![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
|
5 static postural deviations |
1. Ankle pronation/supination 2. Hip adduction 3. Anterior/posterior pelvic tilting 4. Shoulder position & thoracic spine 5. Head position |
|
|
What is the effect on posture if the subtalar joint is pronated? |
- the foot is everted - internal rotation of the tibia - internal rotation of the femur - anterior tilting of pelvis |
|
|
What is the effect on posture if the subtalar joint is supinated? |
- inversion of the foot - external rotation of the tibia - external rotation of the femur - posterior tilting of pelvis |
|
|
Effect of hip adduction on posture? |
Right hip: ▪right hip is higher than that of left (posterior view) ▪hips usually shift right (plumb line view)
- Progressively lengthens & weakens right hip abductors - May be caused by limb length discrepancy - Can be caused by sleeping on one side |
|
|
Describe anterior pelvic tilting |
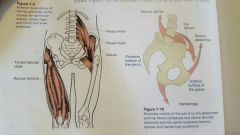
▪hips tilted forward (spill water out the front), anterior & superior portion of hips are pulled forward & down ▪tight hip flexors coupled with tight erector spinae
- causes increase in lordosis - foot pronation may cause anterior pelvic tilting to better accommodate (internally rotated) head of femur - common in sedentary individuals that sit a lot |
|
|
Describe posterior pelvic tilting |
▪hips tilted backward (spill water out the back), posterior & superior portion of hips are pulled backward & down ▪tight rectus abdominis coupled with tight hamstrings - causes decrease in lordosis (flat lower back) - foot supination may cause anterior pelvic tilting to better accommodate (externally rotated) head of femur femur |
|
|
Scapular movements: Elevation Depression Adduction (retraction) Abduction (protraction) Upward rotation Downward rotation |
|
|
|
What is winged scapula? |
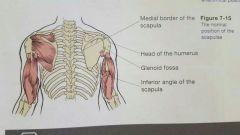
Protrusion of the inferior angle and medial border of the scapula outward |
|
|
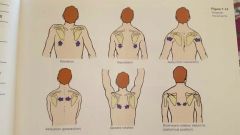
Describe scapular protraction |
▪shoulders are rounded in a forward position (sagittal view) ▪protrusion of medial border of scapula
- palms face backwards instead of to the sides (frontal plane) 》this could also indicate internally rotated humerus - tight serratus anterior, anterior scapular humeral muscles, upper trapezius |
|
|
Ways to view forward head position |
▪in sagittal view (plumb line on AC joint), the earlobe appears farther forward than the AC joint ▪Place thumb on superior sternum and index finger on chin. Pushing head forward reduces space between the fingers ▪Place index finger of one hand on collar bone below the cheek, other index finger on cheekbone below the eye. Fingers should be vertically aligned. |
|
|
5 primary movements of ADL |
1. Bending/lifting 2. Single-leg 3. Pushing 4. Pulling 5. Rotation |
|
|
Explain the general characteristics and observations of the "Bend and Lift Screen" |
- feet shoulder width apart - dowels next to the outside of each foot - ask client to bend and pick up dowels with a 2 second pause before lifting
OBSERVATIONS: - stability of foot (pronation, eversion, heel lifting off floor) - alignment of knees over second toe - glute or quadricep dominance - achievement of parallel between tibia and torso - degree of lordosis in lumbar/thoracic spine when lowering - changes in head position during lowering |
|
|
Lumbar dominance during a squat |
Hip flexors & erector spinae pull pelvis forward during squat. Implies a lack of abdominal and glute strength. The individual experiences excessive loads in the lumbar spine. Tight hip flexors from sedentary lifestyle may contribute to this. |
|
|
Glute dominance during squat |
Initiated by pushing hips backward in hip-hinge movement. Maximizes eccentric loading of glutes to increase concentric force. Preferred method of squatting - reduces stress on lumbar spine and knees. |
|
|
Quadriceps dominance during a squat |
Initiates squat by driving the knees forward. Glutes can't generate much force. Adds stress and pressure to knees, specifically ACL (anterior cruciate ligament) |
|
|
Explain the general characteristics and observations of the "Hurdle Step Screen" |
Client holds a dowel across back of shoulders, steps over string (positioned over halfway up tibia) and places heel of foot on floor, return foot to starting position. Perform on both sides. OBSERVATIONS: - stability of foot (pronation, eversion, etc) - alignment of stance-leg knee over foot - hip adduction >2" add measured by excessive stance-leg adduction or downward hip-tilting toward opposite side - Alignment of moving leg |
|
|
Explain the general characteristics and observations of the "Shoulder Push Stabalization Screen" |
