneCHOL methaCHOLine Pilocarpine -side-effects - diarrhea, urination, miosis, bradycardia, bronchoconstriction, lacrimation, salivation, sweating, CNS stimulation Nicotinic effects- skeletal muscle excitation + CNS stimulation |
|
|
Acetylcholine
|
Acts on Muscarinic and Nicotnic receptors Short half-life, no clinical use |
|
|
Bethanechol
|
M only Rx- postop/neurgenic ileus, urinary retension |
|
|
Methacholine |
M > N Diagnosis of asthma (bronchial hyperreactivity) -causes wheezing in ashtmatic patients |
|
|
Pilocarpine |
M only
Rx- glaucoma (topical, xerostomia) Can be used to increase sweat for sweat testing for CF |
|
|
Acetylcholinesterase inhibitors |
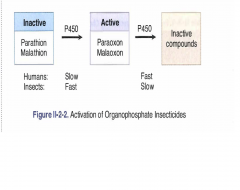
-Edrophonium, physotigmine, neostigmine, pyridostigmine, donepezil, organophosphate (parathion, malthion)
-can cause cholinergic crisis due to desensitized *can die from diaphragmatic paralysis -side-effects - Diarrhea, urination, miosis, bradycardia, bronchoconstriction, emesis, excitation, lacrimation, salivation, sweating |
|
|
Edrophonium (tensilon)
|
-Short acting
-used to diagnose Myasthenia -used to differentiate myasthenia from cholinergic crisis** -MG will improve, choliergic crisis won't |
|
|
Physostigmine
|
Tertiary amine-nonpolar-NRH2-enters CNS
Rx- glaucoma, atropine toxicity |
|
|
Neostigmine, pyridostigmine |
Quaternary amine- NRH3+-polar-does not cross BBB
Rx- ileus, urinary retention, myasthenia, reversal of nonpolarizing NM blocker (quarare) |
|
|
Donepezil
|
Lipid soluable
Rx- alzheimer- due to loss of ACh neurons in meynert's nucleus |
|
|
Organophosphates * -malathion, parathion (insecticides) -Sarin (nerve gas) |
|
|
|
Management of organo-phosphate toxicity
|
Treat muscarinic effects: Atropine
Regeneration of AChE: Pralidoxime (2-PAM) *Require this asap! or else it ages and becomes irreversible! |
|
|
Pralidoxime (2-PAM)
|
Replaces R-P-AChE to R-P-2-PAM = regeneration of AChE
-Requires the R group in order for this to occur -after it "ages", the R-P-AChE loses R and becomes the permanent P-AChE
-2-3 minutes in nerve gas |
|
|
Chronic toxicity due to organophosphate |
Looks like multiple sclerosis
-peripheral neuropathy- muscle weakness/sensory loss -demyelination due to organophosphate being lipid soluable- goes through myelin and damage it |
|
|
Atropine
|
Muscarinic receptor antagonist Effects- Decreased secretion, mydrasis and cycloplegia, hyperthermia (cause vasodilation, tachycardia, sedation, urinary retention and constipation, urinary retention and constipation Behavior: excitation and hallucination |
|
|
Other drugs with antimuscarinic pharmacology |
1. antihistamines 2. tricyclic antidepressants 3. Antipsychotics 4. Quinidine 5. Amantadine 6. Meperidine |
|
|
Treatment of acute atropine intoxication |
Symptomatic +- physostigmine |
|
|
Atropine -clinical uses |
Antispasmodic, antisecretory, management of AChE inhibitor OD, Antidiarrheal, ophthalmology (long action) |
|
|
Tropicamide |
Ophthalmology (topical) - shorter half-life than atropine so sometime they use this to dilate |
|
|
Ipratropium, tiotropium |
Asthma and COPID (inhalation)- no CNS entry, *no change in mucus viscosity, just less secretion |
|
|
Scopolamine |
use in motion sickness -causes sedation and short-term memory block |
|
|
Benztropine, trihexyphenidyl |
Lipid-soluable (CNS) - used to treat parkinsonism and acute pyramidal symptoms induced by anti-psychotics |
|
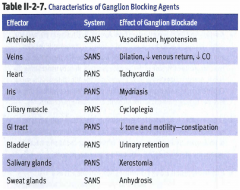
Ganglionic blocking agents |
Hexamethonium and mecamylamine -reduce predominant autonomic tone -prevent baroreceptor reflex |
|
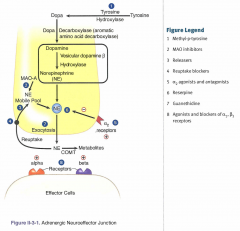
Adrenergic pharmacology
|

Q - a1 I-a2 S-b1 S-b2 |
|
|
Phenylephrine |
A1 agonist- increase MAP and vasoconstrict -increase BP so may have reflex bradycardia Rx- nasal decongestant and ophthalmologic use (mydrasis without cycloplegia) |
|
|
Clonidine, methyldopa |
A2 angonist -Decrease sympathetic outflow by stimulating Rx- mild to moderate HTN |
|
|
Isoproterenol |
non-selective b agonist Rx- B1- heart block, bradyarrhythmias B2- bronchospasm S/e- flushing (B2), angina (B1), arrhythmias (B1) |
|
|
Dobutamine |
B1 > B2
|
|
|
Selective B2 agonists |
salmeterol, albuterol, terbutaline used in asthma Terbutaline used in premature labor |
|
|
Norepinephrine A1, A2, B1 |
A1: ^TPR, ^BP B1: ^ HR, ^ SV, ^ CO -increase pulse pressure -potential reflex brady -does not affect B2 *NE CAN NEVER LOWER BP |
|
|
Epinephrine A1, A2, B1, B2 |
