Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
49 Cards in this Set
- Front
- Back
|
Sensory Systems: Most Common Changes
-Vision -Hearing -Sensation -Perception |
Vision: 1st noticeable sign of aging
– 19% of 65+ are visually impaired (not completely corrected by glasses/contacts) – equal in men & women Hearing: most well-known change – 33% of 70+ are hearing impaired – more common in men Sensation: Stimulation of sensory cells Perception: interpretation of sensory information taking place in the brain |
|
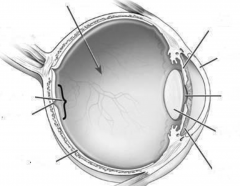
Front of the eye (1-5)
-Sclera |
1) Ciliary Muscles: change the shape of the lens to focus
2) Cornea: protection and outer layer of eye 3) Pupil: controls how much light can pass through 4) Lens: changes the way light enters the eye (curves it) to concentrate at the macula and fovea 5) Iris: Protects structures in the back of the eye from over stimulation -controls pupil and regulates light intake -muscle that is pigmented and gives eye color Sclera: white of eye and major supporting structure (gives spherical shape) |
|
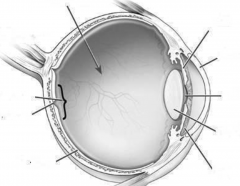
Back of the eye (1-5)
|
1) Vitreous Gel: fills eye but isn't tight (allows for give)
-problematic for glaucoma 2) Optic nerve: takes light info to the brain -no retina in this area= Blind spot 3) Macula- processes light info VERY efficiently -densest cell area 4) Fovea: tiny spot on macula with dense cells 5) Retina: Multilayered tissue that lines the back of the eye and converts light rays into electrical impulses -cells in the retina are called cones and rods More severe changes happen in the back of the eye |
|
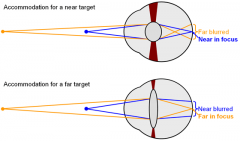
Lens & Accommodation:
-Accommodation -Presbyopia -Distance Accommodation |
-Starts at age 40
-Accommodation: involves the lens changing shape depending on an object’s distance. -Lens loses flexibility with age and accommodation is compromised -Cornea increases in curvature and thickens causing presbyopia -Presbyopia: clearest vision moves farther from the eye because the lens becomes flatter and the ciliary muscles get stiffer causing elders to not focus on near objects -Distance Accommodation: lens/ciliary muscles decline= harder to shift back and forth from near- to far vision (important for driving) |
|
|
Physical Eye Changes and Light Sensitivity:
-floaters |
-Begins in your 50's
-Lens thickens and gets yellow/cloudy (accumulated insoluble proteins) -less light passes through lens -difficulty seeing in dim light = less night driving -sensitive to glare (even at night) -"floaters" (particles of insoluble protein) accumulate in vitreous humor but don't effect vision -Vitreous humor becomes more liquid (from gel) |
|
|
The Retina and Dark Adaption:
-cones -rods -Peripheral Vision |
-In retina called "cells" or "Photo Receptors"
-fewer cells as we age Cones: -Color Vision -Visual Acuity -Densely packed at fovea Rods: -Concentrated in periphery -Low light vision (can still see SHAPE and MOVEMENT) Peripheral Vision: have to turn our heads as we get older -young = 170 degrees -by 50 = 140 degrees |
|
|
Visual Acuity:
-Static -Dynamic |
-Visual acuity is the ability to see fine detail.
-Acuity is much greater at the center of the visual field than it is at the periphery. -Static Acuity: seeing detail in things that are still -Dynamic Acuity: Seeing detail in moving things -Both static and Dynamic decline with age but dynamic declines more |
|
Cataracts
|
-Lens Clouds
-Genetic condition -image cannot focus on retina= blurred vision -treated with surgery |
|

Glaucoma
|
-one of leading causes for blindness
-common in middle & late life -Genetic: Blacks & diabetics -Pressure and fluid build up -creates retinal damage -Periphery is blurred Treatments: -medicated with drops/ marijuana - surgery (only temporary) |
|

Macular Degeneration
|
-Leading cause of blindness
-smoking increases risk -receptor cells in retina deteriorate -dark spots and blurring Treatment: surgery (not easily treated) |
|
|
Retinal Detachment
Retinopathy |
Retinal Detatchment:
-inner and outer layers of the retina separate -Can be surgically reattached Retinopathy: -Small blood vessels that nourish retina do not function properly as a result of diabetes -amendable through laser treatments |
|
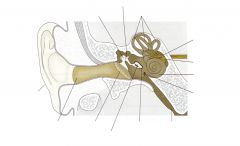
Anatomy of the Ear
|
1) Pinna: The outer ear catches sound wave and directs it into the inner ear to the ear drum (Tympanic Membrane)
2) Tympanic Membrane (Ear Drum): vibrates the Ossicles 3) Ossicles are made up of three bones called the 4) Hammer 5) Anvil and 6) Stirrup which act as levers & push against the Cochlea 7) Cochlea: a snail-shaped, fluid-filled structure. 8) organ of Corti: The tiny hairs in the cochlea turn this pressure into electrical signals, which are then sent to the temporal lobes of the brain. |
|
|
Hearing and sound:
-Vibrations -Pitch -Dog whistle |
-All sounds send out vibrations (sound waves).