Client should perform push-ups in proper form OBSERVATIONS - changes in scapula position at top and bottom of pushup - lumbar hyperextension during press (weak abdominals) |
|
|
Explain the general characteristics and observations of the "Thoracic Spine Mobility Screen" |
- sit on edge of chair, ball or block between knees, feet on floor, holds dowel horizontally in front of shoulders - squeeze block, gently rotate right and left without any bouncing to end-ROM OBSERVATIONS - discrepancies between rotations in each direction - any vertical tilting of dowel should be avoided |
|
|
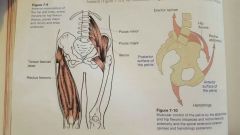
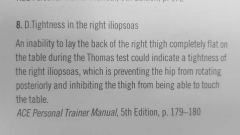
Describe the Thomas Test and it's observations |
▪measures the length of hip flexors and rectus femoris ▪do not perform if patient suffers low back pain ▪client sits on table with edge at mid thigh, lay back and bring both knees up, clasp hands behind knee and bring it towards the chest, slowly lower the other leg and allow it to hang freely off the edge of the table Observations - whether the back of the lower thigh touches the table (10 degrees of hip extension) - weather the day of the Lord like achieves 80 degrees of flexion - whether the lowered knee rotates internally or externally |
|
|
PSL Raise |
Passive straight leg raise ▪have client lay on their back, place one hand under lower back and other under calf of testing leg, slowly raise leg keeping knee extended until firm pressure on hand from low back is felt <80° movement indicates tight hamstrings |
|
|
Describe the Shoulder Flexion and Extension Test |
Flexion ▪client lies on back with bent knees and arms at their sides, raise both arms overhead until they reach the floor above their head (or not), maintain neutral lumbar spine ▪170-180° good mobility Extension ▪client lays on stomach with arms at their sides, raise arms off the floor behind them, don't raise chest or head ▪50-60° off floor good mobility |
|
|
Describe the Internal and External Rotation test |
Internal ▪client lies on back with arms stretched perpendicular to torso, bend arms 90° so fingers are pointed to ceiling, rotate arms to hands decend to the floor towards the feet ▪70° towards mat good mobility External ▪same as internal, but hands rotate toward the mat near the head ▪touch the floor good mobility |
|
|
Describe the Stork-Stand Balance Test |
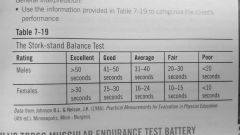
▪remove shoes and hands on hips, bring one foot to the inside of the stance leg below the knee, lift heel off floor to balance on ball of foot ▪3 trials per leg, record best time |
|
|
Three exercises of McGill's Torso Muscular Endurance Test Battery |
- trunk flexor - trunk lateral - trunk extensor |
|
|
Describe Apley's Scratch Test |
Shoulder flexion, external rotation, & scapular abduction ▪client in seated position, reach arm overhead and slide hand down the spine, palm facing spine ▪can touch medial border of opposite scapula - good mobility Shoulder extension, internal rotation, & scapular adduction ▪reach hand behind back, palm facing out, slide hand up spine ▪touch inferior angle of opposite scapula - good mobility |
|
|
Describe the Sharpened Romberg Test |
▪remove shoes, stand heel-to-toe, cross arms in front of chest, close eyes and maintain balance with good control, perform twice on both sides and take the best time ▪<30 sec poor balance |
|
|
Describe the Trunk Flexor Endurance Test |
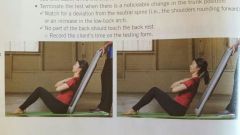
▪sit with hips and knees at 90 degree angle, arms crossed over the chest, lean against the board placed at a 60 degree angle, can anchor or stabilize the feet ▪ remove the board, client is to hold this position with neutral spine for as long as possible, record the time ▪ contraindications: low back pain, recent back surgery, acute low back flare up |
|
|
Describe the trunk lateral endurance test |
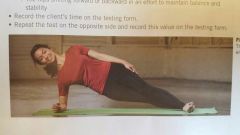
▪ perform a side bridge on the elbow, client should hold this as long as possible without breaking the position, record the time on both sides ▪ contraindications: shoulder pain, low back pain, recent back surgery, low back flare up |
|
|
Describe the trunk extensor endurance test |
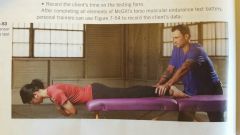
▪Client lays prone with hips on the edge of the table, holds trunk at horizontal position for as long as possible , trainer should hold feet to the table, record time ▪ contraindications: major strength deficiencies , client with high body mass (Trainer unable to securely hold client), low back pain, recent back surgery, acute low back flare up |
|
|
Good ratios for torso endurance test battery 1. Flexion:extension 2. R side bridge:L side bridge 3. R+L side bridge:extension |
1. <1.0 2. 0.95-1.05 3. <0.75 |
|
|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|

