![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
250 Cards in this Set
- Front
- Back
|
What does the Spinal Canal hold? |
The spinal cord |
|
|
What 3 things does the intervertebral foramina enclose |
1. Dorsal root ganglia 2. Mixed spinal nerves 3. Blood vessels |
|
|
How does the vertebral column structure differ in the foetus and an adult?
|
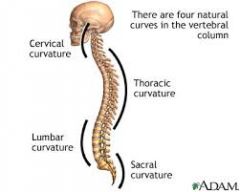
- Starts off as a C shape in foetus
- Secondary 'lordotic curves' develop in cervical and lumbar regions => Allows upright posture & horizontal sight |
|
|
What are the 3 abnormal curvatures that can occur to the vertebral column? |
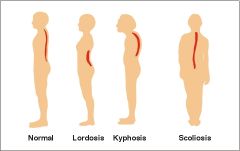
1. Abnormal lordosis
- Protruding lumbar (gut) 2. Kyphosis - Increased thoracic curvature (hunched) 3. Scoliosis - Lateral deviation of spine from midline |
|
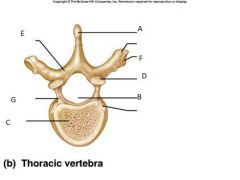
Label this Lumbar Vertebra |
A. Spinous process B. Vertebral foramen C. Vertebra body D. Superior articular process E. Lamina F. Costal Facet G. Transverse process |
|
|
What are the 2 properties of the vertebral body? |
1. Weight bearing
2. Have articular surfaces on top & bottom |
|
|
What 2 components make the vertebral arch and what is its function?
|
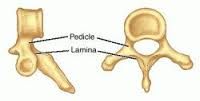
Made from pedicles + lamina
=> forms the vertebral foramen/canal allowing protected passage of spinal cord |
|
|
What is the function of the spinous and transverse processes?
|
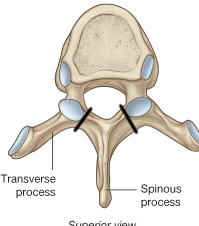
Provide sights for muscle attachment which allow movement of the back
|
|
|
What is the function of the articular processes?
|
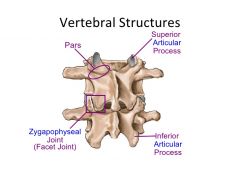
Superior articular processes + Inferior articular process = Zygophasageal / Facet Joint
=> Allows movement between joints |
|
|
Name 5 regional characteristics of vertebra
|
1. Progressive increase in vertebral body size further down (progressively higher weight load) until sacrum which tapers (low weight bearing)
2. Cervical vertebra form a 'foramen transversarium' due to element fusion which allows for vertebral artery/vein passage 3. Thoracic vertebra have ribs fused on tom them 4. Sacrum and coccyx are both fused 5. Articular processes orientated in different directions, as to allow zygophasageal joint movement in different planes (e.g. thoracic processes are orientated in coronal plane to allow rotation and lumbar processes are orientated in the saggital plane to allow flexion/extension) |
|
|
What is the 'cauda equina' and where does it start? |
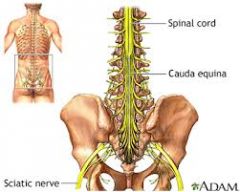
The cauda equina is a horsetail shaped collection of spinal nerve roots which extend to the lower body.
It starts where the spinal cord ends - roughly L1 / L2. |
|
|
Why are the intevertebral and vertebral foramen larger in the cervical region and smaller in lower regions? |
Superior vertebra must surround all the nerves whereas the inferior vertebra must surround only a portion of the spinal nerves. |
|
|
How are the spinal nerves named? |
From C1 - C7 vertebra, each vertebra has a spinal nerve above. C7 vertebra has 2 spinal nerves, one above and one below respectively named the C7 & C8 spinal nerves. From C7 vertebra onwards, all the vertebra have 1 spinal below. |
|
|
Where do the afferent/efferent nerves of the anterior rammus lead to? |
The upper & lower limbs + the trunk |
|
|
Where do the afferent/efferent nerves of the posterior rammus lead to? |
The back muscle |
|
|
What is the difference of function in the ventral and dorsal spinal roots? |
Dorsal = afferent = sensory Ventral = efferent = motor |
|
|
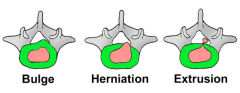
Describe the structure of the intervertebral disc |
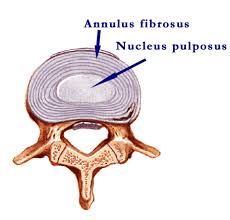
1. Nucleus pulposus (centre) 2. Anulus fibrosis (covering) |
|
|
How does the structure of the nucleus pulposus relate to its function? |
- The nucleus pulposus is comprised of a gel-like substance with loose fibres that is high in water content - This allows it to serve a shock absorbing function - It can be laterally deformed but resists downwards compression |
|
|
|
- Annulus fibrosus is composed of concentric fibrous lamellae, orientated in alternating directions - Allows twisting of vertebra without tearing and excessive movement |
|
|
What are the 4 types of vertebral column ligaments? |
1. Longitudinal Ligaments (posterior +anterior) 2. Interspinous Ligaments 3. Supraspinous Ligaments 4. Ligamenta Flava |
|
|
What are longitudinal ligaments? |
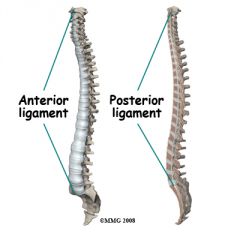
Ligaments that run down the front and back surfaces of the spine. There is an anterior longitudinal ligament and a sheet of posterior longitudinal ligament. |
|
|
What are zygophasageal (facet) joints? |
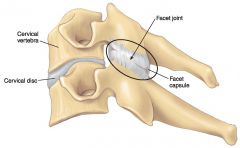
- Plane synovial joints formed by the inferior articular process of a vertebra and the superior articular process of the vertebra below. - Allows gliding along a single axis (movements dependent on articular surface shape, depth and orientation) - Surrounded by synovial membrane + capsule |
|
|
What are Interspinous Ligaments? |
Sheets of ligament that run between the spinous processes of vertebra |
|
|
What are supraspinous ligaments? |
Sheets of ligament that run over the top of spinous processes |
|
|
What are Ligamenta Flava? |
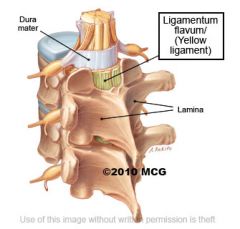
Non-continuous sheets of ligaments that attach lamina of adjacent vertebra. They are high in elastic fibre content (yellow colour) to allow stretch. |
|
|
What are the 2 main groups of deep (intrinsic) back muscle? What general function do they serve?
|
All attach to and act on the back
1. Erector Spinae 2. Transversospinalis |
|
|
What is the function of the erector spinae muscles? |
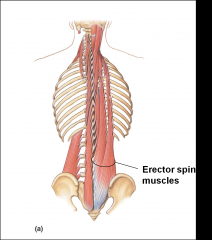
- Act as prime movers
1. Concentric contraction = Upright posture 2. Eccentric contraction = Flexion of back |
|
|
What is the function of the transversospinalis muscles? What are some distinguishing factor of transversospinalis muscles? |

