![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
|
Small Bowel Ileus |
Temporary cessation in peristalsis. Most common causes is surgery, but other causes are drugs (Opiates), electrolyte abnormalities, infections.
Need to distinguish from SBO/partial SBO which can be done with abdominal CT and/or upper GI contrast study
Management is supportive with IV fluids. Can try erythromycin (No evidence it works) |
|
|
Unique physical exam finding in Polymyositis |
Mechanics Hand (Hyperkeratotic eruptions over finger pads) Polymyositis also causes ILD, and can affect the diaphragm leading to aspiration, breathing difficulties |
|
|
Causes of AFIB |
P: Pulm Embolism I: Ischemia R: rheumatic heart ds A: Atrial Myxoma, Old Age, anemia T: hyrotoxicosis, toxins E: EtOH, electrolytes S: Sepsis, stimulants |
|
|
May Turner Syndrome |
Iliac Vein Compression Syndrome (Left iliac vein is compressed by right iliac artery Can explain multiple DVT in left leg when hypercoaguable work up is negative |
|
|
Goal of Uric acid Level in gout |
< 6.0 (Losartan is only BP medication that also lowers uric acid level) |
|
|
Hypothyroidism vs Hyperthyroidism myositis differential |
in hyper, CK will be slightly elevated or normal because muscle is already burned out In Hypo, will have very high CK levesl |
|
|
Which area of lung does IPF effect? |
Lower lobes |
|
|
Which area of lung does silicosis effect |
Upper lobe |
|
|
When to treat assymptomatic bacturia and first line treatmnet |
Pregnant women or patients that are undergoing aggresive urological procedures (TURP) Nitrofurontoin |
|
|
first line treatment of pyelonephritis |
Cipro |
|
|
Renal Mass Cut off for intervention |
>3cm need to be removed, less than 3 can be observed |
|
|
Cyclin D1 Overexpression |
seen in mantle cell lymphoma |
|
|
Babesiosis
|
Tick borne disease transmitted from ixodes tick; Sx: High fevers (104), malaise, jaundice, arthralgia, anorexia, abdominal pain SEVERE CASES: DIC, ARDS Pathogenesis: infects RBC leading to hemolytic anemia which can damage kidneys, spleen filters infected RBCs leading to hypersplenism Labs: hemolytic anemia, transaminitis, elevated alk phos, thrombocytopenia Diagnosis: peripheral smear showing parasitemia and occasionally maltese cross Tmnt: Atovaquone + Azithromycin for mild Clindamycin IV + quinine for severe infections ****Always suspect coinfection with Lymes/Anaplasmosis |
|
|
Alcohols with gaps
|
All alcohols cause osmolar gap Isopropyl Alcohol -> metabolized to acetone (Only Osmolar Gap) Methanol -> metabolized to formic acid (Osmolar/Anion gap) Ethylene Glycol -> metabolized to oxalic acid (Osmolar/Anion Gap) |
|
|
Toxoplasmosis pathogenesis and presentation |
Acquired by eating undercooked meats (Pork,Beef) or exposure to cat feces which contain the parasite. Ingested as cysts, and our digestive enzymes break down the cysts, releasing the parasite which disseminates throughout body (Mostly in lymph and CNS) leading to multiple ring enhancing lesions. Immune competent host: Usually assymptomatic Immunocompromised: Headache, meningitis/encephalitis type picture ***Almost always a reactivation disease so IgG almost always positive and during acute reactivation IgM will be negative. |
|
|
CNS infections/manifestations in AIDS patients |
Toxo, CNS Lymphoma, HSV encephalitis Cryptococcal meningitis, PML |
|
|
Treatments/Ppx for Toxoplasmosis |
Treatments is with Permethermine w/Folinic Acid and Sulfadiazine ppx with Bactrim when CD4 <100 |
|
|
Monocular Diplopia |
Occurs when one eye is covered and one eye is not. Indicates malingering vs corneal abrasion vs cataract vs lense dislocation vs abducense nerve palsy and is nothing to be concerned about |