-Vibrations occur at various frequencies, not all of which the human ear can hear. -PITCH= frequencies that can be heard range from 20 to 20,000 Hz (Hertz=frequency per sec.) -Dog whistle: 16,000 – 22,000 Hz |
|
|
Effects of aging and Loudness:
-Loudness -Aging effects |
-Loudness= Decibels
-Researchers have found that people are listening to music at very high levels. -sustained exposure to 90-95 dB = hearing loss -One in five listening to MP3 players at 100 dB or higher. -People get louder (decibels) when pitch (frequency) gets higher |
|
|
Dr. Colavita Video:
1) One reason older adults show deficits on hearing tests? 2) role of drugs and noise i hearing loss? can they be reversed? |
1) fear of inaccuracy- older adults will wait to be sure they know the answer, while younger ppl will answer sooner
2) DRUGS: ototoxic, streptomycin, and mycin drugs kill hair cells=hearing damage -NOISE: the amount of hearing loss experienced 5 mins after an 8 hour shift = damage you will sustain permanently if you worked job for 10 years -typical hearing range of an 18yr old = 18,000hZ |
|
|
Hearing Disorders:
1) Otosclerosis 2) Presbycusis 3) Tinnitus |
1) Otosclerosis
-10% of the population -Soft boney growth at foot of stapes in oval window -can occur in only one ear which leads to degenerative changes 2) Presbycusis -Progressive loss of hearing for high frequency tones due to deterioration in inner ear -not solely in industrialized cultures -hair begins to atrophy -treated with hearing aid 3) Tinnitus -Ringing in ears -Injury discharge -aspirin can cause this if taken in large amounts |
|
|
Hearing Disorders:
1) Central Auditory impairment 2) Conductive Loss |
1) Central Auditory impairment:
-difficulty understanding language but can hear external sounds -nerve centers in brain are damaged -there is no cure 2) Conductive Loss: -Blockage of wax, fluid or abnormal bone growth stops sound from traveling -sound seems muffled while ones own voice may sound louder -treated by flushing ear, medication, or surgery |
|
|
Hearing loss:
-gender -speech perception -Hearing aids |
- one of the most frequent chronic conditions in older adults at 28.6% of ppl 65+
-more frequent in men -speech perception: speech by itself does not decline but when speech has to compete with noise in the background there is more significant decline Hearing aids: placed in right ear because it is better at speech detection -talk louder, face them so they can read lips |
|
|
Sense deterioration:
Smell Taste Touch Balance- Thai Chi |
Smell: processed in olfactory bulbs
-shows cell loss with advanced age -decline in ability to detect aromas -may be caused by air pollutants (ex. cigarette smoke) Taste: 4 types of taste buds (sweet, salty, sour, bitter) -# of taste buds decline at 40 b/c rate of replacement decreases -sweet buds most often lost and all buds 2/3 gone by 70 -salvation decreases and gets thicker Touch: declines with age -fewer cells to detect temp. changes and sensations -frequent burns b/c cant detect hot surface fast enough Balance: difficulty maintaining balance -Thai chi practiced to maintain slow movements |
|
|
Slowing:
-3 parts of Response time -Simple reaction time -Choice Reaction Time -Complex Reaction time |
-Slowing: measuring response time
-Response Time: 1) sensory 2) brain processing 3) muscle response -Simple Reaction Time: one stimulus is presented and person makes one response -Choice Reaction Time: 2 stimuli presented and person must respond differently to each -Complex Reaction Time: 2+ stimuli requiring 2+ responses |
|
|
Falling and Time
|
-1/3 of older adults fall because of continued loss of senses and perceptions
-women fall more often than men -can cause breaks and be fatal Time: passes more quickly partially because you don't remember all the events happening through out the day |
|
|
Feats of Memory:
-Akira Haraguchi -Andi Bell -Kim Peek |
- Akira Haraguchi can recite pi from memory to 83,431 decimals.