|
|
|
|
|
|
During a static postural assessment, in which plane of movement does the personal trainer view the client's balanced resting posture between the anterior and posterior sides of the body? A. Frontal B. Sagittal C. Coronal D. Transverse |
|
|
|
Which of the following responses correctly describes the phenomenon called "winged scapulae"? A. A protrusion of the inferior angle and vertebral (medial) border of the scapula B. A protrusion of the vertebral border outward C. A protrusion of the superior angle and spine of the scapula D. A protrusion of the inferior angle and glenohumeral (lateral) border of the scapula |
|
|
|
Which of the following observations would NOT be noted as a postural deviation? A. The palms of the hands face backward B. The superior, anterior portion of the pelvis rotates downward and forward C. The cheek bone is in line with the collarbone D. The subtalar joint is in pronation |
|
|
|
Which of the following posture postural deviations could indicate that a client has an internally (medially) rotated humerus and/or scapular protraction? A. Front view: Palms face backward B. Posterior view: scapular winging visible C. Side view: upper back has an exaggerated curve D. Front view: sternum not in line with Plumb line |
|
|
|
The client should be referred to his or her physician if which of the following is found during assessments? A. Lordosis during postural screening B. The lack of foot stability with the ankle collapsing inward C. Pain during the bend and lift screen D. Forward head position during postural screening |
|
|
|
During the bend and lift screen, which observation would indicate that the client has tight plantar flexors? A. hamstrings touch the calves B. Squat initiated at knees C. The big toes extend upward D. Heels rise off the floor |
|
|

|
Quadriceps and hip flexor dominance |
|
|
Rectus abdominis and hip extensors |
|

|
Rectus femoris |
|

|
Client displayed inability to internally rotate the forearm 70 degrees toward the mat |
|

|
The client exceeds 30 seconds with good postural control |
|
|
Good |
|
|
Shoulder flexion-extension test and internal-external rotation test of the humerus |
|

|
Anterior view: backs of the hands are visible |
|
|
The coupling relationship between tight _______ and _______ is defined as the lower-cross syndrome. A. Rectus abdominis; hamstrings B. Hip flexors; erector spinae C. Rectus abdominis; erector spinae |
B. Hip flexors; erector spinae |
|
|
Structural deviations |
|
|
False |
|
|
Forces internal rotation of the tibia and slightly less internal rotation of the femur |
|
|
Trunk flexor endurance test |
|
|
True |
|
|
Scapular protraction |