|
|
Binocular Diploplia |
Diploplia occurs when both eyes are open and improves when one eye is covered and is due to disruption of of ocular alignment Should ask if diplopia is side by side or vertical (images are side by side or on top of one another) |
|
|
Causes of binocular Diplopia |
Infectious, Inflammatory, Restrictive, Neurologic, Neoplastic, Metabolic Restrictive: Something prevents movement of globe such as infection, tumor, thyroid disease. Will need high res imaging of orbit (MRI) Myethenia Gravis: Many cases are limited to ocular in nature and patients will complain of blurry vision and can have ptosis. Pupils will always be normal. Can check acetylcholine receptor Ab or MUSK Ab but can be negative. Edrophonium test in eye can confirm. **Botulism from food or wound can mimic ocular myesthenia When restrictive diseases and mysthenia ruled out, will need to suspect CN involvement
CN 3: Ptosis (Levator palpebrae), dilated pupil (iris sphincter) with eye "down and out" because lateral rectus is unopposed **If visual fields are normal it rules out retina or optic nerve problem and indicates problem with muscle |
|
|
Clostridium Botulinum |
Anaerobe that causes disease by ingesting toxins in food or if spores get into a wound and produce the toxin which transmission of Ach. Clinical symptoms: Cranial Nerve palsies Diplopia, ptosis, facial paralysis, descending paralysis, respiratory failure (4 D diploplia, dysarthria, dysphonia, dysphagia) Need to ask about recent wounds and if they prepare home canned foods Diagnosis: Clinical, myesthenia, Gillen barre are on differential, Eaton Lambert Treatment: Botulism anti-toxin |
|
|
BK Virus |
Polyoma virus that can damage kidneys of immunosuppressed patients leading to nephritis and will see decoy cells in urine. |
|
|
Ronchi |
indicates secretions in bronchial airway |
|
|
Cryptococcosis |
Type of fungus found in pacific northwest that can lead do infection through inhalation. In immunocompetent hosts there is usually no diseae, but in immunosuppressed will usually cause meningitis and sometimes pneumonia/ skin involvement |
|
|
Clinical Manifestations of Cryptococococsis |
Meningitis: Headache, Fever, lethargy, CN palsies Lung: fever, chills, sputum production Skin: papules,plaques, purpura, vesicles (Can look like moluscum contagiosum |
|
|
Diagnosis of cryptococcosis and treatment |
CSF: India Ink Stain Treatment: Amphotericin and Flucytosine |
|
|
Coccidiomycosis |
Fungus found in southwest that presents as a PNA after inhalation of mold. Will have sputum production, pleurtic chest pain, night sweats, arthralgias and skin rash **will often have peripheral eosinophila |
|
|
Seretonin Syndrome vs Neuroleptic Malignant Syndrome |
Seretonin syndrome leads to hyperreflexia, tremor, myoclonus where NMS patients are rigid. Pupils are usually dilated in seretonin syndrome but not NMS. |
|
|
arterial vs venous ulcerations |
venous is medial Arterial is distal by feet and lateral malleolus |
|
|
lactic adisosis types |
Type A - Tissue Hypoperfusion Type B - mitochondrial dysfunction (Metformin, Propofol) Type D - bacterial overgrowth in patients with short bowel syndrome (Will have anion gap but falsely negative lactate) |
|
|
anterior mediastinum masses |
Thyomoma, Teratoma, Terrible Lymphoma, Thyroid |
|
|
visual field deficity chart |

|
|
|
imagine and labs for diplopia |
CTA head and neck to rule out stroke, aneurysm MRI of orbit to rule out mass, infection of orbit ANA, ANCA, RF, ESR, CRP, SS-A/SS-B can also consider LP if all unremarkable |
|
|
Treatment for Colon Cancer? |
FOLFOX Folinic Acid (Fol) Flurouracil (F) Oxaliplatin (Ox) |
|
|
Folinic Acid |
