Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
6 Cards in this Set
- Front
- Back
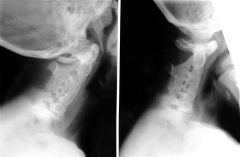
10yo M in Fig wishes to participate in junior football. C spine CT scan in Fig C, renal evaluation-unilateral renal aplasia, and cardiac evaluation is nl. What is Dx & the corresponding medical clearance decision for playing football?
|

1-Klippel-Feil synd w/no participation in contact sports
2-Down's synd w/no participation in contact sports 3-Holt-Oram synd w/no participation in contact sports 4-Down's synd w/full participation in contact sports 5-Klippel-Feil synd w/full participation in contact sports only following skeletal maturity::: congenital cervical fusion of cervical vertebra triad=low, posterior hairline, a short neck, and limited neck motion. Klippel-Feil w/ C spine fusions > C3 should not participate in contact sports. It is critical that patients undergo a cardiac and renal evaluation upon their diagnosis to look for cardiac septal defects and several different types of renal anomalies.Ans 1 |
|

35 yo M s/p MVA and sustains the neck inj Fig, PE = w/ Brown-Sequard SCI. Which represents the motor & sensory findings? 1-b/l UE loss of motor & unilateral LE loss of pain & temp; 2-b/l loss of motor func & unilateral loss of pain and temp 3-Ipsi loss of motor & contra-lat loss of pain & temp; 4-b/l loss of pain & temp & unilateral loss of motor func 5-ipsi loss of pain & temp & contra-latloss of motor func
|
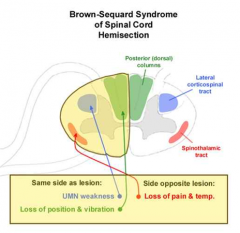
ipsilat motor deficit & loss of SOAP
Sequard-contralateral/Opposite Pain And Temp SAOP Ans3 |
|
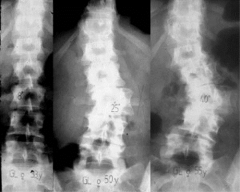
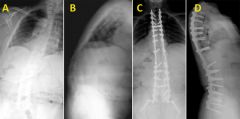
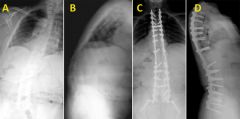
53 yo F is seen in the adult spine clinic for long-standing LBP. Hx untreated scoli as a child. Her xrays Fig A & B. Due to discomfort w/ ADLs & progressive pain, surgical intervention is planned. Which of the following factors would increase her risk of nonunion?
|

1-ant thoracoabdominal apprch; 2-Preop Cobb angle of 60 deg; 3-Age > 35 yrs; 4-A pos midline apprch; 5-Pos sagittal balance < 5 cm::: a thoracoabdominal approach > rates of PSeudoArthrosis/PSA vs post proced, risk factor for PSA=smoking, kyphosis >20 deg, (+) sagittal balance >5cm, preexisting hip arthritis, age >55, and a throacoabdominal approach.Ans1
|
|
In pts w/ adult scoli requiring long thoracolumbar fusns, which of the following is the major advan of extending the fusn to the sacrum as opposed to ending at L5? 1-Improved function outcomes; 2- Dec pseudoarthosis rates; 3-Dec major medical complic
4-Improved correction & maintenance of sagittal balance; 5-Improved curve correction in the coronal plane |
pt fused to the sacrum also had an > rate of pseudoarthosis, major medical complic, improved correction & maintenance of their sagittal balance.Ans4v,
|
|

adult pts w/ scoli, severity of sx correlates w/ which of the following variables? 1-Coronal imbalance; 2-Sagittal imbalance; 3-Magnitude of coronal Cobb angle 4-# of spine levels involved in the deformity; 5-Level of the apex of the curve
|

Sagittal balance is the most reliable xray predictor of clinical health status in adults with spinal deformity, As the C7 plumb line deviation inc, poorer results were found in all measures of health status, lumbar kyphosis had > disability compared to controls.Ans2
|
|

13 yo B is brought to your office because his mother is concerned about his poor posture. A lat xray shows thoracic kyphosis of 38 degrees. This likely represents: 1-Nl range of thoracic kyphosis; 2-Adolescent idiopathic scoli; Scheuerman's kyphosis; 4-Pathologic scoli 5-Congenital scoli
|

nl thoracic kyphosis for a growing adolescent is between 20 -40 deg. Any degree of kyphosis at the thoracolumbar or lumbar spine should be considered abnormal. NOT rigid thoracic hyperkyphosis defined by > 45 deg=Scheuermann's Kyphosis, thoracic kyphosis which does NOT correct w/hyperext.Ans1
|