- Serve as stabilizing muscles (i.e. prevent excess movement of back)
- They are short muscles that typically span 2-3 vertebra - They can atrophy quickly following injurt and lack of use |
|
|
What are the 3 functions of lumbar fascia?
|
1. Provide sites of attachment for erector spinae and the extrinsic back muscles (e.g. trapezius) 2. Forms a tight compartment for intrinsic back muscles, enhancing their action 3. Being continuous with the abdominal muscles, tightening of abs tightens the fuscia and allows stretching of the intrinsic back muscles |
|
|
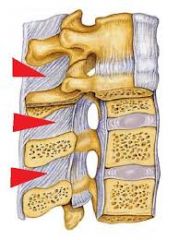
What are the 3 types of vertebral disc injuries? |
|
|
|
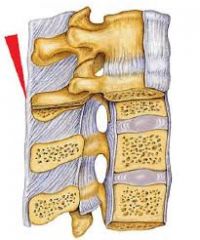
How does vertebral joint degeneration occur? What effect can it have? |
- Joint degeneration occurs when articular cartilage thins + vertebral bony outgrowths (ostephytes) form - Decreases joint mobility - Osteophytes encroach on spinal canal / intervertebral foramen - Can cause severe pain if there is impingement on spinal nerves |
|
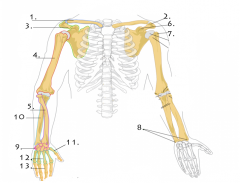
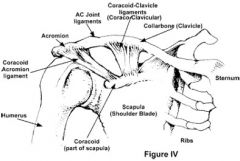
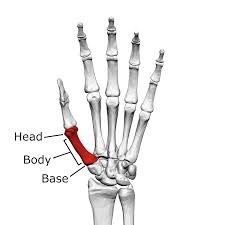
What bone is no. 1? What type of bone is it? What function does it serve? |
The clavicle
- Long bone - Serves to connect sternum and scapula - Pushes the upper limb to the side, allowing a full range of arm motion |
|
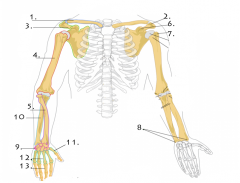
What structure is at 2? |
The acromion process
|
|
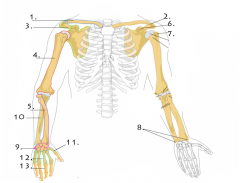
What bone is no. 3?
What type of bone is it? |
The Scapula
- Flat bone |
|
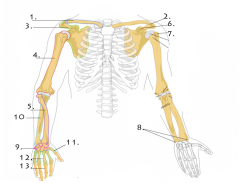
What bone is no. 4?
|
The humerus
|
|
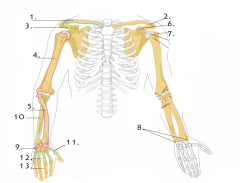
What bone is no. 5? |
The radius
|
|
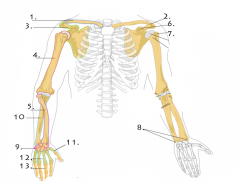
What bone structure is at 6? |
The coracoid process |
|
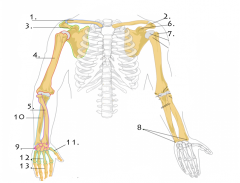
What bone structure is at 7? What are its 2 sections? |
The head of humerus - Subdivided in to anatomical neck (proximal) and surgical neck (distal) |
|
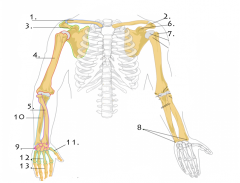
What bone structure(s) does 8 refer to? |
The styloid processes of the radius and ulna
|
|
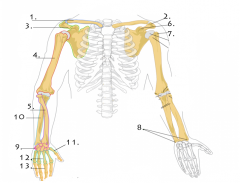
What are the bones at 9?
|
The carpals
|
|
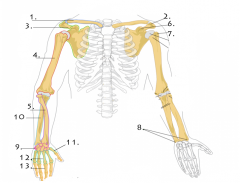
What is the bone at 10? |
The ulna
|
|
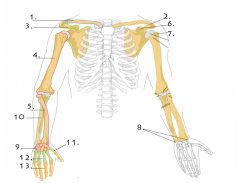
What is the bone at 11? |
The 1st metacarpal |
|
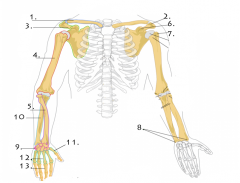
What are the bones at 12? |
The 2nd - 5th metacarpals
|
|
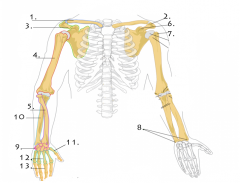
What are the bones at 13? |
The Phalanges |
|
|
What is the glenoid fossa and where is it found? |
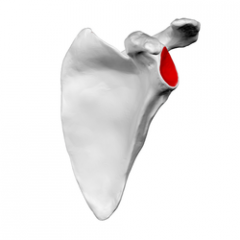
Articular depression of scapula. - allows head of humerus to attach to scapula - lined by deep labrum |
|
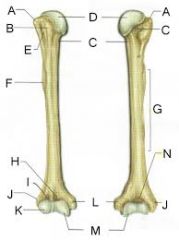
What are structures A & B? What are their purpose? |
A - greater tuberosity of humerus
B - lesser tuberosity of humerus They serve as muscle attachment sites, allowing for movement of the humerus |
|
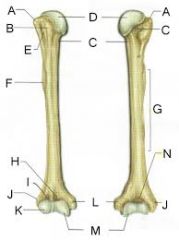
What is structure E? What is its purpose? |
E - Bicipital groove Allows passage of biceps brachii |
|
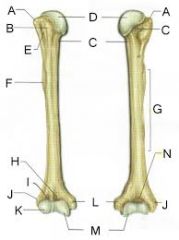
What does the region G refer to? |
The shaft of humerus
|
|
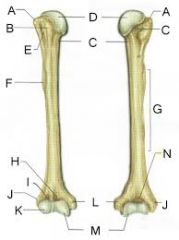
What are structures L & J? What are their functions? |
L - Medial Epicondyle
J - Lateral Epicondyle Serve as sites for muscle attachment |
|
|
What bone structure does the ulnar nerve run behind at the elbow joint? |

The medial epicondyle |
|
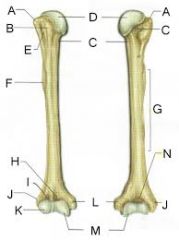
What structure is at M? What is its purpose? |
The Trochlea of humerus
- fits in to trochlear notch of ulna to form main articular surface of elbow joint |
|
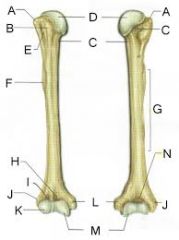
What structure is at K? What is its purpose? |
The Capitulum - Allows radial head to glide over (minor articulation in the elbow joint) |
|
|
What 3 structures/regions of the humerus are most susceptible to fracture? |
1. Surgical Neck 2. Midshaft 3. Supracondylar region |
|
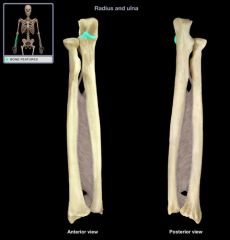
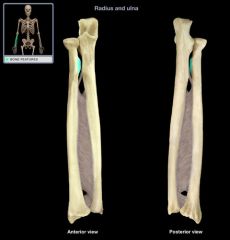
What structure is highlighted? What is its purpose? |
The Coronoid Process |
|

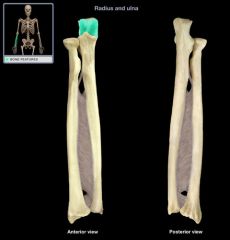
What structure is highlighted? |
The head and 'fovea' of radius |
|

What bone structure is left unlabeled? |
The olecranon process of ulna
|
|
What bone structure is highlighted? What is its purpose? |
The Radial Tuberosity => insertion of biceps |
|

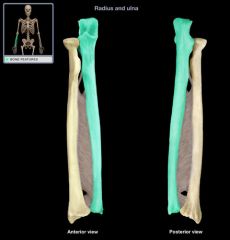
What bone is highlighted? |
The Radius
|
|

What bone structure is highlighted? |
The styloid process of radius |
|
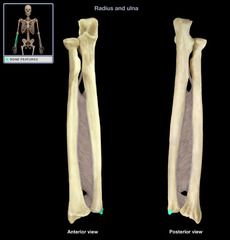
What bone structure is highlighted? |
The styloid process of ulna |
|
What bone structure is highlighted? |
The Trochlea Notch
|
|
What bone is highlighted? |
The Ulna
|
|
|
What is the interosseous membrane and its function? |

Sheet of connective tissue between the radius and ulna (forearm) or the fibula and tibia (leg).
- Increases surface area for muscle attachment - Forms a fibrous syndesmosis joint between the two bones - Directs force between radius & ulna |
|
|
What are the 4 features of the sternoclavicular joint? |

1. Saddle type synovial joint
2. Has intra-articular disc which allows increased stability and movement 3. Has a very strong synovial capsule 4. Reinforced by strong costoclavicular ligament |
|
|
What are the 3 features of the acromioclavicular joint? |
1. Plane type synovial joint 2. Has a weak capsule 3. Stabilised mainly by coracoclavicular ligament (conoid + trapezoid ligaments) |
|
|
What is the general principle that relates joint mobility and joint stability? |
More stable joints tend to be less mobile, and vice versa. |
|
|
What is the glenoid labrum? |
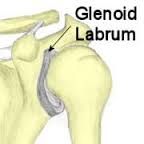
A fibrocartilaginous rim that is attached to the margin of the glenoid cavity, deepening the shoulder socket |
|
|
What 3 forms of support does the glenohumeral joint have? |
1. Coroacromial ligament => above fossa 2. Long head of biceps => in front of fossa 3. Rotator cuff muscles => all around (except underneath) pulling humerus in to glenoid cavity |
|
|
What are the 2 ways the shoulder can become dislocated? Which is more common? |
1. Anteriorly
=> When force is applied to abducted and externally rotated arm 2. Posteriorly => When falling on outstretched arm Anterior dislocation is more common |
|
|
What is the scapulo-thoracic joint and what function does it serve? |

Articulation between scapula & rib cage (physiological joint, not true joint) - Allows scapulo-humeral rhythm => abduction/adduction & rotational movement of humerus |
|
|
What is the radial notch, and what is the ulnar notch? |
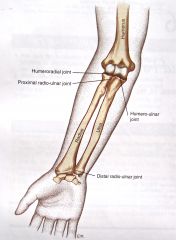
Radial notch - articular depression on the coronoid process of the ulna that houses part of the radius head, forming the proximal radioulnar joint
Ulnar notch - articular depression on the distal side of the radius that houses part of the ulnar head, forming the distal radioulnar joint |
|
|
What 3 joints are in the elbow joint capsule? |
1. Humeroulnar Joint
2. Humeroradial Joint 3. Proximal Radioulnar Joint |
|
|
What type of joint is the elbow joint? |
Hinge type synovial joint
(reinforced by strong ligaments) |
|
|
What type of joint are the proximal & distal radioulnar joint? What movements can occur at these joint? |
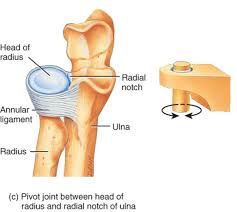
Pivot type synovial joint => pronation & supination Proximal and distal linked via interosseous membrane and function as a single joint |
|
|
What is the anular ligament? |

