Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
17 Cards in this Set
- Front
- Back
|
Neuromuscular Physiology
|
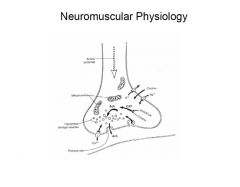
Neuromuscular Physiology
|
|
|
Atropine and Cocaine
|
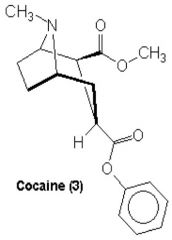
Atropine and Cocaine (Do I need to know the structures by heart?)
|
|
|
Phenylephrine
|
Synthetic non-catecholamine
Primarily alpha1-adrenergic receptor stimulant Mostly direct acting Venoconstriction>arterial constriction Less potent than norepi Longer lasting |
|
|
Phenylephrine Basics
|
Dose: 50-200 microgms IV, can be used as continuous infusion (20-50 microgms/min)
Treat hypotension in OR due to various reasons Increases MAP, SBP, DBP, SVR Decreases HR, CO Not used in OB anesthesia Double dilution/or in 100mL |
|
|
Ephedrine Basics
|
Synthetic non-catecholamine
Indirect acting-stimulates alpha and beta adrenergic receptors Dosage: 5-25mg IV Treat hypotension in OR due to various reasons Can be used in OB anesthesia |
|
|
Ephedrine Continued
|
CV effects similar to epinephrine, longer lasting (10X)
SVR effected minimally CV effects mostly due to an Increase in contractility Increased MAP, SBP, DBP, HR, Coronary BF Decreased renal, splanchnic BF Tachyphylaxis is common with this agent-due to indirect effect and occupying of receptors Dilute once |
|
|
Atropine
|
Anticholinergic-antagonizes effect of Ach at cholinergic post ganglionic muscarinic receptors.
Muscarinics are present in: Heart, salivary glands, smooth muscles of GU and GI tract. No/minimal effect at nicotinic receptors. |
|
|
Atropine Continued
|
Tertiary amine-naturally occurring, is an alkaloid of belladonna plant.
Resembles cocaine in structure, and has mild analgesic activity. Combines reversibly with muscarinic receptors and prevents Ach from binding to these sites, competitive inhibitors. |
|
|
Atropine Targets Which Receptors?
|
Muscarinic receptor subtypes:
M1-CNS & Stomach M2-lungs and heart M3-CNS, airway smooth muscles, glandular tissue M4 & M5-CNS |
|
|
Atropine Basics
|
Drug of choice for treating intra op bradycardia.
Dose: 15-75 microgms/kg IV. Other effects: antisialagogue, bronchodilation, mydriasis, GI motility and acid production, bronchodilation, sedation. |
|
|
Glycopyrrolate
|
Similar to atropine.
Quaternary ammonium-does not easily cross BBB so no sedative effects. Uses similar to atropine, similar effects, more potent antisialagogue, less potent at HR. Dosage: .2-.4mg IV Combine with anticholinestrases for reversal, .005-.007mg/kg (or 1cc of robinul for each cc of reversal drawn) |
|
|
Lidocaine
|
Amide local anesthetic
Prevents transmission of nerve impulses by inhibiting passage of sodium ions through ion selective sodium channels in nerve membranes. Slows the rate of depolarization such that the threshold potential is not reached and an action potential is not propagated. |
|
|
Lidocaine Continued
|
Used for local anesthetic activity, numbness of veins for propofol (about 30mg), and ablating response to laryngoscopy (1mg/kg).
Used as an antidysrhythmic-suppresses ventricular dysrhythmias, especially PVCs, and Vtach-2mg/kg IV followed by infusion of 1-4mg/min In heart delays the rate of spontaneous phase 4 depolarization by preventing the gradual decrease in K+ ion permeability. OD causes CNS toxicity/seizures. |
|
|
Succinylcholine
|
Depolarizing muscle relaxant
SCh attaches to each of alpha subunits of the nicotinic cholinergic receptor and mimics the action of ACh, depolarizing the post-junctional membrane. Hydrolysis of SCh is slower than ACh resulting in sustained depolarization of the receptor ion channels. |
|
|
Succinylcholine Basics
|
Dose: 0.5-1mg/kg
Duration of action: 3-5minutes Used for emergency a/w situations, rapid sequence induction. Can cause: dysrhythmias (bradycardia, arrest-acts at cardiac muscarinic receptors mimics ACh), hyperkalemia, myalgias, Increased GI pressure, ICP, and IOP. |
|
|
Labetalol
|
Non selective beta blocker as well as alpha blockade.
Beta:Alpha in a ratio of 7:1. Usual IV dose is 0.25 mg/kg. Can repeat q 10 mins. Bolus of 10mg-typical Duration of action of 2-18hrs Make sure pt has adequate HR, do not give to asthmatics. |
|
|
Esmolol
|
Beta-1 selective agent at small doses.
Onset of 2 minutes. E1/2 life of 9 minutes-metabolized by non-specific plasma esterases found in the cytosol of RBCs. Bolus dose of 500ug/kg (IV loading dose) In OR we typically use 10-15mg, and then dose according to response. |