B1: ^HR, ^SV, ^ Co, ^PP B2: decrease TPR, Decrease BP A1: ^ TPR, ^ BP At low dose B2 > A1 At high dose A1 > B2 At high dose, potential reflex brady |
|
|
Way to tell difference btwn Norepinephrine and epinephrine |
Check for B2 specific characterstics -smooth muscle relaxation (bronchioles, uterus, blood vessles) -metabolic- glycogenolysis, gluconeogenesis, mobilization and use of fat At high dose epinephrine, Block A1 (administer A1 antagonist) -if pt becomes severely hypotensive, it was due to high dose epinephrine, not norepinephrine |
|
|
Use of norepinephrine and epinephrine |
1. cardiac arrest 2. adjunct to local anesthetic (keep it localized) 3. hypotension (A1 and B1) 4. anaphylaxis -epinephrine only- B2 due to bronchospasm -use high dose, or pt will become hypotensive even more 5. asthma- epinephrine only |
|
|
Norepinephrine Releasers- displace norepinephrine from mobile pool |
Watch out for drug interactions -MAO-inhibitors inhibit MAO-A in gut -this increases tyramine bioavailability and causes hypertensive crisis -same with Amphetamines and ephedrine + pseudepherine |
|
|
Norepinephrine Reuptake inhibitors |
cocaine and tricyclic antidepressant -causes catecholamine (norepi/epi) buildup, can cause ischemia |
|
|
Alpha antagonist |
-decrease TPR and mean BP -may cause reflex tachy and salt/water retention Rx- HTN, pheochomocytoma, BPH Phentolamine, competitive Phenoxybenzamine, noncompetitive |
|
|
Phentolamine |
competitive Alpha antagonist, reversible -cant use it for treatment of pheo, epinephrine will outcompete it |
|
|
Phenoxybenzamine |
non-competitive, irreversible non-selective alpha antagonist Rx- pheochromocytoma -must add Beta blocker AFTER phenoxybenzamine |
|
|
Selective alpha 1 blocker |
prazosin, doxazosin, terazosin, tamsulosin Rx- BPH (does not treat the BPH it self, but just treats the urinary retention) |
|
|
selecitve A2 blocker |
mirtazapine- antidepressant -skinny old lady thats depressed -will help her gain weight |
|
Beta receptor antagonist |
B1 blockade -decrease HR, SV, CO (decrease oxygen demand) -decrease renin release -decrease Aqueous humor production B2 blockade -may precipitate bronchospasm -decrease aqueous humor production -metabolic effects- blocks glycogenolysis/gluconeogenesis -increase LDL, TG due to impaired lipolysis |
|
|
Beta blocker- B1 selective - A ~ M -cardioselective |
Acebutolol, atenelol, Metoprolol -less effect on vasculature,bornchioles, uterus, metabolism -safer in asthma, DM, PVD |
|
|
Acebutolol |
B1 blocker -has intrinsic sympathomimetic activity (ISA) meaning its a partial agonist -does not cause increase blood lipid -safer in asthma, diabetes, peripheral vascular diseases |
|
|
Intrinsic sympathomimetic activity |
Acts as partial agonist -less bradycardia -slight vasodilation or bronchodilation -minimal changes in plasma lipids |
|
|
Atenelol |
B1 selective -water soluable = does not enter CNS |
|
|
General use of Beta-blockers |
-angina, HTN, post-MI -Antiarrhythymics (class II: Proranolol, acebutolol, esmolol) -glaucoma- timolol -migrane, thyrotoxicosis, performance anxiety, essential tremor (propanolol) |
|
|
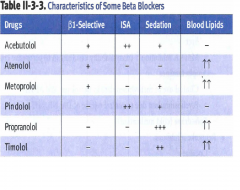
Beta blockers |
B1 selective- Acebutolol, atenolol, metoprolol Non-selective- Pindolol, propranolol, timolol ISA + - Acebutolol, pindolol Sedation- Propanolol, timolol Does not raise blood lipid - Acebutolol, pindolol |
|
|
Beta blocker watch contraindications/s/e |
-avoid in asthmatic, vasospatic disorder, diabetics -may cause prinzmetal angina or Raynauds (treat with CCB) -masks hypoglycemic events in diabetics -treat betablocker toxicity with glucagon (Gs protein = increase cAMP) -must wean off, tapering it due to chronic use leading to upregulation of receptors |
|
|
Propranolol |
nonselective betablocker Rx- migraine, thyrotoxicosis, performance anxiety, essential tremor thyrotoxicosis- inhibits deiodinase (T4 -> T3) in the blood |
|
|
Labetalol and carvedilol |
combined alpha -1 and beta blocking -use in CHF (carvedilol) and in htn emergencies (labetalol) |
|
|
Sotalol |
K+ channel blockade and B-blocking activity |
|
|
Open-angle glaucoma |
Cholinomimetic- Pilocarpine, echothiophate -contracts ciliary muscle = increase out flow through canal of Schlemm Echothiphate is an organophosphate - AChE inhibitor -> increase outflow Betablocker- Timolol -blocks NE action -> decrease aqueous humor |
|
|
Close angle glaucoma |
give cholinomimetics (pilocarpine, echothiphate), carbonic anhydrase inhibitors (acetazolamide), mannitol contraindicated-antimuscarinic drugs and a1 agonist |