![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
|
Waldeyers Ring |
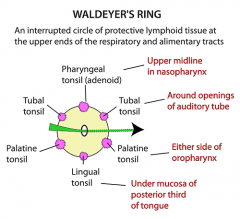
Consists of B-cell lymphocytes, T-cell lymphocytes and some plasma cells |
|
|
Adenoid Self Anatomy |
- Pharyngeal Tonsil, part of Waldeyers ring - Lymphatic tissue covered by respiratory epithelium (pseudostratified columnar) - Non encapsulated, No crypts |
|
|
Adenoid Location |
-Posterior Superior wall of nasopharynx - Anatomical relations: Inferior to sphenoid sinus Anterior to basi-occiput Lateral to lymphoid tissue of Rosenmuller Recess |
|
|
Adenoid Development |
- Small at birth - Enlarge by age 4 - Regress from age 7 to adolescence - Absent in adults |
|
|
Adenoid Function |
To mount an immunologic response against infective agents |
|
|
Adenoid Hypertrophy causes |
- Usually they enlarge and regress after infection subsides - May stay enlarged in the case of chronic infection, or chronic allergies. |
|
|
Adenoid Hypertrophy: Clinical Presentation & Features |
- Noisy breathing - Nasal obstruction --> (OSA in severe cases) - Mouth breathing --> (drying of throat -->Chest infection) -Repeated URTI, rhinosinusitis and OM - Hyponasal speech |
|
|
Adenoid Face |
- Dull/Stupid looking - Flattened Nose - Open mouth - Protruding Upper insisor teeth & Malocclusion of upper jaw - High arched palate |
|
|
Adenoid Hypertrophy: Adverse effects |
- Nasal Obstruction - Pharyngitis (due to dry mouth) - OSA - Rhinosinusitis - Recurrent URTI - OM |
|
|
Adenoid Hypertrophy: Diagnosis |
- Usually not seen during routine examination of nose and throat - Nasal Endoscopy - Mirror Examination - Lateral soft tissue X-ray (rarely needed now) |
|
|
Adenoid Hypertrophy: Treatment |
- Antibiotics (in acute infection) - Adenoidectomy |
|
|
Adenoidectomy Indications |
No absolute indications Relative indications: - Persistent rhinitis that doesnt respont to medical TT - OSA - OM with effusion, that recurs even after grommet |
|
|
Adenoidectomy Procedure & Post-Op Complications |
Procedure - Under GA with endotracheal Intubation Complications -Hemorrhage: Primary (1st 24h) or Secondary (5-10d due to premature separation of eschar/scab) -OM - Regrowth of residual adenoid tissue - Rhinolalia aperta: hyponasal speech disorder |
|
|
Tonsils: Anatomy |
- Palatine tonsils - Deep crypts lined with antigen processing squamous epithelium - They also harbor debris & bacteria --> (halitosis & tonsilloliths) |
|
|
Tonsils: Location |
- In lateral wall of oropharynx within tonsillar fossa - Tonsillar fossa: Palatoglossus (anterior pillar) Palatopharyngeal (post pillar) Superior constrictor (base) - There is potential space between tonsil and pharyngeal muscles --> site of peritonsilar abscess |
|
|
Tonsils: Innervation & Lymphatic drainage |
Innervation: Tonsillar branch of Glossopharyngeal nr --->(also supplies middle ear, so referred pain) Lymphatic drainage: Tonsillar LN Jugulodigastric LN |
|
|
Acute Tonsilitis: Etiology |
Viral: (most common) - Adenovirus, Rhinovirus, Influenza Bacterial: GABHS (most common), S.aureus, strep pneumonia, mycoplasma, chalmydia |
|
|
Acute Tonsilitis: Pathophysiology |
Initial infection may be viral, then bacterial takes over. |
|
|
Acute Tonsilitis: Symptoms |
- Sorethroat - Dysphagia/Refusal to eat - Earache (referred) - Headache & malaise |
|
|
Acute Tonsilitis: Signs |
- Tonsils: hyperemic, enlarged, may exude pus - Pharynx: red, inflamed - Foetor (bad breath) - Cervical LN: Enlarged & Tender |