Ligament that attaches to ulna and forms a ring around the head of radius, binding it close and forming the proximal radioulnar joint |
|
|
What bones form the wrist joint? What is between these bones? What type of joint is it? |
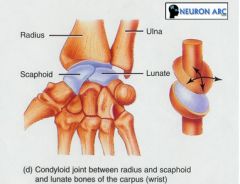
- The radius and scaphoid + lunate (no ulnar articulation) - Articular disc found between these bones - Condyloid synovial joint |
|
|
How many carpal bones are there? How many metacarpal bones are there? |
8 Carpal Bones 5 Carpal Bones |
|
|
Where is the midcarpal joint located? |
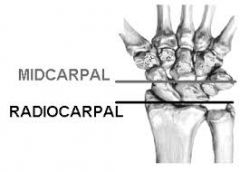
Between the proximal and distal rows of carpal bones
|
|
|
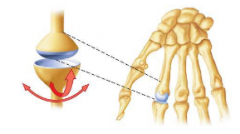
What type of joint is the 1st carpometacarpal joint? |

Saddle type synovial joint
|
|
|
What type of joint are the 2nd to 5th carpometacarpal joints? |
Plane type synovial joint
|
|
|
What type of joint is the first metacarpophalangeal joint? What movements does it allow? |
Hinge type synovial joint => Flex/Ext |
|
|
What type of joint are the 2nd to 5th metacarpophalangeal joints? What movements do they allow? |
Condyloid type synovial joint => Flex/Ext + Abb/Add |
|
|
What type of joints are the interphalangeal joints? What movements do they allow? |
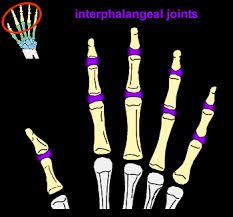
Hinge joint
=> Flex/Ext |
|
|
What planes (i.e. transverse, sagital, coronal or mixed) do the following shoulder movements occur in? 1. Retraction/Protraction 2. Flexion/Extension 3. Abduction/Adduction 4. Medial/Lateral Rotation 5. Circumduction |
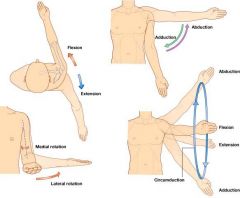
1. Transverse
2. Saggital 3. Coronal 4. Transverse 5. Both Transverse and Saggital |
|

What is the following forearm movement? |
Pronation
|
|
|
What 3 movements can occur at the wrist joint and what plane do they occur in? |
1. Flexion/Extension (Saggital)
2. Abduction/Adductoin (Coronal) 3. Circumduction |
|
|
Where is the brachial fascia found?
|
In the arm |
|
|
Where is the antebrachial fascia found? |
In the forearm |
|
|
What are 4 examples of fascia found in the upper limb? What are their general functions? |
1. Interosseous Membrane => Binds radius and ulna 2. Retinaculae => Binds down tendons (prevents bow stringing) => Protects nerves & vessels 3. Flexor Retinaculum => Forms carpal tunnel roof => Holds median nerve 4. Aponeurosis => Serves similar function to tendon 5. Digital Sheaths => Reduce friction between hand tendons and surrounding structures |
|
|
What are the 4 shoulder girdle muscles? What are their main function, respectively? |
1. Pectoralis Major => Flexion of shoulder 2. Pectoralis Minor => Pulls scapula anteriorly and inferiorly 3. Seratus Anterior => Originates from ribs and inserts of nedial border of scapula => Keeps scapula against thoracic cage 4. Deltoid => Coronal abduction of arm => Shoulder rotation |
|
|
What are the 3 divisions of arteries in the arm? |
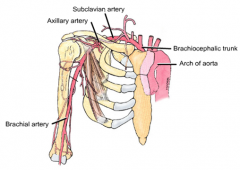
1. Subclavian artery 2. Axillary artery 3. Brachial artery |
|
|
Where does the subclavian artery lie and what does it supply and connect? |
- Lies under the clavicle - Supplies blood to the arm - Connects the aortic arch and the axillary artery |
|
|
Where does the axillary artery lie and what does it supply and connect? |
- Lies in the axilla (armpit) region - Supplies blood to the axilla - Connects the subclavian artery and brachial artery |
|
|
Where would you find the brachial artery? What does it supply and connect? What is its significance in clinical practice? |
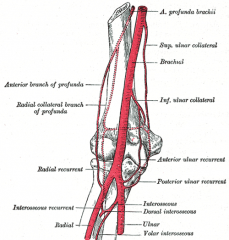
- Found along the ventro-medial aspect of the arm, tucked behind the biceps brachii - Supplies the biceps and triceps - Connects the artery to the radial and ulnar arteries - It is often occluded to take BP readings |
|
|
Which artery is the principal supplier of the forearm and hand? |
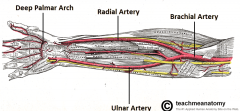
The ulnar artery (radial artery supplies some lateral aspects of forearm) |
|
|
Where do the arteries of the forehand terminate? |
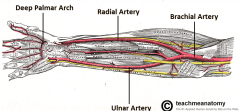
The palmer arterial arch where they then extend as digital arteries |
|
|
Which artery is palpable at the wrist (antero-medially)? |
The ulnar artery |
|
|
How do the ulnar and radial artery pass from the forearm to the hand? |
They pass over the flexor retinaculum (not inside carpal tunnel) |
|
|
What artery passes through the 'snuffbox'? |
The posterior branch of the radial artery |
|
|
What are 'end arteries' and in what regions of the body can you find them? What are their clinical significance? |
End arteries are arteries which terminate and are the sole supplier of blood to a region. They can be found at the finger tips, nose, and penis As they are the only supplier of blood to a body part, occlusion or vasoconstriction due to drug use can lead to necrosis in that region. |
|
|
What are Volkmann's Ischaemic Contractures caused by? What happens as a result? |

They are caused by a supra condylar fracture which damages the surrounding elbow arteries Causes a permanent tightening of forearm muscles due to avascular necrosis leading to a claw like deformity |
|
|
What complications can result from a fractured scaphoid? |

The scaphoid bone is supplied by the radial artery which has a distal to proximal blood supply. Fracturing leads to avascular necrosis of that region (proximal fractures cause the most damage) |
|
|
What are the 3 superficial veins of the upper limb and how are they arranged? |
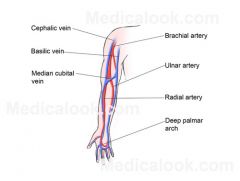
All superficial veins start on the dorsal (back) side of the hand 1. Cephalic Vein - Runs along the radial end of arm 2. Basilic Vein - Runs along the ulnar end of arm 3. Median Cubital Vein - Connects the cephalic and basilic veins (commonly used as a point of blood extraction) |
|
|
How are the superficial veins of the upper limb typically linked to the deep veins? |
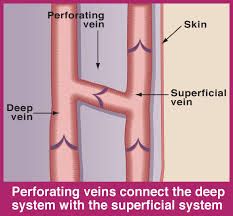
Linked via perforating veins - Use musculovenous pump & valves to ensure unidirectional flow |
|
|
1. Where do the lymphatics of the upper limb originate? 2. What lymph node do they pass? 3. Where do they drain? |
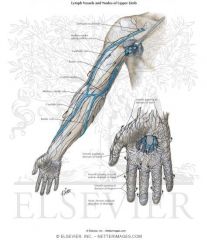
1. Starts in the 'lymphatic plexi' in the hands 2. Follows superficial veins to the axillary lymph nodes 3. Drain via lymphatic trunks in the neck either to the right lymphatic duct (right UL) or the thoracic duct (left UL) |
|
|
What rammi do the brachial plexus nerves arise from? |
The anterior rammi
|
|
|
Which spinal nerves form the brachial plexus? |
C5 - T1
|
|
|
What are the 3 trunks of the brachial plexus and what spinal nerves are in each? |
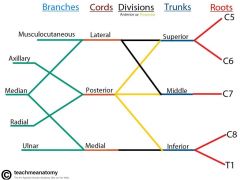
1. Superior
- C5 & C6 2. Middle - C7 3. Inferior - C8 & T1 |
|
|
What divisions do the 3 cords of the brachial plexus come from? What are the cords named according to? |
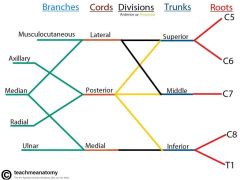
The cords are all named according to their positional relationship with the brachial artery 1. Lateral Cord- Anterior divisions of the superior and middle trunks 2. Posterior Cord - Posterior division of all trunks 3. Medial Cord - Anterior division of inferior trunk |
|
|
What are the 5 terminal nerves of the brachial plexus? |
1. Musculocutaneous nerve
2. Median nerve 3. Radial nerve 4. Axillary nerve 5. Ulnar nerve |
|
|
What terminal nerves do the following cords give rise to? 1. Lateral cord 2. Posterior cord 3. Medial cord |
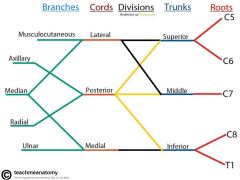
1. Musculocutaneous nerve + median nerve 2. Radial nerve + axillary nerve 3. Ulnar nerve + medial nerve |
|
|
List the following for the musculocutaneous nerve: 1. Spinal nerve origin 2. Muscle innervation 3. Skin innervation |
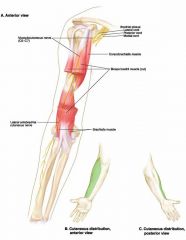
1. C5 - C7 2. Innervates muscles of anterior arm 3. Innervates skin of lateral forearm |
|
|
List the following for the median nerve: 1. Spinal nerve origin 2. Muscle innervation 3. Skin innervation 4. Injuries |

