![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
Clinical Psychologists |
These clinicians have earned a doctoral degree in psychology (either a Ph.D., or Doctor ofPhilosophy; a Psy.D., or Doctor of Psychology; or an Ed.D., or Doctor ofEducation) from an accredited college or university. |
|
|
Counseling Psychologists |
These clinicians alsohold doctoral degrees in psychology and have completed graduate trainingpreparing them for careers in college counseling centers and mental healthfacilities. |
|
|
Psychiatrists |
Haveearned a medical degree (M.D.) and completed a residency program in psychiatry. |
|
|
Clinical or Psychiatric Social Workers |
Haveearned a master’s degree in social work (M.S.W.) and use their knowledge ofcommunity agencies and organizations to help people with severe mentaldisorders receive the services they need. |
|
|
Psychoanalysts |
Typicallyare either psychiatrists or psychologists who have completed extensiveadditional training in psychoanalysis. |
|
|
Counselors |
Havetypically earned a master’s degree by completing a graduate program in acounseling field. Counselors work in many settings, including public schools,college testing and counseling centers, and hospitals and health clinics. |
|
|
Psychiatric Nurses |
Typicallyare R.N.s who have completed a master’s program in psychiatric nursing. |
|
|
Psychotherapy |
Astructured form of treatment derived from a psychological framework thatconsists of one or more verbal interactions or treatment sessions between aclient and a therapist. |
|
|
The Biological Perspective |
· Inspiredby scientists and physicians since the time of Hippocrates · Focuseson the biological underpinnings of abnormal behavior and the use ofbiologically based approaches, such as drug therapy, to treat psychologicaldisorders. · Gaverise to the development of the medical model, which remains today a powerfulforce in contemporary understandings of abnormal behavior. |
|
|
The nervous system is made up of |
The _____ is made up of neurons,nerve cells that transmit signals or “messages” throughout the body |
|
|
A neuron is made up of: (3 things) |
Dendrites Axon Terminals These are all parts of... |
|
|
Dendrites |
Theroot-like structures at the ends of neurons that receive messages from otherneurons. |
|
|
Axon |
Thelong, thin part of a neuron along which nerve impulses travel. |
|
|
Terminals |
Thesmall branching structures at the tips of axons. |
|
|
The nervous system main components (3) |
Neurotransmitters, Synapse, Receptor Sites. |
|
|
Neurotransmitters |
Chemicalsubstances that transmit messages from one neuron to another. |
|
|
Synapse |
The junction between one neuron andanother across which neurotransmitters pass. |
|
|
Receptor Site |
A part of a dendrite on a receivingneuron that is structured to receive a neurotransmitter. |
|
|
Medulla |
Anarea of the hindbrain involved in regulation of heartbeat, respiration, andblood pressure. |
|
|
Pons |
Astructure in the hindbrain involved in body movements, attention, sleep, andrespiration. |
|
|
Cerebellum |
A structure in the hindbrain involved in motor behavior, coordination, and balance . |
|
|
Reticular Activating System |
Brainstructure involved in processes of attention, sleep, and arousal. |
|
|
Thalamus |
Astructure in the forebrain involved in relaying sensory information to thecortex and in processes related to sleep and attention. |
|
|
Hypothalamus |
Astructure in the forebrain involved in regulating body temperature, emotion,and motivation. |
|
|
Limbic System |
Agroup of forebrain structures involved in emotional processing, memory, andbasic drives such as hunger, thirst, and aggression. (Thalamus, hypothalamus,amygdala) |
|
|
Basal Ganglia |
Anassemblage of neurons at the base of the forebrain involved in regulatingpostural movements and coordination. |
|
|
Cerebrum |
Thelarge mass of the forebrain, consisting of the two cerebral hemispheres,responsible for higher mental functions. |
|
|
Cerebral Cortex |
Thewrinkled surface area of the cerebrum responsible for processing sensorystimuli and controlling higher mental functions, such as thinking and use oflanguage. |
|
|
Occipital Lobe |
Primarily involved in processing visual stimuli. |
|
|
Temporal Lobe |
Involvedin processing sounds or auditory stimuli. |
|
|
Parietal Lobe |
Involvedin processing sensations of touch, temperature, and pain. |
|
|
Frontal Lobe |
Controlsmuscle movement and includes the prefrontal cortex that regulates higher mentalfunctions such as thinking, problem-solving, and use of language. |
|
|
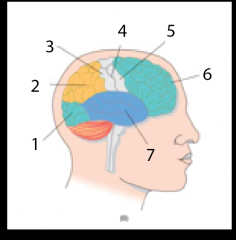
1. Occipital Lobe 2. Parietal Lobe 3. Sensory Area 4. Central Fissure 5. Motor Area 6. Frontal Lobe 7. Temporal Lobe |
|
|
Somatic Nervous System |
The part of the nervous system that relays information from thesense organs to the brain and transmits messages from the brain to the skeletalmuscles. |
|
|
Autonomic Nervous System |
Thedivision of the peripheral nervous system that regulates the activities of theglands and involuntary functions. |
|
|
Sympathetic NS |
Pertainingto the division of the autonomic nervous system whose activity leads to heightenedstates of arousal. |