-Andi Bell can remember the order of 520 playing cards after only 20 minutes of study. -Kim Peek (the real Rain Man) has memorized 7500 books and knows the zip code to every US location. |
|
|
Memory loss with age
|
-Memory complaints become increasingly common in later life (50-80% of people over 60).
-With advancing years, there is loss in certain forms of cognition. -Most older adults equate older age with memory loss |
|
|
Memory loss is inevitable with age?
|
Fiction!
-Not everyone shows the same decline like 1) Individual differences and 2) Successful aging -Not all forms of cognition decline |
|
|
Taxonomy of memory
|
Memory- Short Term/Working or long term
Long term- Procedural or Declarative Declarative- Semantic or episodic |
|
|
Short Term Memory:
-Memory Span -Chunking |
- If you are conscious of something= short-term memory.
-Memory Span: The number of items that can be recalled, in order, after a brief delay. -Chunking: A meaningful group of information that can be stored in STM as one item. Capacity is 7 +/- 2 "chunks" |
|
|
Sensory and Working Memory
|
Sensory Memory:
-different and brief memory for each sense -dissipates rapidly after receiving info (especially with physical decline due to old age) Working memory: -Keep information in mind & actively process it -Limited pool of processing resources that you can allocate to various tasks -Choices must be made when limit is exceeded. |
|
|
Working Memory:
-Operation Span -Reading Span -So What? |
Operation Span: do a equation and if it makes sense asked to remember a word
Reading span: read sentence and if it is coherent, remember the last word of the sentence -Older adults do worse on WM tasks relative to young adults (kids also do poorly b/c their frontal lobes = still developing) -WM is a HUGE predictor of things like writing ability, note taking, complex learning, reasoning, etc. |
|
|
Long Term Memory:
3 types |
LTM: in cerebral cortex
1) Procedural: Knowing "how" • memory for skills & habits; "muscle memory". • often unconscious & difficult to describe in words. 2) Episodic: Knowing "what" • memory for specific, autobiographical events. • accompanied by details about time, place, and event. • "Mental time travel". • things that can be stated or declared. • Most common type of memory impaired in amnesia 3) Semantic: general knowledge and facts that you "know" but can't say where you learned them. |
|
|
Semantic Memory:
1) Association Tasks 2) Lexical Decision 3) Word Finding Task |
1) Association tasks: remember category
Apple is a _______. Linguini is a _________. Basil is a __________. 2) Lexical decision: decide if word stapa stop chup sniff 3) Word finding task: tip-of-the-tongue unusual facts and definitions |
|
|
Episodic Memory:
1) Recall Tasks 2) Recognition Tasks and 2 types of episodic memory |
Recall Task: no memory cues
Recognition Task: Memory cues 1) prospective memory: remembering to do a future behavior such as go to an appointment 2)Retrospective Memory: information that has already occurred that you are trying to remember such as what you did last weekend |
|
|
Memory Systems:
-Encoding -Retrieval |
-Working memory can turn into LTM by engaging in Encoding operations
-Encoding: making information more easily stored through repetition, rehearsal, and pegging -The more this is practiced the easier it is to RETRIEVE the info later -Retrieval process: bring LTM to conscious attention in working memory |
|
|
Working Memory and Aging
|
-does not change with advanced age
-slowing in WM is due to slower info received and processing but not WM itself -processing speed = essential element in observed decline |
|
|
Long Term Memory and Aging:
Experiment 1 |
-Aim: examine age differences in remembering names of unknown & familiar faces & objects
-Experiment 1 -Participants: 24 young (M=23), 24 old adults (M = 70) -Task: 16 pictures of unknown faces with names & occupation so when you see the face, remember name & occupation -What type of memory & task? -Episodic memory, recall task Results: Older adults have poorer episodic memory -Both age groups have more difficulty with names than occupations |
|
|
Long Term Memory and Aging:
Experiment 2 |
-Experiment 2
-Participants: 20 young (M = 21), 20 old (M=67), 20 old-old (M=77) -Task: 36 pictures of familiar faces & 36 familiar objects -When see picture, name person or object -What type of memory & task? -Semantic memory, word-finding task Results: No age differences for remembering familiar objects -Some age differences for remembering familiar faces |
|
|
Long Term Memory and Aging:
Procedural Episodic semantic |
Procedural: remains intact through old age
Episodic: harder to retrieve information because it is poorly encoded semantic: accumulates with age and there is no deficit but creates a wealth of general knowledge |
|
|
Metamemory
|
-"knowledge about ones own memory"
-you can alter how you memorize things by using strengths you find in your own memory -older adults believe their memory declines with age and therefore they score themselves lower on metamemory -2 things affect metamemory: culture/belief about ones own memory and Education |
|
|
Control Versus Automaticity
|
Controlled memory =Significant decline
Auto Memory= little decline |
|
|
Memory improvement
|
-internal mental techniques can help to improve memory -creates reduced anxiety and higher memory recall
-some research suggests it can be improved through pharmacology also - acetylcholine can improve memory as well as ginkgo |
|
|
DRM Effect
|
Deese Roediger-Mcdermott Effect = giving list of word and asking for recall with a lure word (word close to the ones previously listed) to see if a false memory is created
-some older adults are more susceptible to false remembering |
|
|
Intelligence: Sternburgs "What is intelligence"?