Derivative of tetrahydrofolic acid which does not require action of dihydrofolate reductase to become active and has equivalant activity of folic acid. Uses: 1) Rescue agent from methotrexate (rescues bone marrow and GI mucosa 2) Chemo agent (Used with Fluorouracil to enhance it's effects) 3) Can be given with antibiotics that are dihydrofolate reductase inhibitors (Trimethoprim and Pyrimethamine) |
|
|
A-a gradient calculation |
150 (Inspired partial pressure of Oxygen) - paCO2 / 0.8 Normal A-a gradient 5-10 Causes of elevated A-a gradient: V/Q mismatch diffusion limitation shunt (Cardiac or pulmonary) |
|
|
Drugs that prolong QtC |
1) Anti-arrythmics (Except lidocaine), 2) Zofran (Use prochlorperazine /Reglan instead) 3) Fluoroquinolones/Macrolides, 4) Methadone/Oxycodone (Use Morphine instead) 5) Antifungals 6) AntiPsychotics: Haldol (high risk), Geodon (some risk), Can Use Abilify instead
|
|
|
QTc calculation |
QT (In ms) / Square root of RR (In seconds) Men: 360 - 440 Women: 360 -460 |
|
|
Metocloperamide |
Dopamine blocker used for GI dysmotility, headaches, nausea. Side effects include akathesia (Restlessness), hyperprolactenemia, agranulocytosis, NMS, Tardive Dyskinesia |
|
|
Extrapyramidal Disorders |
Movement disorders (Hyper or hypokinesis) due to derangements of basal ganglia (Caudate nucleus, Putamen, Substantia Nigra) |
|
|
Dystonia |
Movement disorder leading to sustained muscle contractions (ie torticollis) from infection, medication (Dopamine blocker) etc Tmnt is IM benadryl |
|
|
Tardive Dyskinesia |
Specific type of movement disorder that leads to choreoathetoid of the limbs (involontary twisting and writhing) Caused by anti-psychotics at either high doses or chronic use. |
|
|
Neuroleptic Malignant Syndrome |
complication of neuroleptics that lead to fever, rigidity, AMS, hyporeflexia and autonomic symptoms. Usually occurs within 1-2 days of treatment but can come on at any time. Treatment is mainly supportive. Low threshold for intubation, and Dantroline is TOC. |
|
|
Wellens Syndrome |
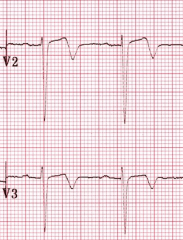
Deeply inverted or biphasic T wave in V2-V3 which is specific for critical stenosis in LAD
***Usually start out biphasic and eventually transition to inverted Well IN.....in 3 2 go
|
|
|
Intravascular vs extravascular hemolysis |
Intravascular is due to mechanical damage or complement mediated Extravascular is due to coating of RBC w/Ab or having an abnormal shape leading to hemolysis in liver or spleen (ITP, AIHA, |
|
|
Coombs Test Direct and Indirect |
Coombs test is used when you suspect hemolysis in Ab mediated (Warm autoimmune hemolytic anemia) Direct: used when Ab is on surface of RBC Patient's RBC is washed and placed in test tube with anti-human globulin (antibody against an Ab) If positive agglutination will take place. Indirect: When Ab is not on surface of RBC, but rather floating around in plasma(Pregnancy and blood transfusions) Place lab RBC with an Antigen the suspected Ab reacts to in patient serum. Then add Antibody to see if agglutination takes place. |
|
|
Leprosy clinical features |
hypopigmented hypoesthetic macules (Leprosy affects peripheral nerves) Treat with Dapsone |
|
|
Examples of positive direct coombs test |
When immune mediated hemolytic anemia is suspected 1) Hemolytic Disease of Newborn 2) Drug induced Autoimmune hemolytic anemia (Methyldopa, Pennicillin) 3) Warm/Cold agglutinins |
|
|
Causes of warm autoimmune hemolytic anemia |
Idiopathic, drug, SLE, Lymphoma |
|
|
Langerhaan Cell Histiocytosis |
Inflammatory disease seen in smokers due to eosinophil activity where patient's present with cough, dyspnea, weight loss and associated with pneumothorax. Chest CT will show nodular opacities and thin walled cysts in upper lobes (Nick Langer is high off alcohol) Tmnt: Smoking Cesssation |