|
|
Parasympathetic NS |
Pertainingto the division of the autonomic nervous system whose activity reduces statesof arousal and regulates bodily processes that replenish energy reserves. |
|
|
Epigenetics |
Thefield that focuses on how environmental factors influence genetic expression |
|
|
For most disorders, the interaction between what and what needs to be examined? |
genes and environmental factors. nature vs. nurture. |
|
|
Psychopharmacology |
Thefield of study that examines the effects of therapeutic or psychiatric drugs. |
|
|
What percentage of Americans take psychotropic drugs? |
20% - one in five do this. |
|
|
What are the three major classes of psychotropic drugs? |
Antianxiety, antipsychotic, and antidepressants. |
|
|
Examples of antianxiety drugs |
Theyinclude mild tranquilizers, such as diazepam (Valium) and alprazolam (Xanax),as well as hypnotic sedatives, such as triazolam (Halcion). |
|
|
Rebound anxiety |
Theexperiencing of strong anxiety following withdrawal from a tranquilizer. |
|
|
Examples of SSRIs |
fluoxetine(Prozac) and sertraline (Zoloft) |
|
|
Possible side effects of antipsychotic drugs |
muscularrigidity and tremors |
|
|
Antipsychotic drugs |
Canalso be used in some cases to treat mania in bipolar disorder. |
|
|
Lobotomy |
Thisprocedure involved surgically severing nerve pathways linking the thalamus tothe prefrontal lobes of the brain. |
|
|
Psychoanalytic Theory |
Thetheoretical model developed by Sigmund Freud that is based on the belief thatthe roots of psychological problems involve unconscious motives and conflictsthat can be traced back to childhood. – also called psychoanalysis. |
|
|
Conscious |
ToFreud, the part of the mind that corresponds to our present awareness. |
|
|
Preconscious |
ToFreud, the part of the mind that contains memories not in awareness but can bebrought into awareness by focusing attention on them. |
|
|
Unconscious |
ToFreud, the part of the mind that lies outside the range of ordinary awarenessand that contains instinctual urges. |
|
|
Id |
Theoriginal and unconscious psychic structure, present at birth, that containsprimitive instincts and is regulated by the pleasure principle. |
|
|
Pleasure Principle |
Thegoverning principle of the id, involving demands for immediate gratification ofneeds. |
|
|
Ego |
Thepsychic structure governed by the reality principle. It organizes reasonableways of coping with frustration and seeks to curb the demands of the id. –Reality principle – involves considerations of social acceptability andpracticality. |
|
|
Superego |
Thepsychic structure that incorporates the values of the parents and importantothers and functions as a moral conscience. – Serves as a conscience, orinternal moral guardian, that monitors the ego and passes judgment on right andwrong. |
|
|
Defense Mechanisms |
The reality-distorting strategies used by the ego to shield the self from awareness of anxiety-provoking impulses. |
|
|
Freud's five psychosexual stages of development: |
oral (first year of life), anal (secondyear of life), phallic (beginning during the thirdyear of life), latency (from around age 6 to age 12),and genital (beginning in puberty). |
|
|
Fixation |
In Freudian theory, a constellation of personality traits associated with a particular stage of psychosexual development, resulting from either too much or too little gratification at the stage. |
|
|
Psychoanalysis |
The first method of psychotherapy developed by Sigmund Freud. Helps individuals gain insight into, and resolve,unconscious conflicts. |
|
|
Free Association |
The method of verbalizing thoughts as they occur without a conscious attempt to edit or censure them. |
|
|
Inpsychoanalytic theory, dreams have two levels of content: |
Manifest content, and latent content |
|
|
Manifest Content |
The material of the dream the dreamerexperiences and reports. |
|
|
Latent Content |
Theunconscious material the dream symbolizes or represents. |
|
|
Freud believed that dreams were the ____________. |
Royal road to the unconscious. |
|
|
Transference Relationship |
Inpsychoanalysis, the client’s transfer or generalization to the analyst offeelings and attitudes the client holds toward important figures in his or herlife. |
|
|
Countertransference |
Inpsychoanalysis, the transfer of feelings or attitudes that the analyst holdstoward other persons in her or his life onto the client. |
|
|
Behaviorism |
Theschool of psychology that defines psychology as the study of observablebehavior and that focuses on the role of learning in explaining behavior. |
|
|
Conditioned Response |
Inclassical conditioning, a learned response to a previously neutral stimulus. (Salivation in response to the bell after learned) |
|
|
Unconditioned Stimulus |
Astimulus that elicits an unlearned response. (like the food) |
|
|
Unconditioned Response |
Anunlearned response. (salivation at site of food) |
|
|
Conditioned Stimulus |
Apreviously neutral stimulus that evokes a conditioned response after repeatedpairings with an unconditioned stimulus that had previously evoked thatresponse. (the bell) |
|
|
Classical Conditioning |