1. C5 - T1 2. Innervates muscles of anterior forearm + thumb 3. Innervates skin of palmar 3.5 digits + nail beds 4. Runs through the carpal tunnel so injury can lead to carpal tunnel syndrome |
|
|
List the following for the ulnar nerve: 1. Spinal nerve origin 2. Muscle innervation 3. Skin innervation 4. Injuries |
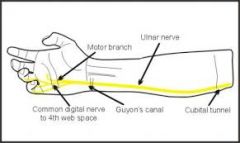
1. C8 - T1 2. Innervates intrinsic muscle of hand (exc. thumb) 3. Innervates skin of medial 1.5 digits of hand (palmar and dorsal) 4. It is reffered to as the 'funny bone' as it is commonly innervated at the medial epicondyle |
|
|
List the following for the axillary nerve: 1. Spinal nerve origin 2. Muscle innervation 3. Skin innervation 4. Injuries |
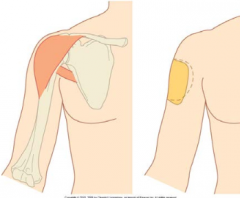
1. C8 - T1 2. Innervates muscles of the shoulder abductors and also the deltiod 3. Innervates skin of the shoulder (military badge region) 4. Can be injured through shoulder dislocation |
|
|
List the following for the radial nerve: 1. Spinal nerve origin 2. Muscle innervation 3. Skin innervation 4. Injuries |
1. C5 - T1 2. Innervates muscle of the posterior arm and forearm 3. Innervates skin of the posterior arm and forearm + part of dorsal hand 4. Runs between lateral and medial triceps => exposed to injury there |
|
|
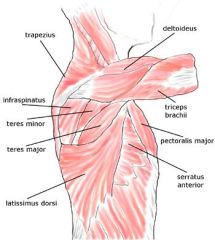
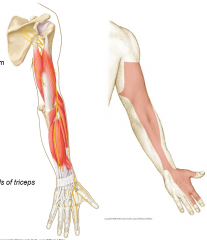
What are the 4 extrinsic back muscles and what are their functions? *Count major and minor as single muscle |
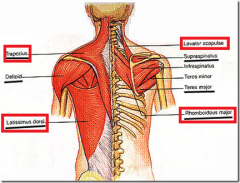
1. Trapezius
- Function depends on which area of trapezius is innervated => Top = scapula elevation => Middle = scapula retraction => Bottom = scapula depression 2. Latissimus Dorsi - Arm extensor 3. Rhomboid Major/Minor - Scapula retraction 4. Levator Scapulae - Scapula elevation |
|
|
What are the 5 shoulder girdle muscles and their functions? *Count major and minor as separate muscles |
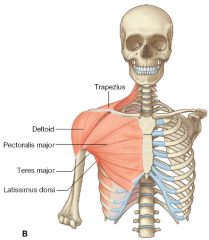
1. Pectoralis Major
- Shoulder flexion 2. Pectoralis Minor - Pulls scapula anteroinferiorly 3. Serratus Anterior - Keeps scapula against thoracic cage (rib origin and medial scapula insertion) 4. Teres Major - Humerus rotator and abductor 5. Deltoid - Arm abduction and shoulder rotation |
|
|
What 2 general functions do scapulo-humeral muscles have? |
1. Fixator function
- Pulls humeral head towards glenoid 2. Prime mover function - Rotation and abduction of arm |
|
|
What are the 4 'rotator cuff' muscles and their functions? |
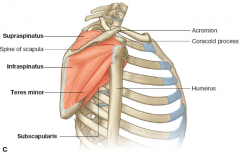
1. Supraspinatus - Humerus abduction 2. Infraspinatus - Humerus external rotation 3. Teres Minor - Humerus external rotation 4. Subscapularis - Humerus internal rotation |
|
|
What general difference in function do the muscles of the anterior and posterior arm serve? |
Anterior
- Flexors Posterior - Extensors |
|
|
What are the 3 muscles of the anterior arm compartment? |
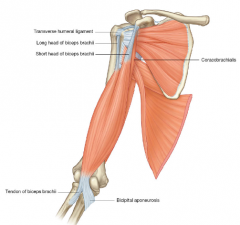
1. Biceps Brachii
2. Brachialis 3. Coracobrachialis |
|
|
What is the function of the biceps brachii? Where is its origin and insertions? |
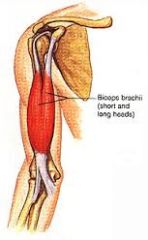
- Arm flexor (prime mover) - Long head origin = supraglenoid tubercle - Short head origin = coracoid process - Insertion inradial tuberosity and bicipital aponeurosis on ulnar |
|
|
What is the function of the brachialis? Where is it located? |
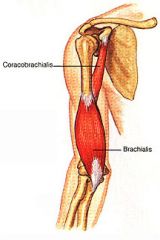
- Arm flexor (synergist of biceps) - Located deep to biceps brachii |
|
|
What is the function of the coracobrachialis? Where is its origin and insertion? |
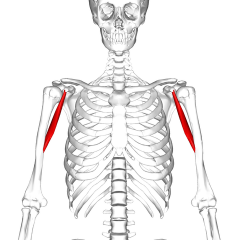
- Arm abduction - Origin = coracoid process - Insertion = body of humerus |
|
|
What is the main muscle in the posterior arm compartment? What is its function? Where are its origins and insertions? |
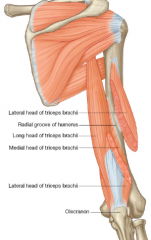
Triceps Brachii
- 3 Heads - Extensor of arm - Long head origin = scapula - Medial and lateral head origin = humerus - Insertion on olecranon process |
|
|
What is the general function of the anterior forearm muscles? |
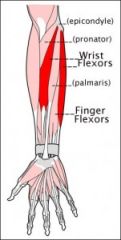
Wrist and finger flexors |
|
|
What is the general function of the posterior forearm muscles?
|
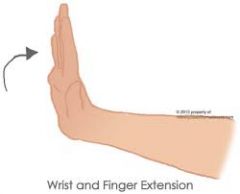
Wrist and finger extensors |
|
|
What are the 3 layers of anterior forearm muscles? Where do they all originate? Do they travel through or over the carpal tunnel?
|
1. Superficial
2. Intermediate 3. Deep Originate on the medial epicondyle of humerus All except PL, PT and PQ travel through the carpal tunnel. |
|
|
What are the 4 muscles in the superficial layer of the anterior forearm? |
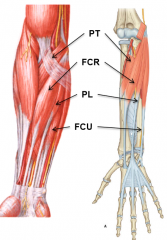
1. Flexor Carpi Radialis (FCR) 2. Flexor Carpi Ulnaris (FCU) 3. Palmaris Longus (PL) 4. Pronator Teres (PT) |
|
|
What is the 1 main muscle in the intermediate layer of the anterior forearm? |
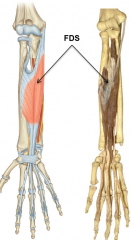
1. Flexor Digitorium Superficialis (FDS) |
|
|
What are the 3 muscles in the deep layer of the anterior forearm? |
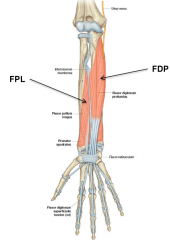
1. Flexor Pollicis Longus (FPL) 2. Flexor Digitorium Profundus (FDP) 3. Pronator Quadratus (PQ) |
|
|
What are the 2 layers of the posterior forearm? From where do the muscles of this compartment originate? |
1. Superficial Layer
2. Deep Layer Originate on the lateral epicondyle of humerus ('common extensor origin' or CEO) |
|
|
What are the 6 muscles in the superficial layer of the posterior forearm? |

1. Extensor Carpi Radialis Longus (ECRL) 2. Extensor Carpi Radialis Brevis (ECRB) 3. Extensor Carpi Ulnaris (ECU) 4. Extensor Digitorum Communis (EDC) 5. Extensor Digiti Minimi (EDM) 6. Brachioradialis (arm flexor at elbow) |
|
|
What are the 5 muscles in the deep layer of the posterior forearm? |