|
|
lymphangiomyomatosis |
Lung disease affecting women of child bearing age due to proliferation of smooth muscle around lympatics and airway leading to multiple cysts. Proliferation of smoothe muscle is thought to be exacerbated by estrogen. Patients present with SOB, PTX, chylothorax Treated with Sirolimus which is an Mtor inhibitor. |
|
|
Classification of vasculitis |
1) Immune Complex Formation: IgA vasculitis, SLE vasculitis, Hep B/C vasculitis 2) ANCA Mediated: Granulomatosis w/Polyangitis, Churgg-Strauss, Microscopic Polyangitis 3) T-Lymphocyte Mediated: Giant Cell Arteritis, Takayasu Arteritis, |
|
|
Immune Complex Mediated Vasculitis mechanism and examples |
IgA Vasculitis, Lupus vasculitis, Hep B/C
Antigen/Ab complex deposits within vessell wall which then trigger complement activation as well as neutrophil chemotaxis and lead to ischemia of the vessel well as well as the tissue it supplies when intracellular enzymes are lysed |
|
|
When to suspect vasculitis |
palpable purpura, microscopic hematuria, mononeuritis, unexplained ischemic events |
|
|
Polyarteritis Nodosa |
Small and medium vessel vasculitis that usually affects renal vasculature (spares venules) but can effect GI system, CNS, bronchioles (spares pulmonary artery) Strong associated with w/Hep B |
|
|
Lemierre's Syndrome |
Complication of Fusobacterium (Anaerobic Gram negative rod) infection leading to thrombosis of jugular vein with dissemintation of abscess (septic emboli) into throat, chest and mediastinum, liver) Patient presents with high fevers, neck throat pain and respiratory distress Treat with clindamycin |
|
|
Type of enema contraindicated in dialysis patients |
Fleet's enema because of phosphate |
|
|
alkalosis and calcium levels |
Alkalosis causes increased binding of calcium to albumin which can lower available levels |
|
|
cyanide poisoning |
Can occur in fires (burning of plastics). Inhibits mitochondrial transport chain and tissues are not able to extract oxygen. smetabolically active tissues (Brain) are most susceptible. Tmnt: Nitrites and sodium thiosulfate, Nitrites create methyhemoglobin which has higher affinity to cyanide than cytochrome system. This can create a dangerous level of methemoglobin so sodium thiosulfate is given to get rid of methemoglobin. ***Cautious in patients exposed to fire Sodium thiosulfate can be given alone Hydroxycobalamin has recently been approved as antidote |
|
|
Parapneumonic effusions |
Effusions that form in pleural space associated with PNA 1) Uncomplicated: No bacteria in pleural space 2) Complicated parapneumonic effusion: Occurs when bacteria migrates into pleural space 3) Empyema: Pus in bacterial space When patient has pleural effusion from PNA that fails to respond to treatment within 48 hours will need to get a thoracentesis to assess pH, glucose, cell count, protein, ldh, |
|
|
differentials in guillain barre |
polio, West Nile Virus, critical care myopathy, lyme polyradiculitis, porphyria, vasculitis, mysethenia |
|
|
Why is there a narrow anion gap in multiple myeloma |
myeloma has increased proteins which are positively charged (immunoglobulins) which in turn cause an increase in absorption of chloride and leads to decreased gap |
|
|
Anion Gap |
The difference between anions and cations. Unmeasured cations: K,Mg, Ca Unmeasured anions: Phosphates,Sulfates, Albumin In an elevated gap acidosis, acids are generated which dissociate into H (which consumes a HCO3) and into their respective anions to replace HCO3 |
|
|
duration of AC in bioprosthetic heart valve? |
3 months |
|
|