Aform of learning in which a response to one stimulus can be made to occur toanother stimulus by pairing or associating the two stimuli. |
|
|
Operant Conditioning |
Aform of learning in which behavior is acquired and strengthened when it isreinforced. |
|
|
Reinforcement |
Changesin the environment (stimuli) that increase the frequency of the precedingbehavior. |
|
|
Negative Reinforcers |
Reinforcersthat, when removed, increase the frequency of the preceding behavior. |
|
|
Punishment |
Reduces the frequency of the behavior it follows. |
|
|
Positive Reinforcers |
Reinforcersthat, when introduced, increase the frequency of the preceding behavior. |
|
|
Social Cognitive Theory |
Alearning-based theory that emphasizes observational learning and incorporates roles for cognitive variables in determining behavior. |
|
|
Modeling |
Learningby observing and imitating the behavior of others. Abehavior therapy technique for helping an individual acquire a target behaviorby observing a therapist or another individual demonstrate the behavior andthen imitating it. |
|
|
Expectancies |
Beliefsabout expected outcomes. |
|
|
Behavioral Therapy |
Thesystematic application of the principles of learning to treat psychologicaldisorders. |
|
|
Systematic Desensitization |
Abehavior therapy technique for overcoming phobias by means of exposure toprogressively more fearful stimuli while one remains deeply relaxed. |
|
|
Gradual Exposure |
Abehavior therapy technique for overcoming fears through direct exposure toincreasingly fearful stimuli. |
|
|
Token Economy |
Behavioraltreatment program in which a controlled environment is constructed such thatpeople are reinforced for desired behaviors by receiving tokens that may beexchanged for desired rewards. |
|
|
Self-Actualization |
In humanistic psychology, the tendency to strive to become all that one iscapable of being. The motive that drives one to reach one’s full potential andexpress one’s unique capabilities. |
|
|
Unconditional Positive Regard |
Valuingother people as having basic worth regardless of their behavior at a particulartime. |
|
|
Conditional Positive Regard |
Valuingother people on the basis of whether their behavior meets one’s approval. |
|
|
Humanistic Therapy |
A focus on what clients are experiencing in the present—the here andnow. Person-centered therapy (also calledclient-centered therapy), which was developed by the psychologist Carl Rogers. |
|
|
Person-Centered Therapy |
The establishment of a warm, acceptingtherapeutic relationship that frees clients to engage in self-exploration andachieve self-acceptance. |
|
|
Cognitive Theory/Models |
The study of cognitions—the thoughts, beliefs, expectations, andattitudes—that accompany and may underlie abnormal behavior. Our interpretations of the events in our lives,and not the events themselves, determine our emotional states. |
|
|
Information-processing models |
theoristsdiscuss human cognition in terms such as input (sensory and perceptual processes), manipulation (interpreting orprocessing), storage (placing information inmemory), retrieval (accessing information from memory), and output (acting on the information). |
|
|
Albert Ellis |
Creator of the ABC Approach |
|
|
What are the ABCs of the ABC Approach? |
A - Activating event B - beliefs/ interpretations - mediators C - Consequences |
|
|
REBT - Rational Emotive Behavioral Therapy |
Atherapeutic approach that focuses on helping clients replace irrational,maladaptive beliefs with alternative, more adaptive beliefs. |
|
|
Fourbasic types of cognitive distortions |
1.Selective abstraction 2.Overgeneralization 3.Magnification 4.Absolutist thinking |
|
|
Cognitive Behavioral Therapy |
Alearning-based approach to therapy incorporating cognitive and behavioraltechniques. Tointegrate therapeutic techniques that help individuals make changes not only intheir overt behavior but also in their underlying thoughts, beliefs, andattitudes. |
|
|
The social causation model |
Thebelief that social stressors, such as poverty, account for the greater risk ofsevere psychological disorders among people of lower socioeconomic status. |
|
|
Downward Drift Hypothesis |
Thetheory that explains the linkage between low socioeconomic status and behaviorproblems by suggesting that problem behaviors lead people to drift downward insocial status. |
|
|
TheBiopsychosocial Perspective |
This perspective examinesthe contributions of multiple factors representing biological, psychological,and sociocultural domains, as well as their interactions, in the development ofpsychological disorders. |
|
|
The Diathesis-Stress Model |
Amodel that posits that abnormal behavior problems involve the interaction of avulnerability or predisposition and stressful life events or experiences. |
|
|
Diathesis |
Avulnerability or predisposition to a particular disorder. |
|
|
Eclectic Therapy |
Anapproach to psychotherapy that incorporates principles or techniques fromvarious systems or theories. |
|
|
Nonspecific treatment factors |
Factorsnot specific to any one form of psychotherapy, such as therapist attention and support,and creating positive expectancies of change. |