1. Supinator
2. Abductor Pollicis Longus (APL) 3. Extensor Pollicis Brevis (EPB) 4. Extensor Pollicic Longus (EPL) 5. Extensor Indicis (EI) |
|
|
What are 4 groups of intrinsic hand muscles? What is the general function of each group? |
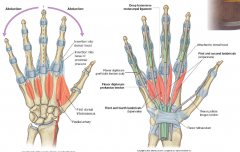
1. Thenar Muscles - Base of thumb movement 2. Hypothenar Muscles - Base of little finger movement 3. Lumbricals - Palm of hand movement 4. Interossei - Back of hand movement |
|
|
Where are the extrinsic hand muscles located? |
They originate in the forearm and only extend in to the hand as tendons
|
|
|
What is a myotome? |
The group of muscles that is innervated by a single spinal nerve root. It is common for a single muscle to be stimulated by more than 1 spinal nerve root (hence each muscle can belong to more than 1 myotome). |
|
|
What 4 movements does C5 allow? |
Snakes Alive, it's C5
1. Shoulder Flexion 2. Abduction 3. External Rotation 5, 6 Pick up sticks 4. Elbow Flexion |
|
|
Which 7 movements does C6 allow? |
Down from heaven 6 & 7
1. Shoulder Extension 2. Adduction 3. Internal Rotation 5, 6 Pick up sticks 4. Elbow Flexion Supine flick, that's C6 5. Forearm Supination Royal Wavin, 6 & 7 6. Wrist Flexion 7. Wrist Extension |
|
|
Which 9 movements does C7 allow? |
Down from heaven 6 & 7 1. Shoulder Extension 2. Adduction 3. Internal Rotation 7, 8 Put 'em in the grate 4. Elbow Extension Pronate, 7,8 5. Forearm Pronation Royal Wavin, 6 & 7 6. Wrist Flexion 7. Wrist Extension Grab it tight, 7 & 8 8. Finger Flexion 9. Finger Extension |
|
|
Which 4 movements does T1 allow? |
Last, have fun with T1 1. Finger Abduction 2. Finger Adduction 3. Thumb Abduction 4. Thumb Adduction |
|
|
What are the 2 sites of brachial plexus injury and their corresponding spinal nerves? What are their respective causes? |
1. Upper Trunk (C5 - C6)
- Forced lateral flexion of head from shoulder 2. Lower Trunk (C8 - T1) - Sudden traction of the upper limb (e.g. falling on outstreched hand) |
|
|
Comparing the upper limb vs. the lower limb, which: 1. Has more mobility? 2. Has more leverage for movement? 3. Is rotated anteriorly in development? 4. Has an angulated bone? 5. Has an opposable digit? |
1. Upper limb is more mobile but less stable 2. Lower limb bones are longer and provide more leverage for movement 3. The upper limb bones are rotated anteriorly during development wheras the lower limb bones are rotated posteriorly 4. The femur in the lower limb is angulated whereas the humerus isn't 5. The thumb is opposable in the upper limb whereas the big toe is non-opposable |
|
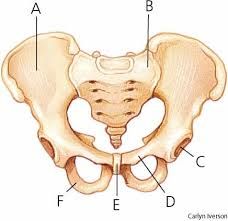
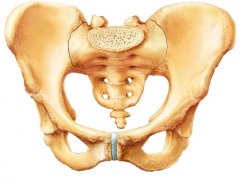
Label the picture |
A. Illium
B. Sacrum C. Coccyx D. Pubis E. Ischium |
|
Point out the Ischial Tuberosities |
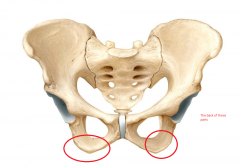
They are the structures you sit on |
|
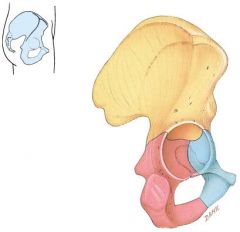
Point out: 1. The illium 2. The pubis 3. The ischium What muscles attach to each? |
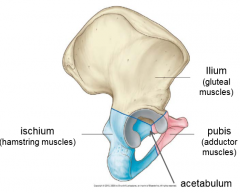
1. Gluteal muscles 2. Hamstring muscles 3. Adductor muscles |
|
|
What 2 features are different between male and female pelvises? |

1. Male pelvises are longer
2. Male pelvises are narrower |
|
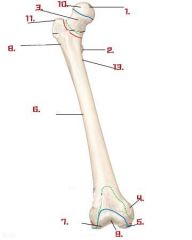
Label the diagram (ignore 8 and 12-13) |
1. Fovea 2. Lesser trochanter 3. Neck of femur 4. Medial epicondyle 5. Medial condyle 6. Body of femur 7. Lateral condyle 9. Intercondylar trochanter 10. Head of femur 11. Greater trochanter |
|
|
Where is the linea aspera found and what is its function? |
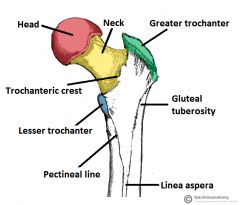
Found on the posterior midline of the femur. Functions as a site of attachment for adductor muscles |
|
Label the acruate bundle and the vertical bundle of trabeculae fibres. What function do they serve together? |
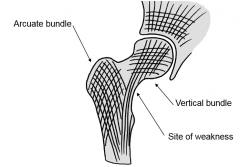
They serve to resist compressive (weight-bearing) forces, and take pressure off the neck of femur which is prone to fracture |
|
|
1. What type of bone is the patella? 2. What function does it serve? |
1. Sesamoid Bone
2. Provides leverage for knee extensor tendons |
|
|
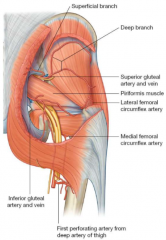
- What 3 muscles are in the anterior pelvic compartment and what is their collective name? - Where are their origins and insertions? - What is their collective function? |
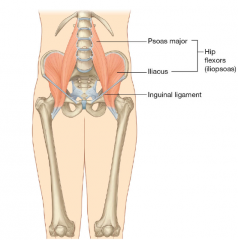
1. Illiacus
- Illiac crest origin 2. Psoas Major - Transverse process origin 3. Psoas Minor - Transverse process origin (higher up) The 3 Muscles form the illiopsoas muscle group => all combine and insert on the lesser trochanta of femur => serve as strong hip flexors |
|
|
- What 3 main muscles are in the posterior pelvic compartment and what is their collective name? - What are their individual functions? |
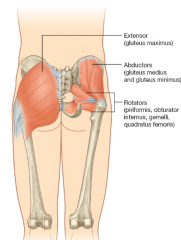
1. Gluteus maximus
- Hip extensor 2. Gluteus medius - Hip abductor 3. Gluteus minimus - Hip abductor |
|
|
What are the 3 fascial compartments of the thigh and what is the generalised function(s) of the muscles in each? |
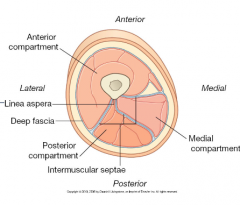
1. Anterior - Knee extensors 2. Medial - Hip adductors 3. Posterior - Hip extensor - Knee flexor |
|
|
- What 5 muscles comprise the anterior thigh compartment? - What is the function of each? |
1. Rectus femoris - Hip flexion 2. Sartorius - Hip flexion 3. Vastus medialis - Knee extensor - Allows normal patella alignment 4. Vastus lateralis - Knee extensor 5. Vastus intermedius - Knee extensor |
|
|
- What 3 muscles comprise the posterior thigh compartment? - What is their collective name? - What is their function? - Where do they originate? - What is a special feature of these muscles? |
1. Semimembranous 2. Semitendonous 3. Biceps femoris Collectively, they are the hamstring muuscles - All act as knee flexors - All have ischial tuberosity origin - All cross 2 joints (prone to straining) |
|
|
What function do the muscles of the medial thigh compartment have?
|

Hip adductors |
|
|
What is a common source of pain in the groin?
|
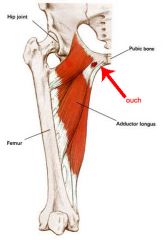
The bony attachment of the medial thigh muscles at the pubis can often become inflamed and cause pain |
|
|
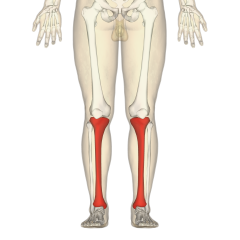
Which bone of the leg is more medial? |
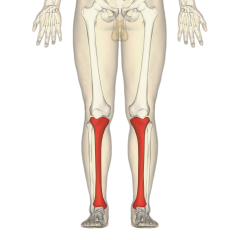
The tibia
|
|
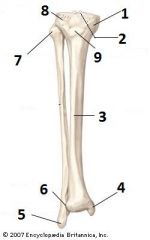
Label pls |
1. Medial condyle of tibia 2. Tibial plateau 3. Shaft of tibia 4. Medial malleolus 5. Lateral malleolus 6. Trochlear notch 7. Styloid process of fibula 8. Lateral condyle of tibia 9. Tibial tuberosity |
|
|
Which is the main, weight bearing, articular bone in the lower leg? What is the purpose of the other bone in the lower leg? |
The tibia bears the weight.
The fibula serves as a point of muscle attachment. |
|
|
What is the purpose of the tibial tuberosity? |

It gives attachment for the patellar ligament
|
|
|
What structure do the medial malleolus, lateral malleolus and the trochlear notch form? |
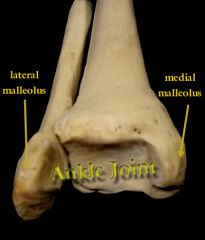
The roof of the ankle joint
|
|

Label 1, 2, 8 & 9 What are the structures 1 - 7 collectively called |
1. Talus
2. Calcaneus 8. Metatarsals 9. Phalanges 1 - 7. Tarsal Bones |
|
|
How many tarsal bones are there? Are the tarsal bones heavier or lighter than the carpal bones? |
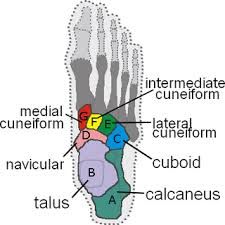
7 Tarsal Bones.
They are heavier than the carpal bones as they bear more weight. |
|
|
What structure(s) does the line of gravity pass in front of in the lower limb? Behind of? What anatomical structures resists this line of gravity? |
Pass in front of: 1. Knee (resisted by posterior capsule) 2. Ankle (resisted by calf muscles, esp. Soleus) Pass behind of: 1. Hip joint (resisted by anterior capsule) |
|
|
What are the 2 main functions of the hip joint? |
1. Weight transfer
2. Content protection |
|
|
What are the 3 joints of the pelvic girdle? Which types of joints are they respectively? |

