Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
16 Cards in this Set
- Front
- Back
|
Sunscreens
- how do they work? - active ingredients? |
Chemical barriers, which absorb a range of UV wavelengths:
- benzophenones, oxybenzone, dioxybenzone, mexenone absorb both UV A and B - PABA - salicylates - cinnamates Physical barriers reflect most UV radiation (A&B): - titanium dioxide - zinc oxide - magnesium oxide - calcium carbonate - kaolin - talc |
|
|
Can we use sunscreens on small children and babies?
|
AMH: it is safe to put on small areas of skin of babies (e.g. face and hands). However, primary sun protection should be clothing, shade and avoidance of the sun
Use sensitive skin formulas |
|
|
A/Es for sunscreens?
Are some ingredients of sunscreens photosensitising? |
RARE: rash, irritation
** Use physical barrier creams on only small areas of the body as they prevent normal heat loss and persperation (Kay stewart) Some are photosensitising (e.g. PABA) but the risk of A/Es with sunscreen remains RARE. The risk outweighs the benefits. The cancer council advises that there is no scientific evidence that sunscreens have any long term side effects, such as skin cancer. |
|
|
Counselling on sunscreen?
|
1. apply liberally 20 minutes before sun exposure
**Kay stewart suggests 1 teaspoon for each limb and face-neck-ears 2. reapply at least every 2 hours, particularly after swimming, exercise, heavy perspiration, towelling dry 3. Still use other protective measures: hat, glasses, shade - do not use sunscreen to increase time in the sun. |
|
|
What does SPF rating mean?
|
SPF means % UV B penetration
e.g. 15+ means 6% penetration, 30+ means 3% penetration These cannot be used to estimate allowable time of sun exposure!!! (time of year, skin sensitivity, etc) BUT SPF 30+ halves risk of sunburn with 15+ for same exposure time **These tests are done using thick applications (typically 4x most consumers) & does not compensate for rubbing, water immersion or sensitised skin |
|
|
How should sunscreen be chosen? (what considerations)
|
Most important:
1. SPF 30+ (refers to filtering of UV B) 2. BROAD SPECTRUM cover (UV A and B) Also: 1. water resistant: if for 4hrs, means SPF 25+ after 4hrs 2. non-ghosting, spray on, purple for children 3. creams - thicker; lotions - thinner but alcohol based; gels - sometimes alcohol based (drys faster) Also: some, such as SunSense SPF 30+ 100g, are available on RPBS |
|
|
Photosensitisers - list some topical and systemic ones
|
Topical
- coal tar - biocides added to soaps (e.g. triclosan) - retinoids - ambrette (in fragrances) - SOME SUNSCREEN CHEMICALS such as PABA - Benzocaine in solarcaine Systemic - Tetracyclines, Fluroquinolones, griseofulvin, sulfonamides, quinolones - Retinoids - NSAIDs - Amiodarone, thiazides - St John's Wort, antipsychotics |
|
|
Define phototoxicity and photoallergic dermatitis
|

PIC: photoallergic dermatitis
Photoallergic = formation of an antigen by chemical activation of the substance by sunlight. Phototoxic = direct tissue damage by the agent in combination with radiation. |
|
|
How can you tell the difference between phototoxic and photoallergic dermatitis?
|

PIC: phototoxic dermatitis
1. the drug history 2. phototoxicity occurs more quickly while photoallergic reactions occur 1-2 DAYS after exposure to the sun 3. both appear like sunburn, although phototoxic reactions are more likely to cause bullae, vesicles |
|
|
What is the pneumonic for the essentials of diagnosis of malignant melanoma?
|
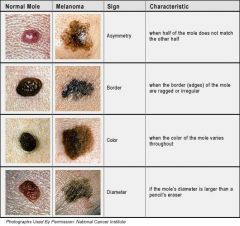
B = border irregularity - often pigment appears to be leaking into surrounding skin
D = diameter >6mm E = evolution E = elevation (almost always present) Occurs most commenly on women's legs and men's torsos - i.e. doesn't neccessarily correlated with area of sun exposure |
|
|
What are other risk factors for melanoma?
|
1. age
2. caucasian skin 3. high number of moles 4. male sex 5. history of sunburn, sun exposure 6. family history 7. systemic immune dysfunction 8. exposure to chemical carcinogens such as tar and chemotherapeutic agents |
|
|
What is a seborrhoeic keratosis?
|

A sun spot
Benign epithelial tumors. Papules or plaques, beige to black, 3–20 mm in diameter, with a velvety or scaley surface. Common—especially in the elderly. |
|
|
what is an actinic keratosis
|
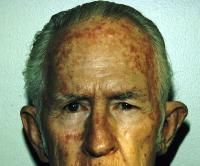
warty, brown/red, scaly, usually flat but can be raised
Can be a precursor to SCC |
|
|
Efudix cream
- indications - cautions, preg - A/Es - dosage - other counselling points |
- cream 5%.20g - RPBS only
- Actinic keratosis only - caution: can worsen inflammatory skin conditions: control first - CI in pregnancy, cat D - Causes local pain, burning, dermatitis, scarring - apply 1-2 times daily for 3-4 weeks; do not treat >500cm2 (cf 25cm2 with aldara) - occassionally an occlusive dressing is also needed - Apply a thin layer using a nonmetal aplicator or glove; avoid contact with eyes, mouth - Your skin will redden, peal, crack - Avoid excess sun exposure |
|
|
Solaraze gel
- instructions |
- apply bd for 2-3 months
- a pea-sized amount is enough for 25cm2, maximum of 8g daily - wash hands |
|
|
Sunburn
- treatment |
- 20 minutes in cold water
- then use hydrogel dressings - some evidence for hydrocortisone cream and anti-inflammatories |