-G factor |
When asking laypersons and experts 3 categories were established: 1) problem-solving ability 2) verbal intelligence and 3) social/practical competence
-intelligence: a general proficency in cognitive tasks -G Factor: general and universal (general proficiency) that underlies all intelligence performance |
|
|
Baltes: Dual-component Model of Intelligence
|
-Mechanics (fluid): Basic information processing
-Hardware of the mind -Biologically-dependent -Genetically predisposed -Pragmatics (crystallized): Acquired knowledge -Software (content-rich) -Culture-dependent -Experience-based -Pragmatics build on mechanics and play a bigger role (esp. in learning) -How will each component change across lifespan? declines more in mechanics |
|
|
Cohort Effects on Intelligence: Schaie’s Seattle Longitudinal Study
|
-Aim: to examine age changes in IQ for multiple abilities across multiple cohorts
- Sequential design: • began in 1956… last testing 1998 • participants tested every 7 years (longitudinal) • new group of young adults at each time (cross-sectional) -Participants: •sample of 5000+ from 20s to 100+ •recruited from health insurance (CONFOUND: eliminates lower income participants) •upper 75% of SES Measures: Thurstone’s 5 Primary Mental Abilities |
|
|
Cohort Effects on Intelligence: Schaie’s Seattle Longitudinal Study RESULTS
-terminal drop |
Results:
Cohort: more decline due to cohort rather than age - the older the cohort the lower the score because of newer technological advances -cohorts living longer because of better health -terminal drop: sudden decline in some cognitive abilities shortly before death Longitudinal: mental ability increases until 40 then remains stable until 60's and start to decrease (mostly for mechanics) Cross-sectional: declines more dramatic for mechanics starting at 40 Inter-Individual Variability: everyone shows decline in at least 1 area by 60's but rarely in all 5 even by 80's |
|
|
Thurstone’s 5 Primary Mental Abilities
|
Pragmatics:
1) Verbal Meaning: recognizing and understanding words 2) Number: Applying numeric concepts Mechanics 3) Word Fluency: recalling verbal information from memory 4) spatial orientation: Thinking about and comparing forms 5) Inductive Reasoning: identify regularities and rules |
|
|
Problem Solving: 2 Types
-SOC -Expertise |
1) Abstract: do not deal with concrete objects of real life situations
2) Practical: deal with concrete objects of real life situations -older adults better at solving practical problems -Selection: choosing activity -Optimization: increasing knowledge -Compensation: adapting to the change -Expertise: very high performance in some activity because of genetic and envio. factors (typically in older people b/c they've had a lot of practice) |
|
|
Wisdom: Baltes & Staudinger Model
-5 Criteria of Wisdom -Wisdom |
Personality is thought to be important in development of wisdom
1) Factual Knowledge: fundamentals of life 2) Procedural Knowledge: knowing about strategies and procedures for everyday life 3) Lifespan Contextualism: Knowledge which considers contexts of life and societal change 4) Relativism: considers the relativity of others values and life goals 5) Uncertainty: can recognize and manage life's uncertainties -Wisdom: good judgement and advice in important but uncertain matters of life |
|
|
Baltes & Staudinger 5 Criteria of Wisdom: Experiment
|
-Participants: young (M = 32) & older adults (M = 71)
-½ are clinical psychologist -Methods: give people fictitious life dilemmas -rate responses according to wisdom criteria EXAMPLE: 15 year old wants to get married Result 1: Wisdom is stable across most of adulthood Result 2: Wisdom is related to experience, and age/experience are related |
|
|
Creativity
|
-"newness and difference from the ordinary"
- another aspect of cognition - Exceptional Creativity: creativity of famous people (such as artists) that is recognized by creative professionals -Ordinary Creativity: creativity of those whose work is not recognized -divergent tests: test creativity by forcing you to come up with multiple solutions to a problem -17% of creativity should be produced a decade until 60's -older adults do poorly on divergent test (especially if timed) but are high in creative productivity because they have so much free time -DOES NOT DECLINE WITH AGE |