1. Sacroiliac joint
- Synovial plane joint 2. Scarococcygeal joint - Cartilagenous joint 3. Pubic Symphisis - Cartilagenous joint |
|
|
What is the purpose of the ligament of the head of femur? |
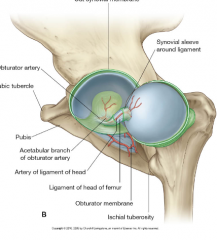
It is an inctracapsular ligament that attaches the femur to the acetabulum
|
|
|
What are the 2 main ligaments which stabilise the hip joint? How does their structure relate to function? |
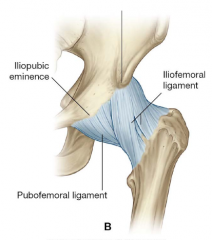
1. Iliofemoral ligament 2. Pubofemoral ligament They both have a spiral orientation of fibres which allows tightening of the ligament during hip extension, pulling the head of femur back in to the socket |
|
|
What are the 2 possible injuries to the hip joint? Give details |
1. Fractured neck of femur - Blood vessels anastamose on the femoral head hence fracture can lead to avascular necrosis of that region 2. Traumatic dislocation of hip - Joint capsule can unwind during flexion - This means it is susceptible to dislocation - Sciatic nerve can tear during posterior dislocation |
|
|
What are the 2 joints found in the knee? When are the ligaments of this region most taut? |
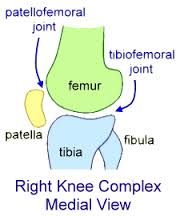
1. Tibiofemoral Joint
2. Patellofemoral joint Ligaments provide most support during knee extension |
|
|
What are the menisci? What 2 functions do they serve? Which meniscus is connected to the its corresponding collateral ligament? |
The menisci are fibrocartilage discs found in the knee joint between femure and tibia - Semilunar and wedge shaped Serve to: 1. Act as shock absorbers (increase articular area of contact by 1/3) 2. Distribute synovial fluid The medial meniscus is adherent to the medial collateral ligament (MCL) |
|
|
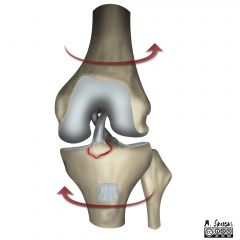
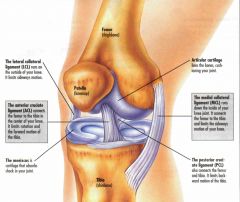
Where does the anterior cruciate ligament (ACL) attach? What function does is serve? |

Attaches on the anterior tibia and posterior femur
- Provides stability in saggital plane by preventing tibia from slipping forward |
|
|
Where does the posterior cruciate ligament (PCL) attach? What function does is serve? |

Attaches on the posterior tibia and anterior femur
- Provides stability in the saggital plane by preventing tibia from slipping backward |
|
|
Which cruciate ligament of the knee is weaker and more susceptible to injury? |
The anterior cruciate ligament (ACL)
|
|
|
Are the cruciate ligaments of the knee intracapsular or extracapsular? What about the collateral ligaments of the knee? |
Cruciate ligaments = intracapsular Collateral ligaments = extracapsular |
|
|
Out of either the medial or lateral collateral ligament, which one: 1. Is rounded and narrow? 2. Is adherent to its corresponding meniscus? 3. Is adherent to its joint capsule? 4. Resists 'varus' stress (as opposed to valgus)? 5. Is less mobile? 6. Has a tibial attachment (as opposed to fibular attachment)? |
1. The LCL is rounded and narrow whereas the MCL is flat and broad 2. The MCL is attached to the medial meniscus whereas the LCL is separate from the lateral 3. The MCL is adherent to its joint capsule whereas the LCL is separate 4. The LCL resists varus stress whereas the MCL resists valgus stress 5. The MCL is less mobile 6. The MCL has a tibial attachment whereas the LCL has a fibular attachment |
|
|
What is the function of the collateral ligaments of the knee? When is their function optimised? |
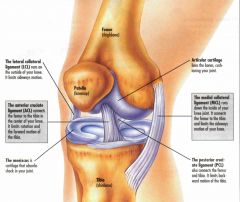
Allow mediolateral (side to side) stability => Most stable in knee extension |
|
|
What is the difference between a prepatellar and suprapetellar bursa? |
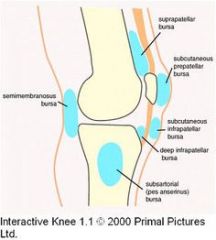
As suprapatellar bursa are in front and above the the patella, they are continuous with the synovial joint cavity, meaning inflammation of the knee can cause suprapatellar bursa swelling. |
|
|
What are the 2 types of common knee joint injury? Give details... |
1. Patellar Dislocation - More commonly a dislocation from the lateral side as the femur is angulated and thus the lateral aspect bears more weight 2. "Unhappy Triad" Injury - Injury to i) ACL ii) MCL iii) Medial Meniscus - Not uncommon for all to be torn at the same time - Typically due to some excessive form of knee rotation |
|
|
What type of joint is the superior tibiofibular joint? What about the inferior? Is ligamentous support for these joints strong or weak? |
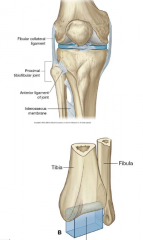
Superior = plane synovial joint Inferior = (fibrous) syndesmosis joint Both have very strong ligamentous support |
|
|
What type of joint is the talocrural joint? What bones form the joint? What movements are allowed at this joint? |
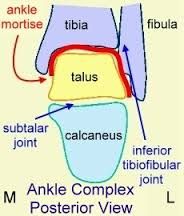
- Hinge type synovial joint
- Formed by 'malleolar matrix' (2 malleoli + articular surface of tibia) and articular surface of talus - Allows plantar (true) flexion and dorsi flexion (extension) |
|
|
What 2 ligament/ligament groups support the talocrural joint? |
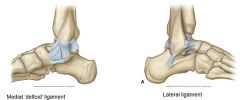
1. Medial 'deltoid' ligaments
- Strong triangle of ligaments which are rarely injured 2. Lateral ligaments - Not as strong (prone to sprain) - 3 separate ligaments (inferior, posterior, anterior) |
|
|
What bones form the subtalar joint? What movements does this joint allow? |
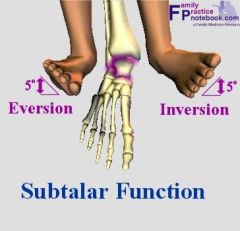
Formed by the talus and calcaneus => Allows inversion and eversion of foot |
|
|
What is the 'fascia lata'? Where does it originate and attach? |
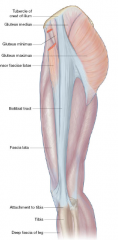
The fascia lata is the deep fascia of the thigh Origin = Tubercle of iliac crest Insertion = Lateral tibia |
|
|
What is the iliotibial band?
What function can it serve? |

The iliotibial band is a lateral thickening of the fascia lata which can be weight bearing when standing up |
|
|
What are the 3 muscle compartments of the leg? What are the generalised functions of the muscles in each? |
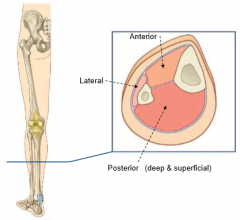
1. Anterior - Ankle dorsi-flexors - Toe extensors 2. Lateral - Ankle plantar-flexors 3. Posterior - Ankle everters |
|
|
What are the 3 muscles in the anterior compartment of the leg? What injury can occur from overuse of these muscles? What injury can occur from swelling of this region? |