Treatment in anticholinergic activity? |
Physostigmine |
|
|
Side effects of Linelozid |
Seretonin syndrome, neuropathy, thrombocytopenia |
|
|
best test to assess respiratory status in guillain barre patients? |
Vital Capacity |
|
|
best test for west nile virus? |
IgM or IgG titers, NOT PCR |
|
|
anticholinergic syndrome |
From Atropine, Anti-histamines, TCAs
Sx: Dry mouth (Dry as a bone), AMS (Mad as a Hatter), Flushed (Red as a beet), decreased urination (Full as a flask) Temperature (Hot as a hare), tachycardic, dilated pupils
Tmnt: Physostigmine
Pfizer makes antidote Pfizer big famous company Johnny Depp as mad hatter is big famous actor |
|

|
Ecythema Gangrenosum 2/2 pseudomonas bacteremia usually in neutropenic patients |
|
|
Barret's Esophagus management |
If low grade dysplasia can watch it, if high grade dysplasia will need endoscopic ablation |
|
|
How to diagnose Insulinoma if CT negative |
Endoscopic US |
|
|
Collagenous Colitis |
AKA Microscopid Collitis Type of microscopic colitis where patients present with watery diarrhea Asssociated with PPI, NSAIDs, SSRIs. Diagnosed by colonoscopy (normal appearing colon,) biopsy will show mononuclear infiltrates Initial treatment is bismuth/loperamide. If failed will need Budesonide. |
|
|
Dyspepsia |
epigastric pain (burning), early satiety, **Different than heartburn which is a retrosternal burning |
|
|
Monocyte |
Type of WBC that can differentiate into macrophage. If you see a lot of monocytes on smear clarify with pathologist as they can be misread as atypical lymph or blast cell |
|
|
chloroma |
solid tumor consisting of myeloblasts seen in AML. |
|
|
carcinomatous Meningitis |
Occurs when tumor cells infiltrate CSF (lung cancer, Leukemia. Patients present with AMS, seizures, cranial nerve pathology, hemiparesis, dysphagia. Need MRI and LP. LP shows elevated protein ???? |
|
|
RP relationships in ECG |
Can be used to help define narrow complex tachycardias. RP is from start of QRS to Start of P. If RP is less than 1/2 of RR, it's considered short RP. If RP is 1/2 of RR or more, its considered long. Differentials for short RP are typical AVnRT, and typical AVRT Differentials for long RP are Atach and atypical AVNRT/AVRT |
|
|
fixed splitting of S2 |
Any type of splitting of S2 occurs when the pulmonic and aortic valve close at different times. With an ASD, blood is always flowing from left atria to right atria, and more blood is being delivered to right ventricle, which delays closure of pulmonic valve. So ASD will cause fixe splitting of S2. |
|
|
Significance of ST elevations in V1-V2 |
Can be septal MI or posterior wall MI via circumflex. Get stat echo to evaluate posterior wall. |
|
|
Association with Lichen Planus? |
Hepatocellular Carcinoma |
|
|
DRESS Syndrome |
Drug Reaction with Eosinophila and Systemic Symptoms. Will develop various types of rash within 8 weeks of starting new drug (can be from any drug but sulfa drugs, allopurinol, anticonvulsants are most common) 30% of patients will have peripheral eosinophilia. Can also effect other organs leading to transaminitis, kidney dysfunction. Treatment is stopping medication, antipyretics, systemic steroids if severe (evidence of organ dysfunction) |
|
|
infusion rate for sepsis |
30 cc/kg per hour |
|
|
Differentiation Syndrome |
Occurs when patients with Acute Promyelocytic Leukemia get treated with ATRA. Thought to be related to cytokine overactivation. Symptoms include fever, edema, pulmonary opacities, hypoxia, renal/hepatic dysfunction. People usually die from hypoxic respiratory failure. Treated with steroids. |
|
|
Beri Beri |
Dry: peripheral neuropathy Wet: High output cardiac failure, tachycardia, wide pulse pressure |