Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
What compensatory mechanisms arise in the face of anemia
|

Shift curve to right, HGB release oxygen more readily in tissue
Increase cardiac output Shunt blood to vital organs Increase breathing rate Stimulate increased EPO within peritubular cells in kidney which are stimulated in case of hypoxia Compensated increased plasma so that blood volume is normal. |
|
|
What are the clinical manifestations of anemia?
|
Weak
Fatigue Headache Inability to concentrate Decreased exercise tolerance Hypovolemia if acute Chronic anemia is better tolerated than acute anemia May have some neurologic symptoms: dizziness, fainting, weakness Skin and mucous membrane pallor |
|
|
At what degree of HGB do we begin to see symptoms of anemia?
|
"Not how low you go but how fast you go down"
HGB > 10 g/dl - MILD ANEMIA HGB BTW 7 & 10 - MODERATE (Tachycardia, short of breath) HGB < 7 g/gl - SEVERE ANEMIA- angina, dizzy, fainting, weakness |
|
|
Classification of anemia is done in two basic ways:
|
Pathophysiologic mechanism
& Morphology on blood smear. CBC |
|
|
4 main pathophysiologic reasons that one may have anemia
|
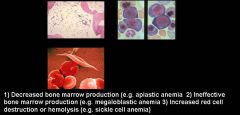
Decreased RBC production
Ineffective production - don't get released to circulation Increased destruction of RBC in periphery Increased blood loss |
|
|
When classifying anemia, when would you see increase reticulocytosis and when would you see a decrease?
|
If have anemia due to decreased production of RBC's --> have inappropriately low reticul count
If have hemolysis -> body responds with increased percentage of reticulocytes, polychromasia |
|
|
Name some of the causes of decreased RBC production in bone marrow that could lead to anemia
|
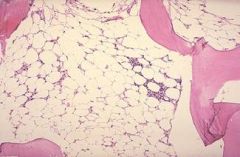
Aplastic anemia - failure of multipotent stem cells
Iron deficiency Chronic inflammatory and infectious disorders Bone marrow infiltration by a neoplastic or infectious process *** HAVE INAPROPRIATE RETICULOCYTE PRODUCTION *** underlying malignancies |
|
|
List some causes of anemia due to increased or premature destruction of RBC's
|
Hemolytic anemia - intravascular or extravascular
Red cell membrane or cytoskeleton - hereditary spherocytosis, hereditary elliptocytosis Autoantibodies Mechanical destruction Hypersplenism - sequester RBC's |
|
|
list three situations where one may have anemia due to the ineffective production of RBC's:
|
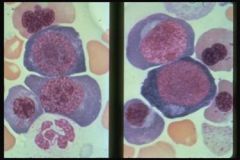
Vitamin B12 or folic acid deficiency
Impaired DNA synthesis Myelodysplastic stem cells |
|
|
Anemia of chronic disease
Acute blood loss Renal disease |
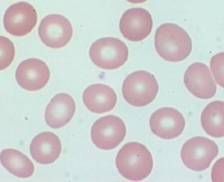
List conditions associated with normocytic red blood cells:
|
|
|
Iron deficiency
Thalassemias Anemia of chronic disease Hemoglobinopathies - HGBpathy E Lead poisoning Sideroblastic anemias - due to stem cell defects |
What anemic conditions are associated with microcytic anemia?
|
|
|
What conditions are associated with macrocytic anemia?
|
Megaloblastic anemia
Hemolytic anemias - have increased size of reticulocytes Liver disease Alchohol disease Hypothyroidsm Stem cell disorders - aplastic anemia, myelodysplasia |
|
|
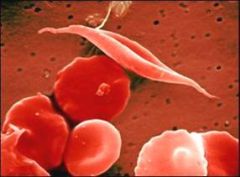
What anemic conditions are associated with hyperchromatic RBC's?
|
Sickle cells
Acanthocytes - membrane defect Spherocytes |
|
|
Abnormal RBC's are known as:
|
Poiklocytes
|
|
|
What conditions are the following cells associated with?
spherocytes |
Hereditary Spherocytosis
Immune hemolytic anemia |
|
|
What conditions are the following cells associated with?
Elliptocytes or ovalocytes |
Hereditary elliptocytosis
|
|
|
What conditions are the following cells associated with?
Target cells |
Thalassemias, hemoglobinopathies,
liver disease |
|
|
What conditions are the following cells associated with?
acanthocytes |
Liver disease
abetaliproteinemia |
|
|
Two of the most common red cell inclusions are
|
Howell-Jolly bodies: nuclear remnants seen with hyposplenims - seen in sicklecell patients
Basophilic stippling (thalassemia, lead poisoning) |