1. Tibalis anterior 2. Extensor hallucis longus (EHL) 3. Extensor digitorum longus (EDL) Overuse can cause tenoperiostosis (shin splints) As the deep fascia of this region are tight, swelling in this area can compress neurovascular structures (fasciotomy needed to decompress) |
|
|
What are the 2 muscles in the lateral compartment of the leg? How can they prevent ankle sprains? |
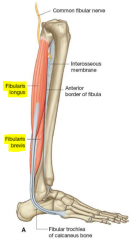
1. Fibularis Longus 2. Fibularis Brevis Have a proprioceptive role in ankle movements (help stability) as to prevent spraining |
|
|
What are the 3 muscles in the superficial, posterior compartment of the leg? Which muscles provide power (as opposed to postural) roles? |
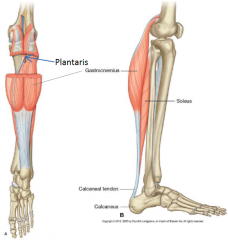
1. Gastrocnemius
2. Plantaris 3. Soleus Gastrocnemius has a power movement role whereas the rest are more postural |
|
|
Which muscle in the leg does the venous sinus run through?
|
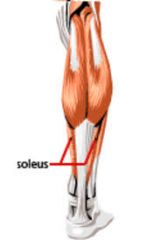
Venous sinuses found within the soleus muscle (superficial, anterior compartment) |
|
|
What is the achilles tendon? |
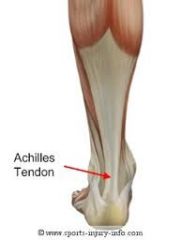
Tendon that attaches the superficial, posterior leg muscles (gastrocnemius, soleus & plantaris) to the calcaneus in the foot
=> prone to tendinitis |
|
|
What structures do 'hallucis' muscles work on? |
The big toe
=> e.g. extensor hallucis longus |
|
|
Starting from the Common Iliac Artery, what 4 major arteries are found in sequence in the lower limb? |
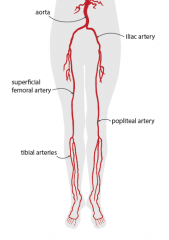
Common Illiac Artery => 1. External Iliac Artery => 2. Femoral Artery (+profunda femoris) => 3. Popliteal Artery => 4. Tibial Arteries (anterior and posterior) |
|
|
What anatomical structure does the external iliac artery pass through? |
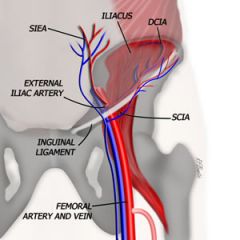
The inguinal canal (formed by inguinal ligament)
|
|
|
What 3 superficial (venous) structures does the blood of the lower limb drain back from? |
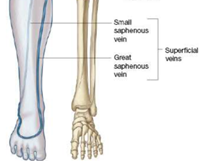
1. Dorsal Venous Arch 2. Greater Saphenous Vein 3. Small Saphenous Vein |
|
|
What are the deep veins of the lower limb named after? |
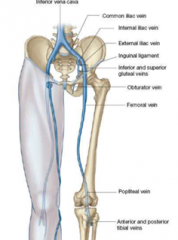
They are named after the artery they run next to
=> e.g. popliteal vein runs alongside the popliteal artery |
|
|
Where do the lymphatics of the lower limb drain back to venous circulation? |

They all drain back to the thoracic duct
|
|
|
Where do the nerves of the lower limb originate from in the spine? What is the plexus that the major nerves come from? |
They all come from the anterior rami of spinal nerves. Come from the 'lumbosacral plexus' |
|
|
For the femoral nerve: 1. What spinal nerves does it arise from? 2. What muscles does it supply? 3. What skin areas does it supply? 4. What structure does it pass through? 5. What clinical signicance does it have? |

1. L2 - L4 2. Anterior thigh muscles (extensors) 3. Anterior thigh and medial leg + foot 4. Passes through inguinal canal 5. Not much => rarely injured except through direct trauma |
|
|
For the obturator nerve: 1. What spinal nerves does it arise from? 2. What muscles does it supply? 3. What skin areas does it supply? 4. What structure does it pass through? 5. What clinical signicance does it have? |
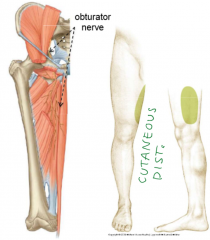
1. L2 - L4 2. Medial thigh muscles (adductors) 3. Medial thigh skin 4. Passes through obturator foramen 5. Can have referred pain from the ovary when it swells and can refer hip pain to the knee |
|
|
For the gluteal nerve: 1. What spinal nerves does it arise from? 2. What muscles does it supply? 3. What skin areas does it supply? 4. What structure does it pass through? 5. What clinical signicance does it have? |
1. L4 - S1 2. Lateral thigh muscles (gluteal) 3. None 4. Greater sciatic foramen 5. None |
|
|
For the sciatic nerve: 1. What spinal nerves does it arise from? 2. What muscles does it supply? 3. What skin areas does it supply? 4. What nerves does it split in to? 5. What clinical signicance does it have? |
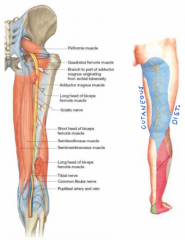
1. L4 - S3 2. Posterior thigh muscles (flexors) 3. Posterior thigh and leg skin 4. Tibial nerve and fibular nerve 5. Must be avoided when gluteal injections are made in the buttocks. Also disc prolapse as L5/S1 can cause nerve root irritation |
|
|
For the tibial nerve: 1. What spinal nerves does it arise from? 2. What muscles does it supply? 3. What structure does it pass through? 4. What clinical signicance does it have? |

1. L5 - S3 2. Posterior leg muscles (everters) 3. Passes the tarsal tunnel to form the plantar nerves 4. Compression of tibial nerve in the tarsal tunnel can cause tarsal tunnel syndrome. Also plantar nerve compression can cause 'jogger's foot' |
|
|
For the fibular (peroneal) nerve: 1. What spinal nerves does it arise from? 2. What muscles does it supply? 3. What clinical signicance does it have? |

1. L4 - S2 2. Superficial fibular = lateral leg muscles (plantar flexors) Deep fibular = anterior leg muscles (dorsi flexors) 3. Compression of peronal nerve can cause 'foot drop' or 'anterior compartment syndrome' if deep nerves compressed. |
|
|
What are the 3 layers that surround the lumen of hollow viscera (deep to superficial)? What are their respective functions? |
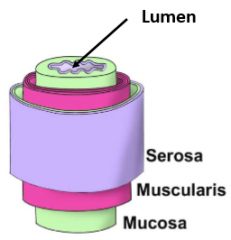
1. Muscosa => Mainly folds of epithelium for absorption 2. Muscularis => Contains smooth muscle for contraction 3. Serosa => Minimises friction |
|
|
How is the smooth muscle of the visceral muscularis layer organised? What function does this allow? |
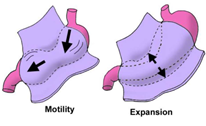
The smooth muscle is arranged circularly and longitudinally
=> Allows motility (e.g. peristalsis) => Allows expansion without changind force of contraction (storage then secretion of liquids or solids) |
|
|
Where does the lumen of hollow viscera usually dilate or constrict? |
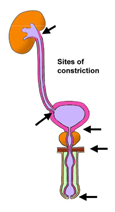
1. Beginning
2. End 3. Other specific sites |
|
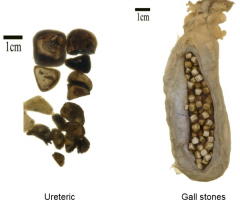
Where are calculi (i.e. ureteric and gall stones) likely to lodge? |
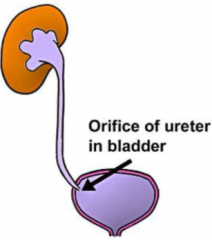
Likely to lodge in the orifice of the ureter and bladder (hollow tube tends to narrow here) |
|
|
What is the difference between an anatomical and functional sphincter? Give examples of each. |
Anatomical - Localised muscle thickening around wall of tubular viscus controls passage of contents - Can be involuntary (1st line of defense) or involuntary (2nd line of defense) - e.g. Anal sphincter Functional - No localised muscle thickening - Control of tubular contents depend on relationship with surrounding structures which can close it off - e.g. Urethral spincter |
|
|
What is the difference between and endocrine and exocrine gland? Give an example of each. |
Endocrine - Secretion of hormones in to blood stream for circulation - e.g. Adrenal glands Exocrine - Secretion of hormones in to ducts directed at specific structures - e.g. Liver and Bile ducts *Some glands can be both exocrine and endocrine (e.g. pancreas) |
|
|
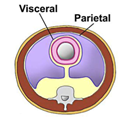
What are the 2 layers of serous membrane? What structures do they respectively cover? Where do they respectively receive their neurovascular supply? |
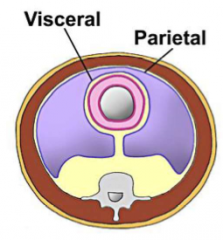
1. Parietal Layer - Lines body wall => receives nerve and blood supply from wall 2. Visceral Layer - Lines viscera => receives nerve and blood supply from viscera |
|
|
What is the serous membrane called in: 1. The thoracic cavity? 2. The abdominal cavity? 3. The heart lining? |
1. Pleura
2. Peritoneum 3. Pericardium |
|
|
How does the serous membrane develop to cover a viscera? |
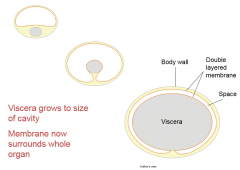
1. Viscera develops in body wall behind a cavity that is lined with cells 2. Viscera invaginates in to cavity and is surrounded by those cells 3. Viscera enlarges 4. Cavity becomes filled with serous fluid |
|
|
What are the 2 functions of serous membranes? |
1. Reduces friction (serous fluid in between parietal and visceral layers) 2. Allows limited movement (connected by mesentery) |
|
|
What is a mesentery? What 2 functions does it serve? |

A mesentery is a fold or stalk of serous membrane that connects viscera to the body wall 1. Allows restrained mobility of viscera 2. Provides a pathway for nerves and vessels |
|
|
What is the clinical difference between paired viscera and unpaired viscera? |
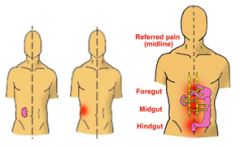
The paired viscera receive individual branches of nerve and blood supply on both sides => Pain on a given side will only present on that side Unpaired viscera often cross the midline and receive nerve and blood supply from both sides => Pain in unpaired viscera will usually be referred to the midline as sensory nerve supply from both sides will reach spinal cord simultaneously |
|
|
What is meant by referred pain? |
The perception of pain in regions other than the actual site of stimulation.
Sensory nerves enter the spinal cord via the same afferent pathway and the brain sometimes cannot differentiate the source of stimulation. Visceral pain is usually referred to somatic regions. |
|
|
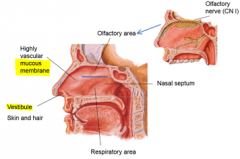
What are the 3 functions of the nasal cavity? |
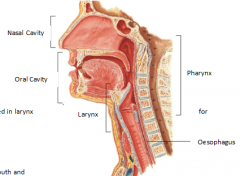
1. Smell
2. Airway passage (breathing) 3. Resonance for sound |
|
|
What are the 3 functions of the oral cavity? |
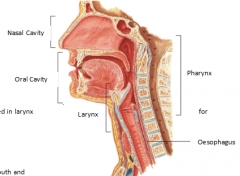
1. Eating 2. Talking 3. Airway passage (breathing) |
|
|
What are the 2 functions of the larynx? |
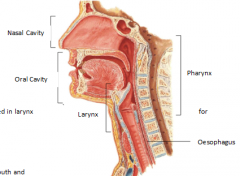
1. Airway passage (breathing)
2. Assists in phonation |
|
|
What are the 2 functions of the pharynx? |
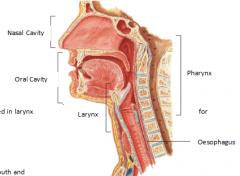
1. Swallowing
2. Has immune tissue |
|
|
Why is the mucous membrane of the nasal cavity highly vascular? |
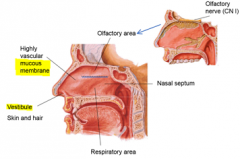
Blood vessels warm up the air for entry in to the respiratory tract |
|
|
What area of the upper respiratory tract is used for olfaction? |
The upper 3rd of the nasal cavity |
|
|
What is the nasal septum? |
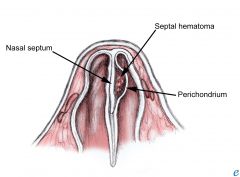
Cartilage running along the midline of the nasal cavity that divides the left and right airways
|
|
|
What specialised structures may be found in the respiratory area of the nasal cavity? |
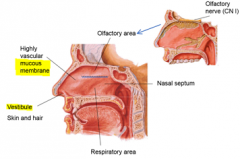
Ciliated epithelium line the mucous membrane, moving mucus in to the back of throat
|
|
|
What is the nasal vestibule? |
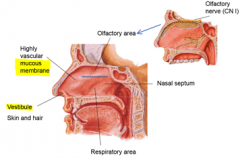
The most anterior (entrance) part of the nasal cavity. It is lined with skin and hair which filter out large dust particles from entering. |
|
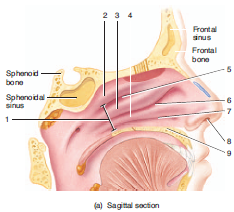
Label this |
1. Concha
2. Superior concha 3. Middle concha 4. Inferior concha 5. Superior meatus 6. Middle meatus 7. Inferior meatus 8. Vestibule 9. Hard palate |
|
|
What are the nasal concha/turbinates? What is their function? |
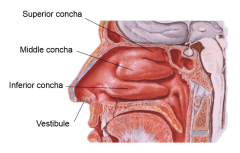
Facial bones which extend horizontally along the lateral wall of the nasal cavity (superior, middle and inferior).
Serve to increase turbulance in nasal cavity, thus warming the incoming air before descending into lower respiratory tract. |
|
|
What are the meatus of the nasal cavity? |
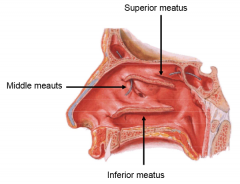
The narrow passageways or spaces located underneath their corresponding concha
|
|
|
What are the 4 paranasal sinuses? Which sinuses are most prone to infection and why? |
1. Frontal 2. Ethmoid 3. Sphenoid 4. Maxillary Maxillary is most likely to be infected at it level and continuous with the nasal cavity meaning mucus and bacterial build up is easy. Frontal and ethmoid are both superior to the nasal cavity and thus drain easily. |
|
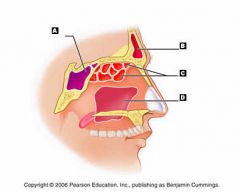
Lbl |
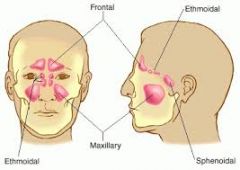
A. Sphenoid sinus B. Frontal sinus C. Ethmoid sinus D. Maxillary sinus |
|
|
Where does the auditory (eustachian) tube enter the nasal cavity? What does this opening allow? |
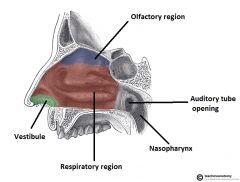
Enters the nasal cavity posteriorly on the lateral wall
Allows the middle ear to equilibriate with atmospheric pressure |
|
|
What are the 2 functions of the lips? |
1. Speaking
2. Food/liquid manipulation |
|
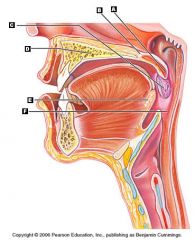
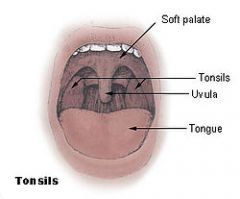
You know what to do |
A. Uvula B. Soft palate C. Palantine tonsil D. Hard palate (maxilla + palantine) E. Lingual tonsil F. Oropharynx |
|
|
What are the 2 divisions of the hard palate? |
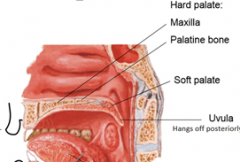
1. Maxilla (anterior) 2. Palantine bone (posterior) |
|
|
What is the uvula? Function? |
Posterior, conic projection of the soft palate (dangly bit at the back of mouth).
Can manipulate sounds |
|
|
What are the 3 functions of the tongue? |
1. Shapes bolus of food
2. Speech manipulation 3. Taste |
|
|
What is the function of the tonsils? What tonsils are found in the oropharynx? What about the nasopharynx? |
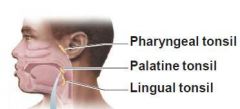
They are collections of lymph tissue (immune function)
Oropharynx = Palantine + Lingual Nasopharynx = Pharyngeal |
|
|
What divides the anterior 2/3rd and posterior 1/3rd of the tongue? |
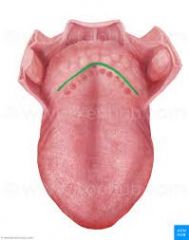
The sulcus terminalis |
|
|
What are the 4 forms of papillae found on the tongue? Which are surrounded by taste buds? |

1. Fungiform 2. Foliate 3. Vallate 4. Filiform All are surrounded by taste buds except filiform which covers the majority of tongue (functions to grip bolus) |
|
|
What difference in function do the extrinsic and intrinsic muscles of the tongue have? |
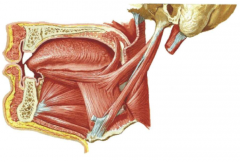
Extrinsic - Alter position of tongue
Intrinsic - Alter shape of tongue |
|
|
What are the 4 types of teeth that we have? What function does each serve? |
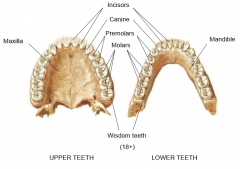
1. Insicors - Shearing 2. Canines - Anchoring food 3. Premolars - Grinding 4. Molars - Grinding |
|
|
What are the 4 main pieces of cartilage that form the larynx?
What are their respective functions? |
1. Epiglottis
=> pulled down by muscles during swallowing to close pathway to trachea 2. Thyroid cartilage => protection of vocal folds 3. Cricoid cartilage => complete ring of cartilage that provides attachment point for muscles/ligaments used in speech production 4. Arytenoid cartilage => provides attachment for vocal ligaments |
|
|
What is the function of the vocal ligaments and vocal folds? When are the ligaments abducted, and when are they adducted? |
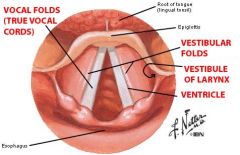
Intrinsic muscle of the larynx pull on the vocal ligaments and the vocal folds (muscosal flaps), causing them to vibrate and produce sounds. Ligament abducted during inspiration and adducted during phonation. |
|
|
What are the 3 segments of the pharnyx? |
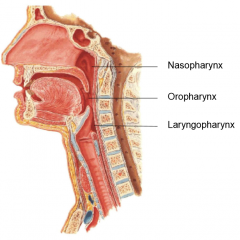
1. Nasopharynx 2. Oropharynx 3. Laryngopharynx |
|
|
What is the function of vestibular folds? |
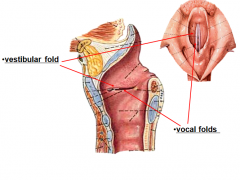
They are thick flaps of mucosa which sit superior to the vocal folds, serving to protect them (no direct role in phonation) |
|
|
What function do the constrictor muscles of the pharynx have? |
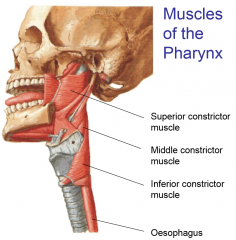
They contract sequentially to allow swallowing |